Staphylococcus pneumonia full details for md exams 15marks answer from fishman and murray and recent guidelines
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Staphylococcus aureus" AND "pneumonia" AND "guidelines"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"MRSA" AND "pneumonia" AND "treatment"
Loading Image
Finding Sources
Reading File
Reading File
This is a full, exam-ready 15-mark answer on Staphylococcal Pneumonia drawn directly from the four authoritative textbooks and supplemented with the latest evidence. Here is a breakdown of what is covered:
Structure of the answer (MD exam format):
- Introduction & Microbiology - Gram stain, MSSA vs CA/HA-MRSA distinction
- Epidemiology - EPIC/GLIMP study data, risk groups (post-influenza, IVDU, dialysis, healthcare workers)
- Pathogenesis - AGR quorum sensing, PVL, alpha-toxin, ADAM10/E-cadherin, SCCmec/mecA, post-influenza synergy (from Fishman's)
- Classification - CAP (inhaled), HAP/VAP, Hematogenous (septic emboli)
- Pathology - Bronchopneumonia pattern, pneumatoceles, abscess, empyema
- Clinical Features - Standard CAP presentation + the distinctive necrotizing CA-MRSA syndrome with leukopenia and 75% mortality
- Radiology - Including the Murray & Nadel chest X-ray image of hematogenous type showing bilateral cavities
- Diagnosis - Gram stain intracellular cocci, nasal MRSA PCR stewardship
- MRSA Risk Scoring - GLIMP criteria (Fishman's Table 128-1)
- Complications - Empyema, abscess, bacteremia, metastatic spread
- Treatment - MSSA (oxacillin/cefazolin), MRSA (vancomycin/linezolid), duration table, daptomycin contraindication, necrotizing pneumonia IVIG protocol, Fishman's treatment table
- HAP/VAP - De-escalation with nasal MRSA PCR
- Prevention & Prognosis
- Summary table for rapid revision
Give me answer
The full, detailed 15-mark answer is already written above in my previous response. Here is the complete answer again, cleanly formatted:
Staphylococcal Pneumonia - 15 Marks MD Exam Answer
(Sources: Murray & Nadel, Fishman's, Goldman-Cecil, Robbins & Kumar, IDSA/ATS Guidelines)
1. Introduction & Microbiology
Staphylococcus aureus is a large gram-positive coccus arranged in grape-like clusters. It causes both community-acquired pneumonia (CAP) and hospital-acquired pneumonia (HAP/VAP). Two clinically critical subtypes:
- MSSA - methicillin-susceptible S. aureus
- MRSA - methicillin-resistant S. aureus (CA-MRSA and HA-MRSA; USA300 is the dominant CA-MRSA clone causing necrotizing pneumonia)
2. Epidemiology
- Accounts for 1-1.7% of all CAP cases (MSSA 1.0%, MRSA 0.7% in EPIC study)
- 3% of CAP in the GLIMP international study (54 countries)
- ~80% of S. aureus CAP hospitalizations in the US were MRSA (2009-2012)
- 2nd-3rd leading cause of CAP requiring ICU admission
- 30-50% of healthy adults carry S. aureus transiently in anterior nares (healthcare workers higher)
High-Risk Populations:
- Post-influenza infection (most important predisposing factor)
- Post-measles (children); HIV infection
- IV drug users - hematogenous seeding from right-sided endocarditis
- Hemodialysis patients, diabetics
- Nursing home residents; recent hospitalization
- Neonates, premature infants, immunocompromised patients
3. Pathogenesis & Virulence Factors
Virulence is regulated by the accessory gene regulator (agr) - a quorum-sensing system linking bacterial density to exoprotein production.
A. Surface Components
| Factor | Role |
|---|---|
| Microcapsule | Anti-phagocytic |
| Teichoic & lipoteichoic acids | TLR-mediated innate immune activation |
| MSCRAMM | Adhesion to fibronectin, fibrinogen on denuded epithelium (critical post-influenza) |
| Biofilm | Antibiotic tolerance; chronic infection |
B. Key Exotoxins
| Toxin | Action |
|---|---|
| PVL (Panton-Valentine Leukocidin) | Pore-forming; lyses neutrophils and macrophages; KEY factor in necrotizing pneumonia |
| Alpha-toxin | Disrupts epithelial tight junctions via ADAM10/E-cadherin degradation; induces necroptosis; inhibits efferocytosis |
| Alpha-phenol soluble modulins, LukAB | Pore-forming; necroptosis of alveolar macrophages via RIPK1/RIPK3 |
| Superantigens (TSST-1, enterotoxins) | Massive T-cell activation; cytokine storm |
C. Immune Evasion
- Inhibits C5a-mediated chemotaxis
- Resists phagocyte microbicidal responses
- Prevents phagolysosomal maturation in macrophages
- IL-17-driven dysregulated neutrophil inflammation causes lung injury
D. Methicillin Resistance
- mecA gene encodes low-affinity PBP2a (penicillin-binding protein 2a)
- Carried on staphylococcal chromosome cassette (SCCmec)
- PBP2a has very low affinity for all beta-lactams - making MRSA resistant to entire class
E. Post-Influenza Synergy (Fishman's)
- Influenza neuraminidase cleaves sialic acid, exposing receptors for staphylococcal adherence
- Virus upregulates α5β1 integrin and ethylenated glycans promoting S. aureus binding
- Denuded epithelium + fibrin deposition stabilizes bacterial adhesion
4. Classification
| Type | Route | Setting | Key Feature |
|---|---|---|---|
| CAP (inhaled) | Aspiration from nasopharynx | Community | Post-influenza; young adults with necrotizing form |
| HAP/VAP | Aspiration of colonized secretions | Hospital, ICU | HA-MRSA; ventilated patients |
| Hematogenous | Septic emboli via bloodstream | IV drug users, endocarditis | Multiple bilateral lower lobe cavities |
5. Pathology
- Pattern: Suppurative (purulent) bronchopneumonia; patchy lobular consolidation, bilateral
- Microscopy: Alveoli filled with neutrophils and pus; liquefactive necrosis
- Pneumatoceles: Thin-walled air-filled cysts from check-valve bronchial obstruction - especially in children; may cause pneumothorax
- Lung abscess: Cavitation from tissue destruction
- Empyema: Purulent pleural effusion - high incidence (characteristic complication)
- Hematogenous pattern: Multiple bilateral septic emboli with central necrosis/cavitation, lower lobe predilection
"Staphylococcal pneumonia is associated with a high incidence of complications such as lung abscess and empyema." - Robbins & Kumar
6. Clinical Features
Standard Presentation
- Acute-onset high fever, rigors, myalgia
- Productive cough - purulent, often blood-tinged sputum
- Pleuritic chest pain
- Progressive dyspnea - may rapidly worsen
- Often preceded by 5-10 days of influenza-like illness
Necrotizing CAP Syndrome (CA-MRSA / PVL-positive strains)
Distinctive, fulminant syndrome in young, previously healthy adults and children:
- Short flulike prodrome (preceding skin/soft tissue infection in ~20%)
- Fulminant respiratory failure requiring mechanical ventilation in ~60%
- Hemoptysis in ~40% (from pulmonary necrosis)
- Leukopenia (WBC ≤3,000/μL) - hallmark; associated with mortality up to 75%
- Shock, multiorgan failure
Hematogenous Pneumonia
- Respiratory symptoms mild or absent
- Pleuritic chest pain + hemoptysis if pulmonary infarction from septic embolus
- Features of underlying endocarditis predominate (new murmur, Osler nodes, Janeway lesions, fever)
7. Radiological Features
Chest X-Ray
Bronchopneumonic (inhaled) form:
- Bilateral, patchy, multilobar airspace opacities
- Frequent cavitation
- Pleural effusion/empyema
- Pneumatoceles (thin-walled cysts) - classic in children
Hematogenous form:
- Multiple discrete nodular/cavitary shadows
- Lower lobe predilection (gravity + blood flow)
- Bilateral distribution
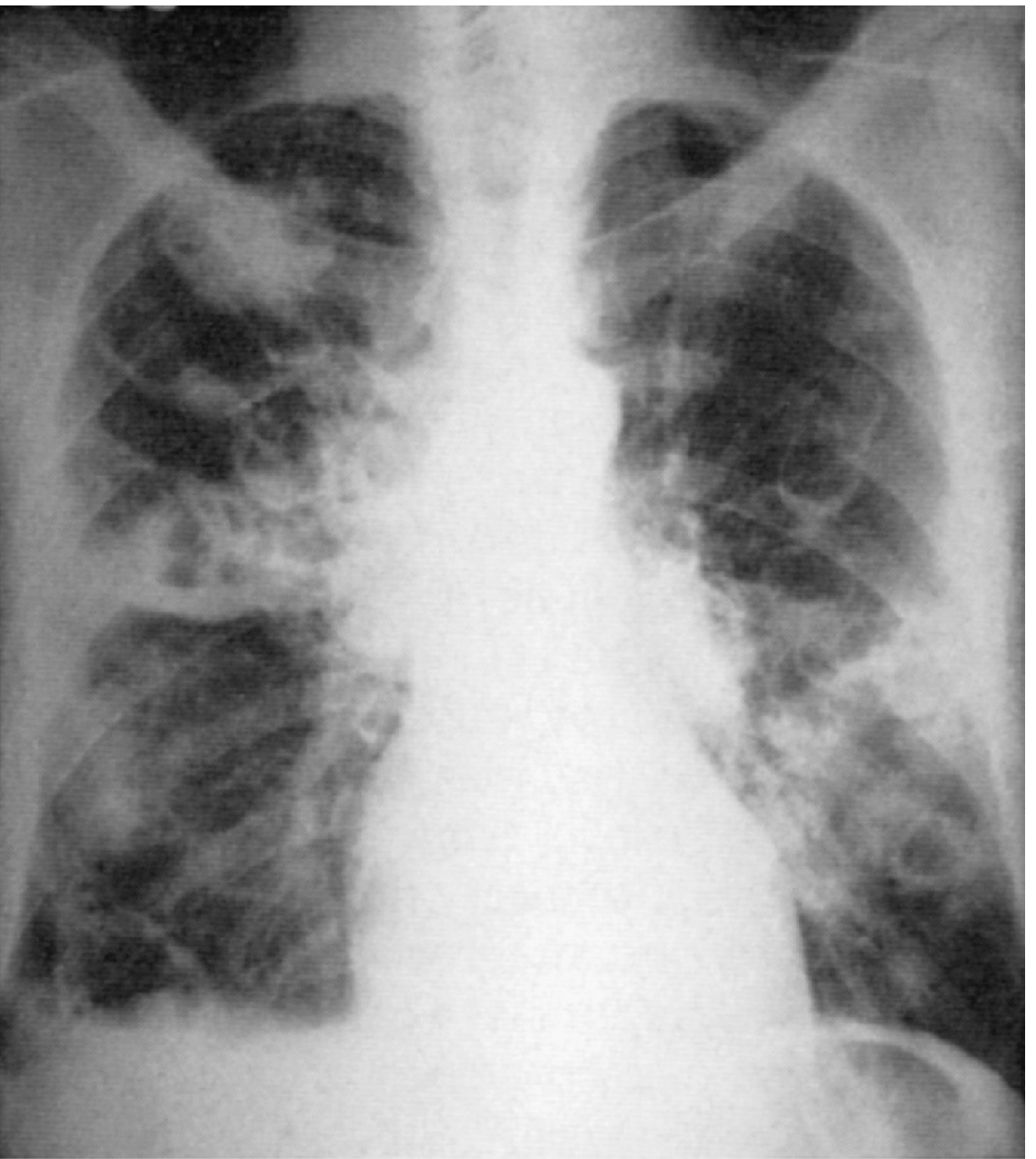
Chest X-ray (Murray & Nadel eFig 46.20): Hematogenous staphylococcal pneumonia showing multiple bilateral cavitary lesions from septic emboli in bacterial endocarditis.
CT chest: More sensitive; shows multilobar consolidation, cavities, tree-in-bud pattern, pleural collections.
8. Diagnosis
| Investigation | Finding / Significance |
|---|---|
| WBC | Leukocytosis (usual); leukopenia = ominous in CA-MRSA |
| Sputum Gram stain | Multiple clusters of large gram-positive cocci, intracellular = strong evidence |
| Sputum culture | S. aureus on blood agar (golden/hemolytic); sensitivity testing (MRSA vs MSSA) |
| Blood cultures | Positive in bacteremia; mandatory in all severe cases |
| Nasal MRSA PCR/swab | Negative result has NPV >96% - rules out MRSA pneumonia; guides de-escalation |
| Pleural fluid | Exudate; low pH/glucose, high LDH; culture if empyema |
| BAL / bronchoscopy | Non-responding cases, immunocompromised, VAP |
9. Risk Factors for MRSA-CAP (GLIMP Study - Fishman's Table 128-1)
Independent risk factors:
- Prior MRSA infection or colonization (strongest predictor)
- Recurrent skin infections
- Severe CAP (ICU admission, cavities, empyema)
Additional: prior hospitalization + IV antibiotics within 90 days, hemodialysis, diabetes, nursing home resident
10. Complications
- Empyema - most common; requires drainage + antibiotics
- Lung abscess - cavitation; prolonged therapy
- Pneumatoceles - especially children; pneumothorax risk
- Bacteremia + metastatic foci: CNS abscess/meningitis, osteomyelitis, septic arthritis, renal abscess
- ARDS - especially necrotizing form
- Septic shock - direct bacterial + toxin-mediated
- Persistent fever - from undrained empyema or cavitary disease (poor local antibiotic penetration)
11. Treatment
For MSSA (Drug of Choice - Murray & Nadel / Goldman-Cecil)
- Oxacillin 8-12 g/day IV or Nafcillin 2 g IV q4h - penicillinase-resistant penicillin
- Cefazolin 2 g IV q8h - equal efficacy, better tolerability
- No other antibiotic, including vancomycin, is as safe or as effective as a beta-lactam for MSSA
- Penicillin-allergic: Clindamycin or Linezolid
For MRSA (IDSA/ATS Guidelines / Murray & Nadel)
| Drug | Dose | Remarks |
|---|---|---|
| Vancomycin | 15 mg/kg IV q12h; target AUC 400-600 μg·h/mL | Drug of choice; MIC shift upward over decades - MIC >1 μg/mL = clinical failure |
| Linezolid | 600 mg IV/PO q12h | Preferred for VAP, renal failure, rising vancomycin MIC; also suppresses toxin production |
| Clindamycin | 600 mg TID IV/PO | Alternative if sensitive + less severe disease; reduces PVL/NETs-degrading nuclease production |
Add MRSA coverage empirically if:
- Prior respiratory isolation of MRSA
- Recent hospitalization + IV antibiotics within 90 days
- Severe CAP requiring ICU after antecedent influenza (Goldman-Cecil)
Necrotizing CAP with PVL-positive MRSA (European Guidelines)
High-dose Linezolid + Clindamycin + Rifampicin + IV Immunoglobulin (IVIG) in especially severe cases
Duration of Therapy (Goldman-Cecil)
| Scenario | Duration |
|---|---|
| Uncomplicated pneumonia | 7-14 days |
| With uncomplicated bacteremia | 14 days |
| With endocarditis / lung abscess | ≥4 weeks |
| With empyema | Prolonged + drainage mandatory |
Drugs to AVOID
- Daptomycin - CONTRAINDICATED in pulmonary infections; inactivated by binding to pulmonary surfactant
Emerging Agents (Fishman's)
- Ceftaroline (600 mg IV q12h) - anti-MRSA cephalosporin via PBP2a inhibition; salvage/combination therapy (PMID 37852658, 2023 systematic review)
- Ceftobiprole - European approval for HAP + CAP; noninferior to ceftriaxone ± linezolid
Fishman's CAP Treatment Table (IDSA/ATS 2019)
| Group | Regimen |
|---|---|
| Outpatient, healthy, no risk factors | Amoxicillin or doxycycline or macrolide |
| Outpatient with comorbidities | Amoxicillin-clavulanate/cephalosporin + macrolide OR respiratory fluoroquinolone |
| Inpatient non-severe CAP | beta-lactam + macrolide OR respiratory fluoroquinolone |
| Severe CAP | beta-lactam + macrolide OR beta-lactam + fluoroquinolone |
| Empiric MRSA coverage | Vancomycin or Linezolid |
HAP/VAP (de-escalation)
- Empiric vancomycin/linezolid if MRSA prevalence >10-20%, or severe illness
- De-escalate within 48-72h if cultures negative AND nasal MRSA PCR negative (NPV >96%; PMID 41338060, 2026 meta-analysis)
12. Prevention
- Influenza vaccination - single most important preventive measure
- Contact precautions + hand hygiene for MRSA
- Decolonization in high-risk patients: mupirocin nasal ointment + chlorhexidine washes
- Judicious antibiotic use (antimicrobial stewardship)
13. Prognosis
| Scenario | Mortality |
|---|---|
| MSSA CAP (EPIC study) | ~4% |
| MRSA CAP (EPIC study) | ~13% |
| Post-influenza MRSA CAP | Higher than baseline |
| Necrotizing CAP + leukopenia | Up to 75% |
| HAP/VAP MRSA | High; complicated by bacteremia |
Quick Revision Summary
| Key Point | Answer |
|---|---|
| Gram stain | Gram-positive cocci in clusters |
| Nasal carriage | 30-50% of adults |
| Most important predisposing factor | Post-influenza |
| Key toxin in necrotizing pneumonia | PVL (Panton-Valentine Leukocidin) |
| MRSA resistance mechanism | mecA gene → PBP2a → SCCmec cassette |
| Pathognomonic CXR finding | Pneumatoceles (children); bilateral lower lobe cavities (hematogenous) |
| Ominous lab sign | Leukopenia ≤3000/μL in CA-MRSA |
| Sputum Gram stain clue | Intracellular clusters of gram-positive cocci |
| MSSA treatment | Oxacillin / Nafcillin / Cefazolin |
| MRSA treatment | Vancomycin or Linezolid |
| Drug to NEVER use | Daptomycin (surfactant inactivation) |
| Preferred in VAP | Linezolid > Vancomycin |
| Key complications | Empyema, lung abscess, bacteremia, pneumatoceles |
| Duration (uncomplicated) | 7-14 days |
| Duration (abscess/endocarditis) | ≥4 weeks |
References: Murray & Nadel's Textbook of Respiratory Medicine (pp. 1004-1006, Ch. 46); Fishman's Pulmonary Diseases and Disorders (Ch. 128, Table 128-1, 128-6); Goldman-Cecil Medicine (Ch. 267, pp. 3299-3321); Robbins & Kumar Pathologic Basis of Disease (pp. 468, 3454); IDSA/ATS CAP Guidelines 2019 (Metlay et al., AJRCCM 200:e45-e67)
This is a shared conversation. Sign in to Orris to start your own chat.