Explain me 10 common heart diseases with ECG changes and ECG image of those diseases
Reading File
Finding Sources
Searching Images
ECG electrocardiogram myocardial infarction ST elevation
Finding Sources
Searching Images
atrial fibrillation ECG irregular rhythm no P waves
Searching Images
heart block complete AV block ECG bradycardia
Searching Images
ventricular tachycardia ECG wide QRS tachycardia
Searching Images
hypertrophic cardiomyopathy ECG left ventricular hypertrophy
Searching Images
pericarditis ECG saddle shaped ST elevation diffuse
Searching Images
Wolff-Parkinson-White syndrome ECG delta wave short PR
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain sinus tachycardia
Searching Images
dilated cardiomyopathy heart failure ECG left bundle branch block LBBB
Searching Images
long QT syndrome Torsades de Pointes ECG polymorphic ventricular tachycardia
Here is a comprehensive guide to 10 common heart diseases, their hallmark ECG changes, and representative ECG images.
10 Common Heart Diseases — ECG Changes & Images
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural myocardial ischemia and necrosis.
Key ECG Changes:
- Hyperacute T waves — earliest sign (tall, peaked, broad-based)
- ST-segment elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in precordial leads; convex ("tombstone") morphology
- Reciprocal ST depression in opposite leads
- Pathological Q waves develop within hours (>40 ms wide, >25% of R-wave height)
- T-wave inversion in the evolution phase
- Localisation by leads: Anterior (V1–V4, LAD), Inferior (II, III, aVF, RCA), Lateral (I, aVL, V5–V6, LCx), Posterior (tall R in V1–V2 with ST depression)

Anterior STEMI: Prominent convex ST elevation across V1–V6 with reciprocal changes in inferior leads. This pattern indicates proximal LAD occlusion.
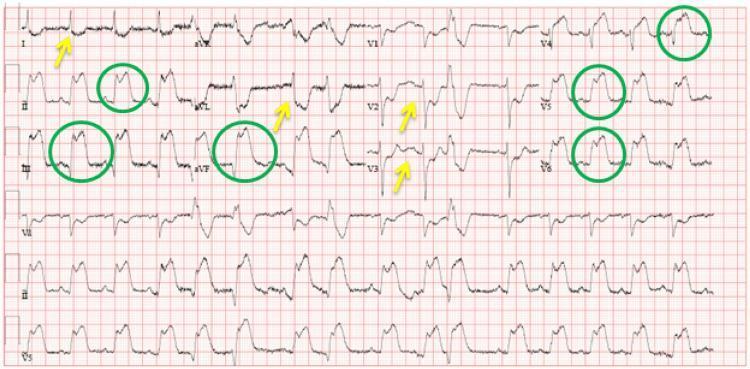
Inferolateral STEMI: ST elevation in II, III, aVF and V4–V6 (green circles) with reciprocal depression in I, aVL, V2–V3 (yellow arrows).
2. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, disorganized electrical activity in the atria produces irregular ventricular response via the AV node.
Key ECG Changes:
- Absent P waves — replaced by fine or coarse fibrillatory (f) waves, best seen in V1 and II
- Irregularly irregular R-R intervals — the hallmark
- Narrow QRS complexes (unless aberrant conduction or bundle branch block coexists)
- Ventricular rate varies (controlled <100 bpm; uncontrolled >100 bpm)
- Baseline appears undulating/chaotic
AF with rapid ventricular response (~126 bpm): Complete absence of organized P waves, fine fibrillatory baseline, and classic irregularly irregular R-R intervals.
3. Complete (Third-Degree) AV Block
Pathophysiology: No conduction occurs between atria and ventricles. Atria and ventricles beat independently; the ventricles are driven by a slow escape rhythm.
Key ECG Changes:
- AV dissociation — P waves and QRS complexes bear no relationship to each other
- Regular P-P intervals (atrial rate normal, 60–100 bpm)
- Regular R-R intervals but at a much slower ventricular escape rate (20–40 bpm if ventricular; 40–60 bpm if junctional)
- Wide QRS if escape is ventricular in origin (infra-nodal block); narrow if junctional
- Prolonged QTc common

Third-degree AV block: P waves (black arrows) march through at a regular atrial rate completely independent of the slow, widened ventricular escape complexes (~33 bpm). QTc 560 ms.
4. Ventricular Tachycardia (VT)
Pathophysiology: Three or more consecutive ventricular ectopic beats at rate >100 bpm, originating below the Bundle of His. Associated with ischaemic or structural heart disease.
Key ECG Changes:
- Wide QRS complexes (>120 ms), typically bizarre morphology
- Regular rapid rate (100–250 bpm) for monomorphic VT
- AV dissociation — independent P waves visible "marching through" QRS
- Fusion beats and capture beats (pathognomonic of VT)
- Concordance in precordial leads (all positive or all negative)
- Axis often markedly deviated (superior axis in fascicular VT)

Monomorphic VT: Wide-complex tachycardia with positive concordance across precordial leads V1–V6, superior axis (negative in II, III, aVF), and no visible P waves — consistent with structural heart disease.
5. Long QT Syndrome / Torsades de Pointes
Pathophysiology: Prolonged ventricular repolarization predisposes to early after-depolarizations, triggering polymorphic VT (Torsades de Pointes) that can degenerate into VF. Can be congenital (ion channel mutations) or acquired (drugs, electrolyte disturbances).
Key ECG Changes:
- Prolonged QTc >450 ms (male) / >470 ms (female) at baseline; >500 ms is high risk
- Prominent U waves (sometimes merged with T wave)
- Torsades de Pointes: polymorphic VT with QRS complexes that "twist" around the isoelectric line, waxing and waning in amplitude
- Initiated by a short-long-short R-R sequence ("pause-dependent")
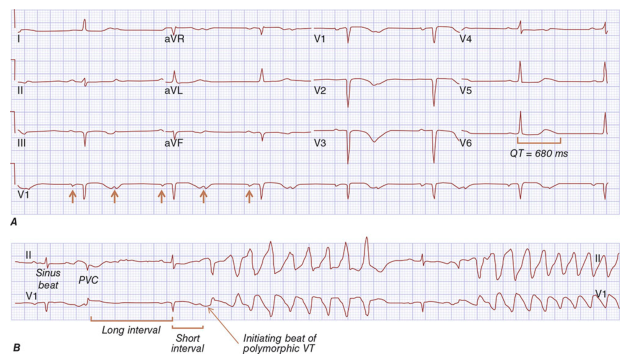
Harrison's: Panel A — baseline ECG with QT prolongation (680 ms) and prominent U waves. Panel B — initiation of Torsades de Pointes by a PVC on the long QT baseline.
6. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium causes diffuse subepicardial irritation, producing characteristic widespread repolarization changes across multiple vascular territories (unlike STEMI, which is territorial).
Key ECG Changes (4 stages):
- Stage 1 (acute): Diffuse concave ("saddle-shaped") ST elevation in most leads (I, II, III, aVF, V2–V6); PR-segment depression (most specific sign) in the same leads; PR elevation and ST depression in aVR
- Stage 2: ST normalises; PR depression may persist
- Stage 3: T-wave inversions develop
- Stage 4: ECG normalises
- Spodick's sign: downward slope of the TP segment
- No reciprocal changes (unlike STEMI)

Acute pericarditis: Diffuse concave ST elevation in I, II, III, aVF, V2–V6; PR depression in lead II (most specific); reciprocal ST depression and PR elevation in aVR. Sinus tachycardia from systemic inflammation.
7. Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Asymmetric myocardial hypertrophy (classically the interventricular septum) causes dynamic outflow obstruction, diastolic dysfunction, and ventricular arrhythmias. A leading cause of sudden cardiac death in young athletes.
Key ECG Changes:
- Left ventricular hypertrophy (LVH) voltage criteria (Sokolow: S in V1 + R in V5/V6 >35 mm)
- Deep, "giant" T-wave inversions in precordial leads (V2–V5) — especially in apical HCM (Yamaguchi syndrome)
- ST-segment depression (strain pattern) in lateral leads
- Absent septal Q waves in I, aVL, V5, V6 (due to septal hypertrophy)
- Left axis deviation common
- May show Wolff-Parkinson-White pattern (especially in PRKAG2 mutations)
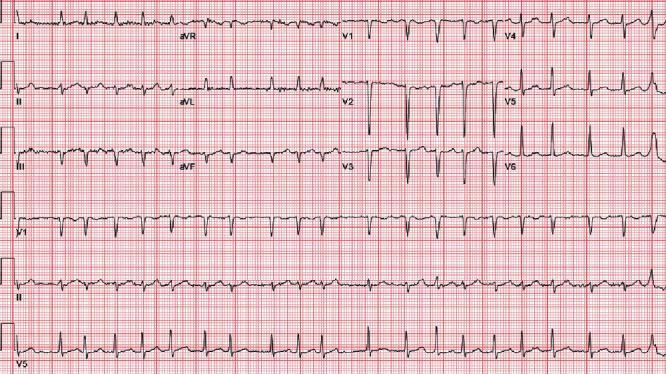
Septal HCM: High-amplitude R waves in V2–V4 (LVH), deep symmetric T-wave inversions and ST depression in precordial and lateral leads (strain pattern). Absent septal Q waves. Positive T in aVR (arrhythmic risk marker).
8. Pulmonary Embolism (PE)
Pathophysiology: Acute right ventricular pressure overload from pulmonary vascular obstruction produces characteristic right heart strain on ECG. The most common ECG finding is simply sinus tachycardia.
Key ECG Changes:
- Sinus tachycardia — most common finding (>40% of cases)
- S1Q3T3 pattern (McGinn-White sign): deep S wave in lead I + Q wave in lead III + T-wave inversion in lead III
- Right bundle branch block (complete or incomplete) — acute RV strain
- Right axis deviation
- T-wave inversions in V1–V4 — right ventricular strain
- P pulmonale (tall, peaked P in lead II >2.5 mm) — right atrial overload
- Atrial fibrillation/flutter may occur

Acute PE: Sinus tachycardia at ~116 bpm. Classic S1Q3T3 (prominent S in I, Q and T-inversion in III). Incomplete RBBB (QRS 110 ms). T-wave inversions in V1–V3 confirming right ventricular strain.
9. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, causing pre-excitation of the ventricles. The slow accessory conduction creates a delta wave, and the pathway can sustain circus-movement re-entrant tachycardias (SVT, and dangerously, AF with rapid conduction).
Key ECG Changes (Classic Triad):
- Short PR interval (<120 ms) — pre-excitation via accessory pathway
- Delta wave — slurred upstroke at the onset of QRS, representing early ventricular activation
- Wide QRS (>120 ms) — fusion of normal and accessory conduction
- Secondary ST-T changes discordant to QRS direction
- Pseudo-infarction Q waves in inferior leads (Type B WPW)
- Pathway location can be inferred from delta wave polarity

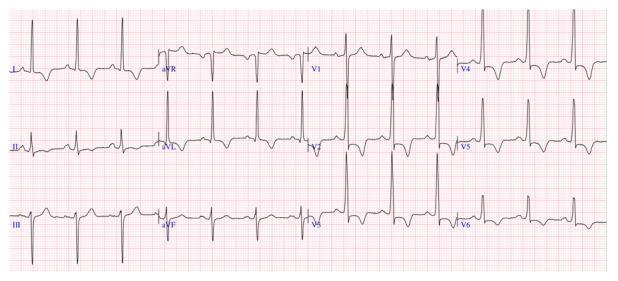
WPW: Short PR interval (<120 ms), prominent delta waves (slurred initial QRS upstroke) in II, III, aVF and V2–V6, and widened QRS complexes — the classic pre-excitation triad.
10. Dilated Cardiomyopathy (DCM)
Pathophysiology: Progressive dilatation and systolic dysfunction of the left (or both) ventricle(s) due to ischaemic, idiopathic, genetic, viral, or toxic causes. The stretched, fibrotic myocardium causes conduction delays and arrhythmias.
Key ECG Changes:
- Left bundle branch block (LBBB) — the most characteristic finding; wide QRS >120 ms, broad R waves in I, aVL, V5–V6; deep S/QS in V1–V3; discordant ST-T changes
- Left ventricular hypertrophy (voltage criteria)
- Poor R-wave progression across precordial leads
- First-degree AV block (prolonged PR)
- Left atrial enlargement (broad notched P wave — P mitrale)
- Frequent PVCs or non-sustained VT (marker of fibrosis)
- Atrial fibrillation common in advanced disease

DCM with LBBB: Wide QRS (>120 ms) with monophasic broad R waves in lateral leads (I, aVL, V5–V6) and deep QS complexes in V1–V3. Secondary ST-T changes (discordant ST depression/T inversion in lateral leads).
Quick Reference Summary Table
| # | Disease | Key ECG Hallmarks |
|---|---|---|
| 1 | STEMI | Convex ST elevation (territorial), reciprocal depression, Q waves |
| 2 | Atrial Fibrillation | Irregularly irregular, absent P waves, fibrillatory baseline |
| 3 | Complete AV Block | AV dissociation, slow escape rhythm, P marches through QRS |
| 4 | Ventricular Tachycardia | Wide QRS tachycardia, AV dissociation, fusion/capture beats |
| 5 | Long QT / TdP | QTc >500 ms, U waves, twisting polymorphic VT |
| 6 | Acute Pericarditis | Diffuse concave ST elevation, PR depression, Spodick's sign |
| 7 | Hypertrophic Cardiomyopathy | LVH, giant T-wave inversions, absent septal Q waves |
| 8 | Pulmonary Embolism | Sinus tachycardia, S1Q3T3, RBBB, T inversions V1–V4 |
| 9 | WPW Syndrome | Short PR, delta wave, wide QRS (pre-excitation triad) |
| 10 | Dilated Cardiomyopathy | LBBB, poor R progression, PVCs, first-degree AV block |
Clinical note: ECG changes must always be interpreted alongside clinical context. Many findings (e.g., ST elevation, T-wave inversions) overlap across conditions. Serial ECGs and correlation with biomarkers and imaging are essential for accurate diagnosis.
This is a shared conversation. Sign in to Orris to start your own chat.