A 23year old female patient is having excess white discharge from 4-5days
vaginal discharge vaginitis diagnosis management
Excess White Vaginal Discharge - 23-Year-Old Female
Overview
Differential Diagnosis
1. Bacterial Vaginosis (Most Common)
- Caused by overgrowth of anaerobic bacteria (most commonly Gardnerella vaginalis) replacing normal Lactobacillus flora
- Discharge: White or gray, thin, homogeneous, malodorous ("fishy" smell)
- Notably absent: Significant itch or pain
- pH > 4.5
2. Vulvovaginal Candidiasis (VVC)
- Caused by Candida albicans (>90% of cases)
- Discharge: White, thick, "cottage cheese"-like, odourless
- Key features: Intense vulval itching, burning, dyspareunia, vulvar erythema
- Triggered by antibiotics, high-oestrogen states (pregnancy, OCP), diabetes, immunosuppression
3. Trichomoniasis
- Caused by Trichomonas vaginalis (flagellated protozoan) - sexually transmitted
- Discharge: Frothy, yellow-green, malodorous
- Dysuria, vulval irritation, "strawberry cervix" on exam
- pH > 4.5
4. Physiological Leucorrhoea
- Normal clear-to-white discharge, cyclically varies with menstrual cycle
- No odour, itch, or irritation; no treatment needed
5. Cervicitis (Chlamydia / Gonorrhoea)
- Often presents with mucopurulent discharge from the cervix
- May be asymptomatic; consider in sexually active women
Key History to Elicit
| Question | Significance |
|---|---|
| Colour of discharge (white, grey, green, yellow) | Differentiates causes |
| Odour (fishy vs. none) | BV vs. candidiasis |
| Itching / burning | Strongly suggests candidiasis |
| Sexual activity / new partner | Trichomoniasis, STIs |
| Recent antibiotic use | Precipitates candidiasis |
| Dysuria / dyspareunia | Severity assessment |
| Last menstrual period | Physiological vs. pathological |
| Fever / lower abdominal pain | Suggests PID |
| Diabetes / immunosuppression | Risk factor for candidiasis |
Diagnosis
| Test | Finding | Diagnosis |
|---|---|---|
| Vaginal pH | > 4.5 | BV or Trichomoniasis |
| Saline wet mount | Clue cells (>20%) | BV (Sens 74%, Spec 86%) |
| Saline wet mount | Motile trichomonads | Trichomoniasis (Spec 100%) |
| KOH (10%) wet mount | Hyphae / pseudohyphae | Candidiasis |
| Whiff test (KOH + discharge) | Fishy amine odour | BV (Sens 67%, Spec 93%) |
| NAAT (vaginal/urine) | T. vaginalis | Trichomoniasis (Sens 95-100%) |
| Gram stain | Reduced Lactobacilli, Gardnerella | BV |
- Thin, homogeneous white/grey discharge
- Vaginal pH > 4.5
- Positive whiff test
-
20% clue cells on wet mount
Treatment
| Condition | First-line Treatment |
|---|---|
| Bacterial Vaginosis | Oral metronidazole 500 mg BD x 7 days, OR intravaginal metronidazole gel, OR intravaginal clindamycin cream |
| Vulvovaginal Candidiasis | Short course topical antifungal (clotrimazole, miconazole), OR single dose oral fluconazole 150 mg |
| Trichomoniasis | Metronidazole 2g single dose OR tinidazole 2g single dose; treat partner simultaneously |
| Physiological | Reassurance; no treatment needed |
Note: For trichomoniasis, partner treatment is mandatory and sexual intercourse should be avoided until both partners complete treatment and symptoms resolve.
Red Flags - Refer/Investigate Further If:
- Fever or lower abdominal/pelvic pain (suggests pelvic inflammatory disease - PID)
- Postcoital or intermenstrual bleeding (cervical pathology)
- Offensive discharge with systemic symptoms (sepsis)
- Recurrent episodes (rule out diabetes, HIV, immunosuppression)
- No improvement after empirical treatment
She had sex and after it she took northeisterone tablet and the next day period came
norethisterone vaginal discharge hormonal effects
norethisterone tablet after sex period next day white discharge mechanism
Updated Clinical Analysis - Full Picture
Understanding the Timeline
Unprotected sex → Norethisterone tablet taken → Period came next day → White discharge (4-5 days)
What is Norethisterone Here?
- Delay a period (taken before expected period), or
- Misused as emergency contraception - which is a common misconception in India and South Asia
Critical note: Norethisterone is NOT an emergency contraceptive. It does not prevent pregnancy. Many patients take it after unprotected sex believing it works like a "morning-after pill," but this is incorrect.
Why Did the Period Come the Next Day?
- The patient was already in the late luteal phase (near her period date)
- Norethisterone temporarily maintains the endometrium
- When its effect is transient or insufficient, withdrawal bleeding occurs
- This bleed can appear quickly, especially if the natural period was already imminent
Why is There White Discharge After the Period?
Most Likely: Hormonal / Physiological
| Cause | Explanation |
|---|---|
| Post-menstrual physiological discharge | Normal clear-to-white discharge resumes after a period as oestrogen rises in the follicular phase |
| Norethisterone-induced cervical mucus changes | Progestogens alter cervical mucus - becoming thicker and more prominent; this can persist after stopping the tablet |
| Hormonal disruption | A single dose of norethisterone disrupts the normal cycle pattern, potentially altering discharge character for 1-2 weeks |
Must Not Miss: Infection After Unprotected Sex
| Infection | Discharge Character | Other Features |
|---|---|---|
| Bacterial Vaginosis | White/grey, thin, fishy odour | No/minimal itch |
| Vulvovaginal Candidiasis | White, thick, curdy | Itching, burning |
| Chlamydia / Gonorrhoea (cervicitis) | White/yellow, mucopurulent | Often asymptomatic |
| Trichomoniasis | Frothy, yellow-green | Odour, irritation |
Is She Protected from Pregnancy?
- Norethisterone does not prevent pregnancy
- The "period" she had is likely a withdrawal bleed - it does not confirm she is not pregnant
- If fertilisation occurred before the tablet was taken, a pregnancy could still be ongoing
- A urine pregnancy test (ideally 2-3 weeks after unprotected sex for reliable results) should be done if there is concern
What Should Be Done Now?
Immediate Assessment
- Full history - nature of discharge (colour, smell, itch), any abdominal pain, dyspareunia
- Menstrual history - was the period normal in flow and duration, or lighter/unusual?
- Per speculum exam - assess cervix, nature of discharge, vaginal walls
- Vaginal pH - quick bedside test
Investigations
- Wet mount microscopy (clue cells, hyphae, trichomonads)
- Vaginal swab for culture
- Endocervical swab for Chlamydia/Gonorrhoea NAAT (given unprotected sex)
- Urine pregnancy test if there is any doubt about the nature of the bleed
Counselling Points
- Norethisterone is not an emergency contraceptive - educate the patient
- If emergency contraception was needed, levonorgestrel 1.5 mg (within 72 hrs) or ulipristal acetate (within 120 hrs) or a copper IUD (within 120 hrs) are the correct options
- Advise on barrier contraception and STI prevention
Treatment
- If infective cause found - treat specifically (metronidazole for BV/TV, fluconazole for candidiasis, doxycycline/azithromycin for chlamydia)
- If physiological/hormonal - reassurance; discharge should resolve as the cycle normalises
- Avoid douching, fragranced products
No itching no burning
Updated Differential - No Itch, No Burning
Most Likely Causes (in order of probability)
| Cause | Why it fits | Key feature |
|---|---|---|
| Physiological / hormonal discharge | Post-period + norethisterone-induced cervical mucus change | White, odourless, no symptoms |
| Bacterial Vaginosis | Most common pathological white discharge without itch | May have mild fishy odour |
| Chlamydial cervicitis | Often completely asymptomatic - "silent STI" | Mucopurulent discharge from os, no itch |
Effectively Ruled Out
- Vulvovaginal Candidiasis - almost always causes significant itching; absence strongly argues against it
- Trichomoniasis - usually causes irritation, burning, offensive odour
The Most Important Question Now
- No odour → Points strongly to physiological/hormonal (norethisterone effect + post-menstrual mucus)
- Fishy/musty odour → Points to Bacterial Vaginosis
- No odour but yellowish tinge → Consider chlamydial cervicitis (swab needed)
Most Probable Diagnosis in This Case
- 23-year-old female
- Unprotected sex → norethisterone → withdrawal bleed
- White discharge starting after the bleed
- No itch, no burning, no odour mentioned
Management
If No Odour and No Other Symptoms
- Reassurance - most likely physiological/hormonal
- Discharge should resolve within 1-2 weeks as the hormonal disruption settles
- No antibiotic treatment needed
- Advise to return if odour develops, discharge becomes yellow/green, or lower abdominal pain appears
Still Recommended Regardless
- Urine pregnancy test - norethisterone is NOT a contraceptive; the bleed was likely withdrawal, not a true period confirming no pregnancy
- Endocervical swab for Chlamydia NAAT - given unprotected sex; chlamydia is asymptomatic in ~70% of women and this should not be missed
- Counsel on correct emergency contraception options for future use
Generate a STI screening checklist for this patient 3-4days
ls -la /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace && ls -la /home/daytona/workspace/
Her cycle was about to come in 3-4 days from the day she took pill
Revised Understanding - Cycle Was Due in 3-4 Days
What Actually Happened
Day 0: Unprotected sex → Norethisterone tablet taken (cycle due in 3-4 days)
Day 1: Period came
Day 2-6: White discharge (4-5 days, no itch, no burn)
- Ovulation had already occurred ~10-14 days earlier
- The endometrium was already preparing to shed
- The norethisterone had minimal effect - the bleed came anyway the next day because the endometrium was already primed to shed
- This bleed was most likely her actual natural period, not purely a withdrawal bleed
Key Implication for Pregnancy Risk
| Timing | Significance |
|---|---|
| Sex occurred in late luteal phase (3-4 days before period) | Very low fertility window - ovulation was ~10-14 days prior |
| Norethisterone taken at this stage | Does NOT act as contraception regardless |
| Period came next day as expected | Strongly suggests normal cycle, ovulation had already passed |
What the White Discharge Now Represents
1. Early Follicular Phase Physiological Discharge (Most Likely)
- After the period ends, rising oestrogen stimulates cervical glands
- Produces white to clear, non-offensive discharge
- This is completely normal in days 1-5 after a period
- No odour, no itch - exactly matching this patient
2. Norethisterone Cervical Mucus Effect (Contributing)
- Even a single dose alters cervical mucus temporarily
- Can make discharge more visible/prominent for a few days
- Self-resolving as the drug clears (half-life ~8 hours)
3. Still Cannot Ignore - Unprotected Sex
- Chlamydia/gonorrhoea remain asymptomatic in most women
- Must be screened regardless of how benign the discharge appears
Revised Probability Ranking
| Diagnosis | Probability | Reasoning |
|---|---|---|
| Physiological post-menstrual discharge | Very high | Timing fits perfectly, no symptoms |
| Norethisterone cervical mucus effect | High | Known side effect, temporal relation |
| Bacterial Vaginosis | Low-moderate | No odour mentioned, but possible |
| Chlamydial cervicitis | Low but must screen | Asymptomatic in 70% of women |
| Candidiasis | Very unlikely | No itch, no burning |
| Pregnancy | Very low | Sex in late luteal phase, period came |
Final Management Plan
Do Now
- Reassure - timing strongly suggests physiological discharge
- Urine pregnancy test - belt-and-suspenders confirmation
- Chlamydia + Gonorrhoea NAAT swab - unprotected sex, cannot be skipped
Counselling
- Her period came because it was already due - norethisterone had minimal effect here
- Norethisterone is not a contraceptive - educate clearly
- For future unprotected sex: Levonorgestrel 1.5mg within 72 hours is the correct emergency contraceptive
- Advise barrier contraception (condoms) going forward
Expectation
- Discharge should resolve on its own within 3-5 days as oestrogen rises and cervical mucus transitions to the fertile-type clear mucus mid-cycle
- No antibiotics needed unless swab returns positive
A 23year old female wants a laser for rapid growth of ingrown hairs over chin
laser hair removal hirsutism PCOS
PMID: 38630483
23-Year-Old Female - Ingrown Hairs on Chin + Laser Request
Step 1: Recognise the Red Flag First
Do not proceed to laser without investigating the cause. Laser on an active hormonal drive will give poor, temporary results and the underlying condition will be missed.
The Underlying Cause Must Be Identified
Most Likely: PCOS (Polycystic Ovary Syndrome)
- Most common cause of hyperandrogenism and hirsutism in women of reproductive age
- Rotterdam criteria: 2 of 3 - (1) clinical/biochemical hyperandrogenism, (2) ovulatory dysfunction, (3) polycystic ovarian morphology on ultrasound
- Often accompanied by insulin resistance, irregular cycles, acne
Other Causes to Exclude
| Cause | Key Features |
|---|---|
| Non-classic Congenital Adrenal Hyperplasia (NCAH) | Mimics PCOS; elevated 17-OHP |
| Cushing Syndrome | Central obesity, striae, HTN, moon face |
| Androgen-secreting ovarian/adrenal tumour | Rapid onset, virilization - this case has "rapid growth" - must exclude |
| Hyperprolactinaemia | Galactorrhoea, amenorrhoea, anovulation |
| Idiopathic hirsutism | Normal androgens, regular cycles - diagnosis of exclusion |
"Rapid and rapidly progressing signs of androgen excess require careful investigation for an androgen-secreting neoplasm" - Berek & Novak's Gynecology, p. 1906
Investigations Before Any Laser
Hormonal Panel (Morning, Days 4-10 of cycle)
| Test | Purpose | Normal Range |
|---|---|---|
| Total Testosterone | Androgen excess | 20-80 ng/dL |
| Free Testosterone (calculated) | Bioactive fraction | 0.6-6.8 pg/mL |
| DHEAS | Adrenal androgen source | 100-350 µg/dL |
| Androstenedione | Androgen precursor | 20-250 ng/dL |
| SHBG | Low in PCOS/insulin resistance | 18-114 nmol/L |
| 17-OHP (follicular phase) | Exclude NCAH | <300 ng/dL = likely unaffected |
| Prolactin | Exclude hyperprolactinaemia | - |
| TSH | Thyroid dysfunction | - |
| Fasting insulin + glucose | Insulin resistance in PCOS | - |
Imaging
- Pelvic ultrasound - ovarian morphology (polycystic ovaries)
- If testosterone markedly elevated (>150-200 ng/dL): adrenal/ovarian MRI to exclude tumour
Clinical Scoring
- Ferriman-Gallwey score - standardised hirsutism severity score (score >8 = hirsutism)
Laser Treatment - When Appropriate
Best Laser Options for Chin Hair
| Laser Type | Wavelength | Notes |
|---|---|---|
| Alexandrite laser | 755 nm | Best evidence for hirsutism in PCOS; effective at high fluence |
| Diode laser | 810 nm | Effective; safer for darker skin types (Fitzpatrick IV-VI) |
| Nd:YAG | 1064 nm | Best for dark skin (Fitzpatrick V-VI); less risk of dyspigmentation |
| IPL (Intense Pulsed Light) | Broadband | Less effective than alexandrite/diode laser |
Evidence (JAMA Dermatology 2024 - Systematic Review, PMID 38630483)
- Alexandrite laser showed significant improvement in hirsutism severity and psychological outcomes, especially at high fluence
- Alexandrite > IPL for effectiveness
- Diode laser + metformin (if PCOS) superior to diode laser alone
- Diode laser + combined OCP superior to diode laser alone
- Conclusion: laser works best combined with systemic hormonal treatment
Practical Points for Laser in This Patient
- Number of sessions: 6-8 sessions typically needed, 4-6 weeks apart (hair must be in anagen phase)
- Fitzpatrick skin type must be assessed - Indian/South Asian skin (Type IV-V) requires Nd:YAG or long-pulsed diode to avoid post-inflammatory hyperpigmentation
- Ingrown hairs will also improve with laser as the follicle is permanently reduced
- Active hormonal drive = regrowth between/after sessions; must treat hormonally in parallel
- Avoid sun exposure 4-6 weeks pre/post treatment
Treatment Plan Summary
Step 1 → Hormonal workup + pelvic ultrasound
Step 2 → Diagnose cause (PCOS most likely)
Step 3 → Start systemic treatment:
- Combined OCP (reduces ovarian androgen production - reduces hair growth
in ~2/3 of hirsute patients)
- ± Metformin (if insulin resistance/PCOS)
- ± Spironolactone/cyproterone acetate (anti-androgen)
Step 4 → Laser hair reduction (alexandrite or diode) as adjunct
- Works significantly better WITH hormonal treatment than alone
Step 5 → Reassess Ferriman-Gallwey score at 6 months
Create a hormonal treatment algorithm for PCOS-related hirsutism
PCOS hirsutism treatment guidelines antiandrogen
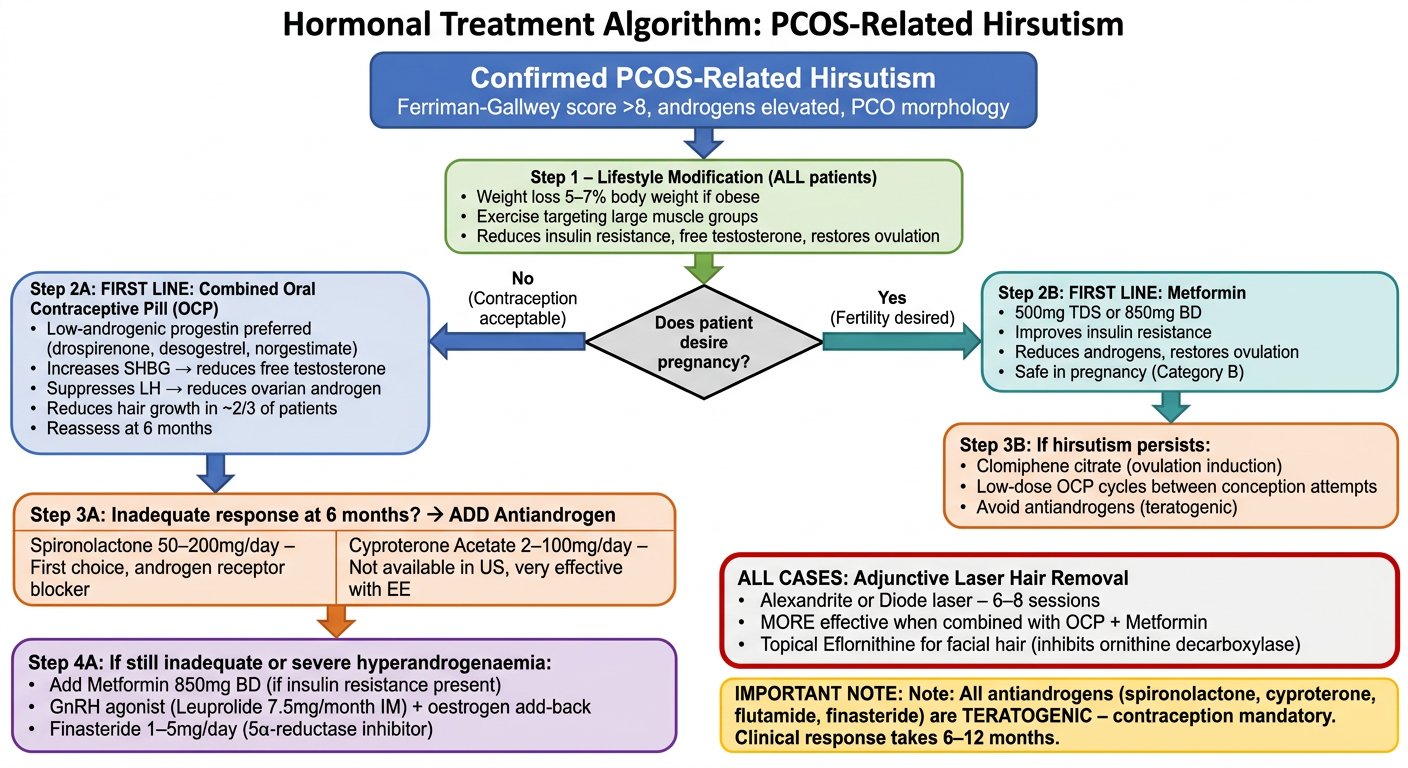
A clean, professional medical clinical algorithm flowchart titled "Hormonal Treatment Algorithm: PCOS-Related Hirsutism" with a white background and clear box-and-arrow flowchart design. The algorithm flows top to bottom with these steps: TOP BOX (blue header): "Confirmed PCOS-Related Hirsutism" with subtitle "Ferriman-Gallwey score >8, androgens elevated, PCO morphology" STEP 1 BOX (green): "Step 1 – Lifestyle Modification (ALL patients)" with bullet points: "• Weight loss 5–7% body weight if obese", "• Exercise targeting large muscle groups", "• Reduces insulin resistance, free testosterone, restores ovulation" DECISION DIAMOND: "Does patient desire pregnancy?" LEFT BRANCH – "No (Contraception acceptable)": STEP 2A BOX (blue): "FIRST LINE: Combined Oral Contraceptive Pill (OCP)" with details: "• Low-androgenic progestin preferred (drospirenone, desogestrel, norgestimate)", "• Increases SHBG → reduces free testosterone", "• Suppresses LH → reduces ovarian androgen", "• Reduces hair growth in ~2/3 of patients", "• Reassess at 6 months" STEP 3A BOX (orange): "Inadequate response at 6 months? → ADD Antiandrogen" with two columns: "Spironolactone 50–200mg/day – First choice, androgen receptor blocker" and "Cyproterone Acetate 2–100mg/day – Not available in US, very effective with EE" STEP 4A BOX (purple): "If still inadequate or severe hyperandrogenaemia:" with bullets: "• Add Metformin 850mg BD (if insulin resistance present)", "• GnRH agonist (Leuprolide 7.5mg/month IM) + oestrogen add-back", "• Finasteride 1–5mg/day (5α-reductase inhibitor)" RIGHT BRANCH – "Yes (Fertility desired)": STEP 2B BOX (teal): "FIRST LINE: Metformin" with details: "• 500mg TDS or 850mg BD", "• Improves insulin resistance", "• Reduces androgens, restores ovulation", "• Safe in pregnancy (Category B)" STEP 3B BOX (orange): "If hirsutism persists:" with bullets: "• Clomiphene citrate (ovulation induction)", "• Low-dose OCP cycles between conception attempts", "• Avoid antiandrogens (teratogenic)" BOTTOM BOX (red border): "ALL CASES: Adjunctive Laser Hair Removal" with bullets: "• Alexandrite or Diode laser – 6–8 sessions", "• MORE effective when combined with OCP + Metformin", "• Topical Eflornithine for facial hair (inhibits ornithine decarboxylase)" IMPORTANT NOTE BOX (yellow): "Note: All antiandrogens (spironolactone, cyproterone, flutamide, finasteride) are TERATOGENIC – contraception mandatory. Clinical response takes 6–12 months." Use professional medical diagram styling with color-coded boxes, clear directional arrows, clean sans-serif font, and appropriate spacing.
Algorithm Explained - Drug Details
Step 1 - Lifestyle (Everyone)
Branch A - Contraception Acceptable (Not Seeking Pregnancy)
| Line | Drug | Dose | Mechanism | Key Point |
|---|---|---|---|---|
| 1st | Combined OCP | 1 tablet daily | Raises SHBG, suppresses LH, inhibits 5α-reductase | Prefer low-androgenic progestin: drospirenone, desogestrel, norgestimate. Avoid norgestrel/norethindrone (androgenic) |
| 2nd (add-on) | Spironolactone | 50-200mg/day | Competitive AR blocker + inhibits 5α-reductase | Most studied antiandrogen; monitor K⁺; use with OCP |
| 2nd (alternative) | Cyproterone acetate | 2mg (in OCP) or 12.5-100mg | Competes with DHT at AR | More effective than OCP alone; not available in USA |
| 3rd | Finasteride | 1-5mg/day | 5α-reductase type 2 inhibitor | Reduces DHT at follicle; Pregnancy Category X |
| Severe/refractory | GnRH agonist (Leuprolide) | 7.5mg/month IM | Suppresses gonadotropins → ovarian androgen | Must add oestrogen add-back to prevent osteoporosis |
| If insulin resistance | Metformin | 850mg BD or 500mg TDS | Reduces hyperinsulinaemia → reduces ovarian androgens | Add to OCP for superior results |
Branch B - Fertility Desired
| Line | Drug | Dose | Rationale |
|---|---|---|---|
| 1st | Metformin | 500mg TDS or 850mg BD | Safe in pregnancy, reduces androgens, restores ovulation |
| 2nd | Clomiphene citrate | 50-150mg Day 2-6 | Ovulation induction |
| Avoid | All antiandrogens | - | Teratogenic - absolutely contraindicated |
Adjunctive - All Cases
- Topical Eflornithine (Vaniqa): Only FDA-approved topical for facial hair; inhibits ornithine decarboxylase shortening anagen phase; used with laser for superior results
- Laser hair removal: Alexandrite or diode laser; 6-8 sessions; significantly more effective when combined with OCP + Metformin than laser alone (JAMA Dermatology 2024)
Critical Safety Reminders
All antiandrogens are TERATOGENIC. Spironolactone (Category C), cyproterone, flutamide, finasteride (Category X) - reliable contraception is mandatory throughout treatment.
Response is slow - patients must be counselled that clinical improvement in hair growth takes 6-12 months. Existing terminal hairs do not regress; only new growth is suppressed.
A 23y f pt came to the opd with Hyperpigmented lips but she doesnt smoke
Hyperpigmented Lips - 23-Year-Old Female (Non-Smoker)
Why Non-Smoking Matters
Differential Diagnosis - Structured Approach
🔴 Must Not Miss (Systemic/Serious)
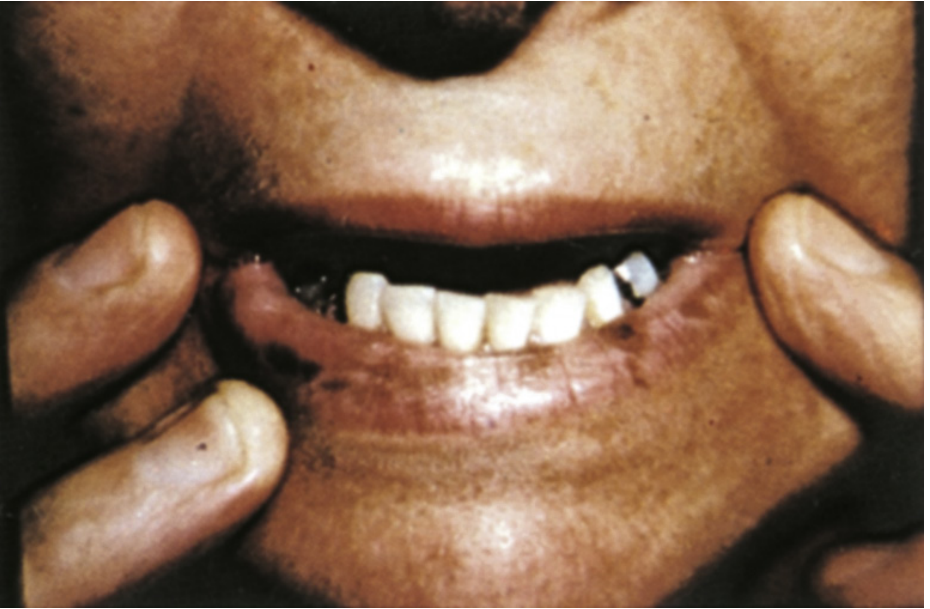
1. Peutz-Jeghers Syndrome (PJS)
- Autosomal dominant - mutation in STK11/LKB1 tumour suppressor gene
- Classic triad: Hyperpigmented macules on lips + GI hamartomatous polyposis + markedly elevated cancer risk
- Macule characteristics: Dark brown/black, appear on lower lip predominantly, perioral skin, buccal mucosa, tongue, fingers, toes
- Appear in infancy/early childhood, grow until puberty, then skin lesions regress - but buccal macules persist
-
95% of patients have perioral lesions
⚠️ If this diagnosis is suspected, refer for GI endoscopy, colonoscopy, capsule endoscopy, and genetic testing immediately.
2. Addison's Disease (Primary Adrenal Insufficiency)
- ACTH excess → stimulates MC1R → diffuse melanin hyperpigmentation
- Distribution: skin, oral mucosa, lips, buccal mucosa, palmar creases, scars, areolae, genitalia
- Associated symptoms: fatigue, weight loss, postural hypotension, salt craving, nausea
- Investigations: 8 AM cortisol, ACTH stimulation test, ACTH level, electrolytes (hyponatraemia, hyperkalaemia)
🟡 Hormonal / Metabolic
3. PCOS with Acanthosis Nigricans / Hyperandrogenism
- PCOS with insulin resistance can cause generalised hyperpigmentation of skin, areolae, genitalia, buccal mucosa, and palmar creases
- Acanthosis nigricans (velvety dark patches at neck, axilla) is common in PCOS and reflects insulin resistance
- Combined with the previous case context for this patient - highly relevant
4. Melasma / Chloasma
- Hormonally-driven melanin overproduction - classically triggered by oestrogen (OCPs, pregnancy)
- Usually affects cheeks, forehead, upper lip area (perioral)
- Check if patient is on oral contraceptives
5. Pregnancy
- Increased melanogenesis due to elevated oestrogen and progesterone
- Causes perioral and facial hyperpigmentation, linea nigra, areolar darkening
🟢 Benign / Acquired
6. Laugier-Hunziker Syndrome
- Acquired (not inherited, no systemic disease) - important distinction from PJS
- Presents with mucosal pigmentation (lips, buccal mucosa) + longitudinal pigmented nail streaks (melanonychia)
- Benign - no GI polyps, no cancer risk
- Diagnosis of exclusion after PJS ruled out
7. Post-Inflammatory Hyperpigmentation (PIH)
- History of lip trauma, herpes labialis, allergic contact dermatitis, lip licking
- Usually patchy, asymmetric, correlated with history
8. Contact/Allergic Reaction
- Lipsticks (especially dark), lip balms, toothpaste (cinnamon/fluoride), food dyes
- Ask about cosmetic use history
9. Drug-Induced Hyperpigmentation
| Drug | Pattern |
|---|---|
| Antimalarials (chloroquine, hydroxychloroquine) | Diffuse skin + mucosal |
| Minocycline | Grey-blue skin, mucosa, nails |
| Cyclophosphamide | Diffuse skin + mucous membranes |
| Zidovudine (ART) | Mucosal + nail pigmentation |
| Amiodarone | Slate-grey photodistributed |
10. Nutritional Deficiency
- Vitamin B12 deficiency - causes mucocutaneous hyperpigmentation; especially in vegetarians/vegans
- Folic acid deficiency - similar pattern
- Check CBC, B12, folate levels
Key History to Elicit
| Question | Targets |
|---|---|
| Family history of lip spots or GI polyps? | Peutz-Jeghers (autosomal dominant) |
| Episodes of abdominal pain, vomiting, rectal bleeding? | PJS polyps, intussusception |
| Fatigue, weight loss, postural dizziness, salt craving? | Addison's disease |
| Irregular periods, excess hair growth, acne? | PCOS (given previous context - very relevant) |
| Currently on OCP or hormonal therapy? | Melasma/chloasma |
| Vegetarian/vegan diet? | B12 deficiency |
| Cosmetic use - lipstick, balm, toothpaste? | Contact pigmentation |
| Any medications? | Drug-induced |
| When did it start? Childhood vs recent? | PJS (childhood) vs acquired |
| Is it macules (spots) or diffuse darkening? | PJS/Laugier = macules; Addison/PCOS = diffuse |
| Nail changes? | Laugier-Hunziker (melanonychia) |
Investigations - Prioritised
First Line (All Patients)
| Test | Targets |
|---|---|
| 8 AM serum cortisol + ACTH | Addison's disease |
| CBC + peripheral smear | B12 deficiency (macrocytic anaemia) |
| Serum Vitamin B12 + Folate | Nutritional deficiency |
| Fasting glucose + insulin + HOMA-IR | PCOS/insulin resistance |
| Thyroid function (TSH) | Associated autoimmune disease |
| LH, FSH, testosterone, DHEAS | PCOS/hyperandrogenism |
Second Line (If PJS Suspected)
| Test | Purpose |
|---|---|
| STK11 gene mutation testing | Confirm PJS diagnosis |
| Upper GI endoscopy + colonoscopy | Detect GI polyps |
| Capsule endoscopy (small bowel) | Small bowel polyps (most common site) |
| Pelvic ultrasound | Ovarian sex cord tumours in female PJS |
| Dermatoscopy of lesions | Characterise macule pattern |
Summary - Most Likely in This 23-Year-Old
| Priority | Diagnosis | Why |
|---|---|---|
| Must exclude first | Peutz-Jeghers Syndrome | Young woman, lip macules, high cancer stakes |
| Must exclude | Addison's Disease | Life-threatening if missed, classic distribution |
| Very relevant here | PCOS + insulin resistance | Given her previous history in this consultation |
| Common/benign | Laugier-Hunziker / contact / B12 deficiency | After serious causes excluded |
What lipbalm to prescribe
Important Caveat First
Topical Agents for Lip Hyperpigmentation
1. Kojic Acid Lip Balm / Gel (Most Commonly Prescribed)
- Mechanism: Inhibits tyrosinase → reduces melanin synthesis
- Formulation: 1-4% kojic acid in lip-safe base
- Use: Apply twice daily; results in 4-8 weeks
- Safe for lips: Yes - widely available OTC and prescription
- Brands: Kojic acid lip serums (multiple brands)
2. Hydroquinone (2%) - Short Term Only
- Mechanism: Tyrosinase inhibitor - gold standard depigmenting agent
- Formulation: 2% cream/gel - apply thinly to lip vermilion only
- Caution on lips: Use carefully - avoid ingestion; do NOT use >12 weeks continuously (risk of ochronosis with prolonged use)
- Not first choice for lips due to mucosal location
3. Azelaic Acid 15-20%
- Mechanism: Inhibits tyrosinase + anti-inflammatory
- Advantage: Safe for long-term use, no risk of ochronosis
- Bonus: Also treats acne - relevant if this patient has PCOS-related acne
- Apply once daily to affected lip area
4. Niacinamide 4-5% Lip Balm
- Mechanism: Inhibits melanosome transfer from melanocytes to keratinocytes
- Safest option for lips - no toxicity concerns with mucosal contact
- Good for maintenance and mild cases
- Widely available OTC
5. SPF Lip Balm (Mandatory Add-On)
- UV exposure is a major driver of lip hyperpigmentation
- Prescribe SPF 30-50 lip balm alongside any depigmenting agent
- Without sun protection, no depigmenting agent will work effectively
- Reapply every 2 hours if outdoors
Recommended Prescription Combination
For mild-moderate lip hyperpigmentation (cause established as benign/cosmetic):
1. Kojic Acid 2% + Niacinamide 4% Lip Gel – apply BD (morning & night)
OR
Azelaic Acid 15% gel – apply OD at night
2. SPF 50 Lip Balm (e.g., La Roche-Posay Anthelios) – apply every morning,
reapply 2-hourly in sun
3. Review at 8 weeks
What to Avoid on Lips
| Avoid | Reason |
|---|---|
| High-concentration hydroquinone (>2%) | Mucosal absorption, ochronosis risk |
| Tretinoin (retinoic acid) on lips | Severe irritation, mucosal sensitivity |
| Mercury-containing products | Toxic |
| Prolonged steroid-containing creams | Skin atrophy, systemic absorption |
Additional Lifestyle Advice
- Stop licking lips - saliva enzymes worsen pigmentation and dryness
- Avoid dark/pigmented lipsticks and lip liners temporarily - can worsen pigmentation
- Stay hydrated - dry lips → micro-inflammation → PIH
- Check cosmetics for potential allergens - cinnamates, fragrances, dyes
How to use melitaine solution
melitane solution how to use cosmetic ingredient alpha-MSH tripeptide pigmentation
melitane topical solution instructions dermatology hyperpigmentation lips
melitane INCI ingredient cosmetic formulation usage percentage instructions seppic
https://www.ulprospector.com/en/na/PersonalCare/Detail/4501/…
Important Clarification First
Critical point: Melitane stimulates melanin synthesis - it is a pro-pigmentation agent, not a depigmenting one. It mimics alpha-MSH and activates MC1-R receptors to promote skin tanning and pigment formation. Prescribing this to a patient with hyperpigmented lips would worsen the condition.
What Melitane Actually Does
| Property | Detail |
|---|---|
| INCI Name | Acetyl Hexapeptide-1 |
| Manufacturer | Lucas Meyer Cosmetics (Clariant) |
| Mechanism | Biomimetic alpha-MSH analog → activates MC1-R → stimulates melanogenesis → increases melanin production |
| Primary use | Promotes skin tanning/pigmentation, UV-induced erythema protection, DNA repair after UV exposure |
| Anti-aging benefit | Reduces UV-induced sunburn cells, limits inflammatory mediators |
| Indicated for | Patients with hypopigmentation, vitiligo support, sunless tanning formulations, UV protection products |
| Contraindicated for | Patients with existing hyperpigmentation - it will make dark lips/spots darker |
Could There Be Confusion in Terminology?
| You might mean | What it is | Used for |
|---|---|---|
| Melitane (Acetyl Hexapeptide-1) | Pro-pigmentation peptide | Tanning, UV protection - NOT for dark lips |
| Mela-Cream / Melalite (Hydroquinone 2-4%) | Depigmenting agent | Dark spots, melasma, lip hyperpigmentation |
| Melaglow / MelaFade | Kojic acid + arbutin combinations | Skin lightening |
| Melarase | Kojic + niacinamide cream | Hyperpigmentation treatment |
| Melatonik | Tranexamic acid serum | Melasma |
If Your Patient Has Hyperpigmented Lips - Do NOT Use Melitane
| Agent | Action |
|---|---|
| Kojic acid 2% | Tyrosinase inhibitor - lightens |
| Niacinamide 4-5% | Inhibits melanosome transfer - lightens |
| Azelaic acid 15-20% | Tyrosinase inhibitor - lightens |
| Hydroquinone 2% (short term) | Gold standard depigmenter |
| SPF 50 lip balm | Mandatory - prevents UV-driven worsening |
Melitraine altris 5
Altris 5 tretinoin cream India how to use instructions
Melitraine cream tretinoin hyperpigmentation India dermatology
Altris 5 cream tretinoin 0.05% uses side effects how to apply India brand
Altris 5 (Tretinoin 0.05% Cream) - How to Use
What It Is
- Active ingredient: Tretinoin (all-trans retinoic acid) 0.05%
- Class: First-generation retinoid (Vitamin A derivative)
- Action for hyperpigmentation: Disperses and reduces melanin granules in keratinocytes, accelerates epidermal cell turnover, fades dark spots and mottled pigmentation
- Results timeline: 8-12 weeks for pigmentation; up to 6 months for full effect
Step-by-Step Application Guide
Evening Routine Only (Never Morning)
- Use a pea-sized amount - enough to cover the entire face lightly
- Dot on forehead, both cheeks, nose, chin
- Spread evenly with fingertips
- Keep away from: eyes, corners of nose, lips, mouth - these areas are very sensitive
- For lip hyperpigmentation specifically: apply to the skin around the lips (perioral area), not directly on the lip vermilion
Frequency Schedule - Build Up Slowly
| Week | Frequency | Why |
|---|---|---|
| Weeks 1-2 | Every 3rd night (2x/week) | Allow skin to adjust |
| Weeks 3-4 | Every other night (3-4x/week) | Gradual increase |
| Weeks 5-6 | Every other night | Continue building |
| Weeks 7+ | Every night | Full maintenance dose |
If irritation is significant at any stage, drop back to every other night and build up again more slowly.
Critical Instructions
☀️ Sun Protection is Mandatory
- Tretinoin makes skin significantly more photosensitive
- Apply SPF 30-50 broad spectrum sunscreen every morning without fail
- Without sunscreen, tretinoin will worsen pigmentation rather than improve it
- Avoid prolonged sun exposure; wear a hat/dupatta when outdoors
❌ Do NOT Use With
- Waxing or threading in the same area (skin is fragile - PIH risk)
- Benzoyl peroxide at the same time (inactivates tretinoin)
- Medicated/astringent toners, salicylic acid products simultaneously
- Other exfoliants (AHA/BHA) on the same nights
✅ Safe to Use Alongside
- Gentle moisturiser (recommended - reduces dryness)
- Niacinamide serum (mornings)
- SPF sunscreen (mornings - mandatory)
- Kojic acid / azelaic acid (alternating nights, not same night)
What to Expect - Normal Reactions
| Reaction | When | What to Do |
|---|---|---|
| Redness, mild stinging, dryness | First 2-4 weeks | Normal - continue, use more moisturiser |
| Peeling, flaking | Weeks 2-6 | Normal - do not scratch or pick; moisturise well |
| Temporary worsening of pigmentation | First few weeks | Normal (purge phase) - continue |
| Improved pigmentation | Weeks 8-12 | Expected result |
Important Caution for This Patient
Do NOT apply Altris 5 directly on the vermilion lip surface. The lip mucosa has no stratum corneum and tretinoin will cause severe irritation, burning, and peeling on actual lip tissue. Apply only to the perioral skin (skin around the lips) for perioral hyperpigmentation. For pigmentation on the lip itself, use kojic acid + niacinamide lip balm + SPF as discussed.
Pregnancy Warning
Melitaine altris 5 hair solution
Altris 5 hair solution tretinoin minoxidil scalp India how to use
"Melitane" OR "Melitaine" hair solution scalp India brand ingredients
https://pmc.ncbi.nlm.nih.gov/articles/PMC6892010
Melitane Altris 5 Solution Spray - Complete Guide
What It Actually Is
| Property | Detail |
|---|---|
| Active ingredient | Melitane (Acetyl Hexapeptide-1) 5% |
| Manufacturer | Alembic Pharmaceuticals, India |
| Formulation | Aqueous solution / spray, 60 ml |
| Mechanism | Activates MC1-R (melanocortin-1 receptor) → stimulates melanogenesis → promotes melanin production in hair follicles |
| Primary indication | Premature hair graying (Premature Canities) - reverses and prevents gray/white hair |
| Age group | Mainly recommended for ages 8-25 years (premature graying) |
How It Works
- Reactivates dormant melanocytes in hair follicles
- Stimulates melanin synthesis (eumelanin - brown/black)
- Protects against UV-induced DNA damage in follicle cells
- Reduces follicular inflammation that can contribute to graying
Step-by-Step How to Use
Application Protocol (Based on Published Case Report - PMC 2019)
- Part the hair to expose the affected scalp area
- For spray: Spray directly onto the scalp at the gray/white hair areas, holding nozzle close to the scalp
- For gel formulation: Pour approximately 2g (about a teaspoon) directly onto the affected scalp area using two fingers
- Focus on areas with most graying
Dosage & Frequency
| Parameter | Recommendation |
|---|---|
| Frequency | Once daily |
| Amount | ~2g / approx. 8-10 sprays per application |
| Time of application | Evening preferred (leave overnight for maximum absorption) |
| Duration of treatment | 4-6 months minimum before assessing response |
| Full response | Up to 24 months for significant hair repigmentation |
What to Expect - Timeline
| Timeline | Expected Change |
|---|---|
| Weeks 1-4 | No visible change; melanocyte reactivation occurring internally |
| Months 2-3 | New hair growing from gray roots may appear darker at base |
| Months 4-6 | Visible improvement in dark regrowth of treated areas |
| Months 12-24 | Significant repigmentation (>95% conversion seen in published case) |
Patience is essential. Hair grows only ~1 cm/month - colour change at the root takes months to become visible as the hair shaft grows out.
Combine With Oral Hair Supplements
| Nutrient | Role |
|---|---|
| Biotin | Hair shaft structural integrity |
| Calcium pantothenate (B5) | Melanocyte function |
| Copper | Essential cofactor for tyrosinase (melanin synthesis enzyme) |
| Zinc | Antioxidant, follicle health |
| Selenium | Reduces oxidative stress in follicles |
| Folic acid | DNA synthesis in rapidly dividing follicle cells |
| N-acetyl cysteine | Antioxidant, reduces hydrogen peroxide accumulation (key cause of graying) |
Important Notes
| Point | Detail |
|---|---|
| Not a dye | Restores natural melanin - works from the root; does not colour existing gray shafts |
| Evidence level | Limited - mainly case reports and industry studies; RCTs lacking |
| Age relevance | Best evidence in premature graying in young patients (<25 years); less evidence in age-related graying |
| Safe for | Coloured and chemically treated hair |
| Pregnancy | Consult doctor before use |
| No scalp irritation | Generally well tolerated; discontinue if rash develops |
How i can check a pt is pregnant or not
How to Check If a Patient Is Pregnant
TIER 1 - Presumptive Signs
| Sign | Details | When |
|---|---|---|
| Amenorrhoea | Absence of periods - earliest and most important symptom | From conception |
| Morning sickness | Nausea/vomiting, usually morning, resolves in hours | Weeks 4-16 |
| Breast changes | Tingling, tenseness, enlargement, darkened nipples, Montgomery's tubercles, colostrum | From 2nd month |
| Quickening | First fetal movements felt by mother as "fluttering" | Weeks 16-20 |
| Skin pigmentation | Linea nigra, darkening of vulva, abdomen, axillae | 2nd trimester |
| Urinary frequency | Enlarging uterus presses on bladder | Early and late pregnancy |
| Fatigue | Easy tiredness | Early weeks |
| Chadwick's sign | Vaginal mucosa changes from pink → violet → blue due to venous congestion | From week 4 |
| Sympathetic symptoms | Excessive salivation, perverted appetite, mood changes | 1st trimester |
TIER 2 - Probable Signs
| Sign | Details | When |
|---|---|---|
| Abdominal enlargement | Uterus palpable above pelvis from 12 weeks; fundal height correlates with gestation (see below) | >12 weeks |
| Uterine changes | Enlargement, softening, change in shape | 6-8 weeks |
| Hegar's sign | Softening of the lower uterine segment (isthmus) - felt on bimanual examination | 6-10 weeks |
| Goodell's sign | Softening of the cervix | 6 weeks |
| Ballottement | Fetus "bounces" on gentle vaginal/abdominal tap | 4-5 months |
| Braxton Hicks contractions | Intermittent, painless uterine contractions | >4 months |
| Uterine souffle | Soft blowing murmur synchronous with maternal pulse on auscultation over uterus | End of 4th month |
Fundal Height Reference
| Weeks | Fundal Height |
|---|---|
| 12 weeks | Just above symphysis pubis |
| 16 weeks | Midway between symphysis and umbilicus |
| 20 weeks | At umbilicus |
| 28 weeks | Midway between umbilicus and xiphisternum |
| 36 weeks | At xiphoid cartilage |
| 40 weeks | Drops slightly (head engages) |
TIER 3 - Positive/Definitive Signs
| Sign | Details | When |
|---|---|---|
| Fetal heart sounds | Heard with Pinard stethoscope from ~20 weeks; Doppler from ~10-12 weeks | 10-20 weeks |
| Fetal movements felt by examiner | Felt on abdominal palpation | >20 weeks |
| Ultrasound | Gestational sac visible, fetal pole, fetal cardiac activity | From 5-6 weeks (TVS) |
INVESTIGATIONS - Most Important
1. Urine Pregnancy Test (UPT) - FIRST LINE
- Detects beta-hCG in urine
- Sensitivity: Detects hCG from as low as 20-25 mIU/mL
- When positive: As early as 10 days after conception (day of missed period or even a few days before)
- How to do:
- Collect first morning urine (most concentrated, highest hCG)
- Dip test strip or apply 3 drops to well
- Read at 3-5 minutes
- 2 lines = pregnant | 1 line (control only) = not pregnant | no lines = invalid test
- Accuracy: >99% at time of missed period
- False negatives: Too early, dilute urine, expired kit
- False positives: Trophoblastic disease (mole, choriocarcinoma), exogenous hCG
2. Serum Beta-hCG (Quantitative) - GOLD STANDARD
| Feature | Detail |
|---|---|
| Detected from | Day 8-10 post-conception (before missed period) |
| Level in early pregnancy | Doubles every 48-72 hours in normal IUP |
| Discriminatory zone | >1500-2000 mIU/mL → gestational sac should be visible on TVS |
| Use | Early pregnancy, ectopic exclusion, monitoring miscarriage |
3. Ultrasound (USG)
| Timing | Findings |
|---|---|
| 5-6 weeks (TVS) | Gestational sac visible |
| 6 weeks (TVS) | Yolk sac visible |
| 6-7 weeks (TVS) | Fetal pole + cardiac activity |
| 10-12 weeks (TAS) | Fetal heart, CRL measurement |
- TVS (transvaginal) is earlier and more sensitive than transabdominal scan (TAS)
- USG is the only positive definitive sign achievable in early pregnancy
Quick Algorithm for Clinical Practice
Patient with possible pregnancy
|
▼
1. History: Last menstrual period, sexual activity,
symptoms (nausea, breast changes, missed period)
|
▼
2. Urine Pregnancy Test (UPT) - First morning urine
| |
POSITIVE NEGATIVE
| |
▼ ▼
3. Confirm with If suspicion high:
Serum beta-hCG Repeat UPT in 48-72 hrs
+ TVS/USG OR serum beta-hCG
|
▼
4. USG to confirm intrauterine pregnancy
(rule out ectopic), gestational age,
fetal viability (cardiac activity)
Special Note - Relevance to This Patient
- Her period came as expected (late luteal phase sex = low risk)
- But a UPT with first morning urine is still the safest, most reassuring test
- If UPT done <10 days after unprotected sex - repeat at 3 weeks for reliable result
- Norethisterone does not affect hCG levels or UPT results
Her cycle is after 20days so i should wait because is having symptoms like constipation ,cramps , eating a lot but not pica
Understanding the Current Situation
Unprotected sex → Norethisterone taken → Withdrawal bleed came next day
(cycle was due in 3-4 days anyway)
↓
Now: 20 days after that bleed → Symptoms present
Interpreting the Symptoms
| Symptom | Pregnancy? | Alternatively |
|---|---|---|
| Constipation | Yes - progesterone slows gut motility from early pregnancy | Also: PMS, low fibre diet, dehydration |
| Cramps | Yes - early implantation/uterine stretching | Also: Pre-menstrual cramps (her next period is DUE) |
| Increased appetite | Yes - early pregnancy hunger | Also: Luteal phase (PMS) increase in appetite |
| Not pica | Pica = eating non-food items (clay, chalk) - its absence doesn't rule out pregnancy |
Critical insight: These symptoms - constipation, cramps, increased appetite - are identical to late luteal phase / PMS symptoms. Progesterone rises in the luteal phase whether pregnant or not, and causes all three symptoms. You cannot clinically distinguish early pregnancy from PMS based on these symptoms alone.
Should You Wait for the Cycle?
The UPT Can Be Done NOW
- Her last bleed was her actual period (cycle was due, came on time)
- If she had unprotected sex before that period and conceived, implantation would have happened before or during that bleed - making this current cycle already delayed/missed
- Current date is already ~20 days past her last period - this is the perfect window to test
If her cycle is due in 20 days, that means she is currently around Day 7-10 of her new cycle - which means she is either:
- Not pregnant (in which case symptoms = normal luteal/follicular phase)
- Or if she had sex in this current cycle around ovulation (~Day 14) - it is too early to test yet
What You Need to Clarify
Did she have unprotected sex again after the withdrawal bleed / after her period?
| Scenario | When to Test |
|---|---|
| Sex was only before the period that already came | Very low risk - test now if she wants reassurance; likely negative |
| Sex after the period (in this current cycle) | Wait until Day 1 of missed period - i.e., in ~20 days as you say |
| Sex around Day 10-14 of this current cycle | Test 14 days after that sex (or at missed period) |
Current Symptoms Explanation - Most Likely
- Constipation → could be dietary, or early follicular phase
- Cramps → possibly ovulation pain (Mittelschmerz) if she is around Day 14, or residual from the recent bleed
- Increased appetite → very common in follicular phase as oestrogen rises; also common around ovulation
Practical Advice
| Action | Timing |
|---|---|
| Reassure now | Symptoms are consistent with normal cycle |
| Do UPT if she is anxious | Can do now - if negative at Day 20+, very reassuring |
| Repeat UPT if next period is missed | On Day 1 of missed period = most accurate |
| Counsel on contraception | This is the third time unprotected sex has come up - she needs reliable contraception going forward |
| Watch for red flags | Severe one-sided pelvic pain + bleeding = rule out ectopic (though very unlikely here) |
Sugar medication can be taken before food?
Diabetes Medications - Timing in Relation to Food
🔴 BEFORE Food (15-30 mins pre-meal)
| Drug | Why Before Food |
|---|---|
| Glipizide (Glucotrol) | Stimulates insulin release - needs to act before glucose load arrives; take 30 min before meal |
| Glimepiride | Sulfonylurea - take with first bite or 15-30 min before breakfast |
| Repaglinide (Prandin) | Rapid-acting secretagogue - take 0-30 min before each meal; skip if skipping meal |
| Nateglinide (Starlix) | Take 1-30 min before meals; skip if meal skipped |
| Short-acting insulin (Regular) | Inject 30 min before meal |
| Rapid-acting insulin (Lispro, Aspart, Glulisine) | Inject 0-15 min before meal or immediately before |
⚠️ Sulfonylureas and meglitinides taken before food without eating = hypoglycaemia risk
🟡 WITH Food (first bite of meal)
| Drug | Why With Food |
|---|---|
| Metformin | Reduces GI side effects (nausea, diarrhoea) significantly when taken with meals; take with or after food |
| Glyburide/Glibenclamide | Take with breakfast or first main meal |
| Acarbose / Miglitol | Alpha-glucosidase inhibitors - MUST be taken with first bite of food; delays carbohydrate digestion at the intestinal brush border - useless if not taken with meal |
| Pioglitazone (Actos) | Thiazolidinedione - can be taken with or without food, but WITH food reduces GI upset |
🟢 ANY TIME (Meal-Independent)
| Drug | Notes |
|---|---|
| Metformin XR (extended release) | With evening meal to reduce GI side effects; otherwise flexible |
| Sitagliptin (DPP-4 inhibitor) | With or without food - no meal timing requirement |
| Vildagliptin, Saxagliptin, Alogliptin | With or without food |
| Empagliflozin, Dapagliflozin, Canagliflozin (SGLT2 inhibitors) | With or without food |
| Long-acting insulin (Glargine, Detemir, Degludec) | Same time each day - no relation to meals |
| GLP-1 agonists (Liraglutide, Dulaglutide - weekly injections) | Meal-independent |
Quick Summary Reference
| Drug Class | Example | Timing |
|---|---|---|
| Biguanide | Metformin | With or after food |
| Sulfonylurea (short-acting) | Glipizide | 30 min BEFORE food |
| Sulfonylurea (long-acting) | Glimepiride, Glyburide | With first meal |
| Meglitinide | Repaglinide | 0-30 min BEFORE each meal |
| Alpha-glucosidase inhibitor | Acarbose | With FIRST BITE of meal |
| Thiazolidinedione | Pioglitazone | With or without food |
| DPP-4 inhibitor | Sitagliptin | With or without food |
| SGLT2 inhibitor | Empagliflozin | With or without food |
| GLP-1 agonist (daily) | Liraglutide | Before any meal (consistent time) |
| Rapid insulin | Novorapid | 0-15 min BEFORE meal |
| Regular insulin | Actrapid | 30 min BEFORE meal |
| Basal insulin | Glargine | Meal-independent (fixed time) |
Most Common in Indian Practice - Quick Recall
| Drug | Timing |
|---|---|
| Metformin 500/850/1000mg | After food - always, to prevent nausea |
| Glimepiride 1/2mg | Before breakfast |
| Glipizide 5mg | 30 min before food |
| Voglibose/Acarbose | With first bite of meal |
| Sitagliptin (Januvia) | Any time |
| Empagliflozin (Jardiance) | Any time (morning preferred) |
| Fixed dose combos (Metformin + Glimepiride) | After food (metformin timing takes priority) |
Key teaching point: When a fixed-dose combination contains metformin (e.g., Metformin + Glimepiride, Metformin + Sitagliptin), the instruction is always "after food" to protect against metformin-induced GI side effects - the metformin timing overrides the sulfonylurea timing in practice.
Metformin sr 500
Metformin SR 500mg - Complete Guide
What is SR (Sustained Release)?
| Feature | Metformin IR | Metformin SR 500 |
|---|---|---|
| Release | Immediate | Slow, over 6-8 hours |
| Frequency | 2-3 times daily | Once or twice daily |
| GI side effects | More common | Significantly less |
| Absorption | Proximal small bowel | Proximal colon |
| Efficacy | Equal | Equal |
When to Take It
✅ Take WITH or IMMEDIATELY AFTER the evening meal
- Always take with food - this is non-negotiable for SR formulation
- Evening meal preferred - reduces overnight GI discomfort and gives best absorption
- Taking on empty stomach = higher peak concentration = nausea, diarrhoea, bloating
- Do NOT crush or chew the SR tablet - it destroys the slow-release mechanism; swallow whole
Mechanism of Action
| Action | Effect |
|---|---|
| ↓ Hepatic gluconeogenesis | Primary action - reduces fasting blood glucose (excess liver glucose = main cause of high FBS in T2DM) |
| ↓ Intestinal glucose absorption | Slows sugar absorption from gut |
| ↑ Peripheral glucose uptake | Improves insulin sensitivity in muscle |
| Does NOT stimulate insulin secretion | Therefore no hypoglycaemia risk when used alone |
Dosing Schedule
| Phase | Dose | Timing |
|---|---|---|
| Starting dose | 500mg SR once daily | With evening meal |
| After 1-2 weeks | 500mg SR twice daily | With lunch + dinner |
| Titrate up | 1000mg SR once daily at night | With dinner |
| Maximum | 2000mg SR per day | Divided doses with meals |
Start low, go slow - this minimises GI side effects during initiation
Indications
- Type 2 Diabetes Mellitus - first-line drug of choice (ADA/AHA guidelines)
- Prediabetes - prevents progression to T2DM
- PCOS - reduces insulin resistance, lowers androgens, restores ovulation
- Metabolic syndrome - off-label but widely used
Side Effects
| Side Effect | Details |
|---|---|
| GI symptoms (nausea, diarrhoea, abdominal bloating) | Most common; SR formulation significantly reduces this vs IR; take with food |
| Metallic taste | Common initially, resolves |
| Anorexia / weight loss | Beneficial in obese T2DM patients |
| Vitamin B12 deficiency | Long-term use; monitor B12 levels annually especially if anaemia or neuropathy develops |
| Lactic acidosis | Rare but potentially fatal; risk mainly with renal failure |
Contraindications
| Contraindication | Reason |
|---|---|
| eGFR <30 mL/min/1.73m² (severe renal failure) | Risk of lactic acidosis - drug accumulates |
| eGFR 30-45 | Use with caution; reduce dose |
| IV contrast dye procedures | Stop 48 hours before; restart 48 hours after (risk of contrast nephropathy → lactic acidosis) |
| Acute MI, sepsis, heart failure exacerbation | Acute renal failure risk |
| Alcohol excess | Increases lactic acidosis risk |
| Hepatic failure | Impaired lactate clearance |
Key Patient Instructions
| Instruction | Why |
|---|---|
| ✅ Take with evening meal, swallow whole | Reduces GI side effects, maintains SR coating |
| ✅ Never skip meals while on metformin | Increases GI side effects |
| ✅ Drink adequate water | Prevents GI issues |
| ❌ Do not crush/chew | Destroys slow-release mechanism → rapid dump of full dose → severe GI reaction |
| ❌ Do not take on empty stomach | Nausea, diarrhoea |
| ✅ Annual B12 monitoring | Long-term use depletes B12 |
| ✅ Check kidney function (eGFR) before starting and annually | Lactic acidosis prevention |
Monitoring Parameters
| Parameter | Frequency |
|---|---|
| HbA1c | Every 3 months until target, then 6-monthly |
| Fasting blood glucose | Weekly initially, then monthly |
| Serum creatinine / eGFR | Before starting, then annually |
| Vitamin B12 | Annually (especially after 3+ years of use) |
| LFTs | Baseline |
Bottom line for Metformin SR 500: Take ONE tablet with evening dinner, swallow whole, never on empty stomach. It does NOT cause hypoglycaemia alone. Start with once daily and increase as tolerated. It is the safest, most evidence-based first-line diabetes drug available.
Metformin500 can be taken before food?
Metformin 500mg - Before Food?
Short Answer: No - not recommended
Metformin IR (Immediate Release) 500mg
| Timing | What Happens |
|---|---|
| Before food (empty stomach) | Drug absorbs rapidly → high peak concentration → nausea, vomiting, diarrhoea, abdominal cramps in most patients |
| With food (first bite) | Food slows absorption → lower peak concentration → GI side effects significantly reduced |
| After food | Also acceptable - slightly lower peak, further reduces GI upset |
Textbook recommendation (Lippincott Pharmacology): "GI adverse effects can be alleviated by titrating the dose slowly and administering the drug with meals."
Metformin SR 500mg
- SR coating controls release over 6-8 hours
- Food in the stomach is necessary for proper, gradual absorption
- Empty stomach = disrupts release profile + worsens GI side effects
Why Metformin Causes GI Problems Without Food
- Direct irritation of the gastric and intestinal mucosa
- Faster transit → less absorption but more irritation
- Higher local drug concentration in the gut wall → nausea, loose stools
Correct Instruction to Give Patient
| Formulation | Timing |
|---|---|
| Metformin 500 IR | With the first bite of food or during the meal |
| Metformin 500 SR | With or immediately after evening meal; swallow whole |
Simple rule to tell patients: "Never take Metformin on an empty stomach. Always take it with your food - not before, not 1 hour after. With food means with food."
23y old female pt came to the opd with left side abdominal pain
Create a clinical assessment checklist for left-sided abdominal pain in young women