Alveolar-Arterial (A-a) Gradient - Complete Answer for MD Exams
Definition
The Alveolar-Arterial (A-a) oxygen gradient is the difference between the partial pressure of oxygen in the alveolus (PAO2) and the partial pressure of oxygen in the systemic arterial blood (PaO2).
A-a gradient = PAO2 - PaO2
It is the single most useful index for evaluating the efficiency of oxygen transfer across the lung. A normal lung has minimal difference between alveolar and arterial PO2; when this gradient widens, it signals a defect in O2 equilibration between alveolar gas and pulmonary capillary blood.
The Alveolar Gas Equation (Essential for Calculating PAO2)
PAO2 cannot be measured directly - it is calculated using the Alveolar Gas Equation:
PAO2 = FiO2 x (PB - PH2O) - (PaCO2 / R)
Where:
- FiO2 = fraction of inspired oxygen (0.21 on room air)
- PB = barometric pressure (760 mm Hg at sea level)
- PH2O = water vapor pressure at body temperature (47 mm Hg)
- PaCO2 = arterial CO2 tension (assumed equal to alveolar CO2 = 40 mm Hg normally)
- R = respiratory quotient (0.8 on a mixed diet)
At sea level on room air - simplified form:
PAO2 = 150 - (PaCO2 / 0.8) = 150 - (1.25 x PaCO2)
With normal PaCO2 of 40 mm Hg:
PAO2 = (0.21 x [760 - 47]) - (40 / 0.8) = ~100 mm Hg
Therefore:
A-a gradient = PAO2 - PaO2 = 100 - 95 = ~5 mm Hg (normal)
Normal Values
| Age (years) | Upper limit of normal A-a gradient (mm Hg) |
|---|
| 20 | 17 |
| 30 | 20 |
| 40 | 23 |
| 50 | 26 |
| 60 | 30 |
| 70+ | ~35 |
General rule for upper limit of normal:
Normal A-a gradient = (Age + 10) / 4
Range at rest on room air: 5-15 mm Hg (young adults), up to 25 mm Hg (elderly).
Important: Normal A-a gradient increases with:
- Age - due to progressive V/Q mismatch from loss of lung elasticity
- Increasing FiO2 - breathing supplemental O2 widens the measurable gradient
Physiological Basis - Why Does a Normal A-a Gradient Exist?
Even in healthy lungs, a small A-a gradient of 5-15 mm Hg exists because of:
- Physiological V/Q mismatch - ventilation and perfusion are not perfectly matched throughout the lung (apex vs. base differences)
- Anatomic shunts - bronchial veins and Thebesian veins drain directly into the left side of the circulation, bypassing alveolar gas exchange (~2-3% of cardiac output)
- Diffusion limitation - minimal at rest but becomes relevant in disease
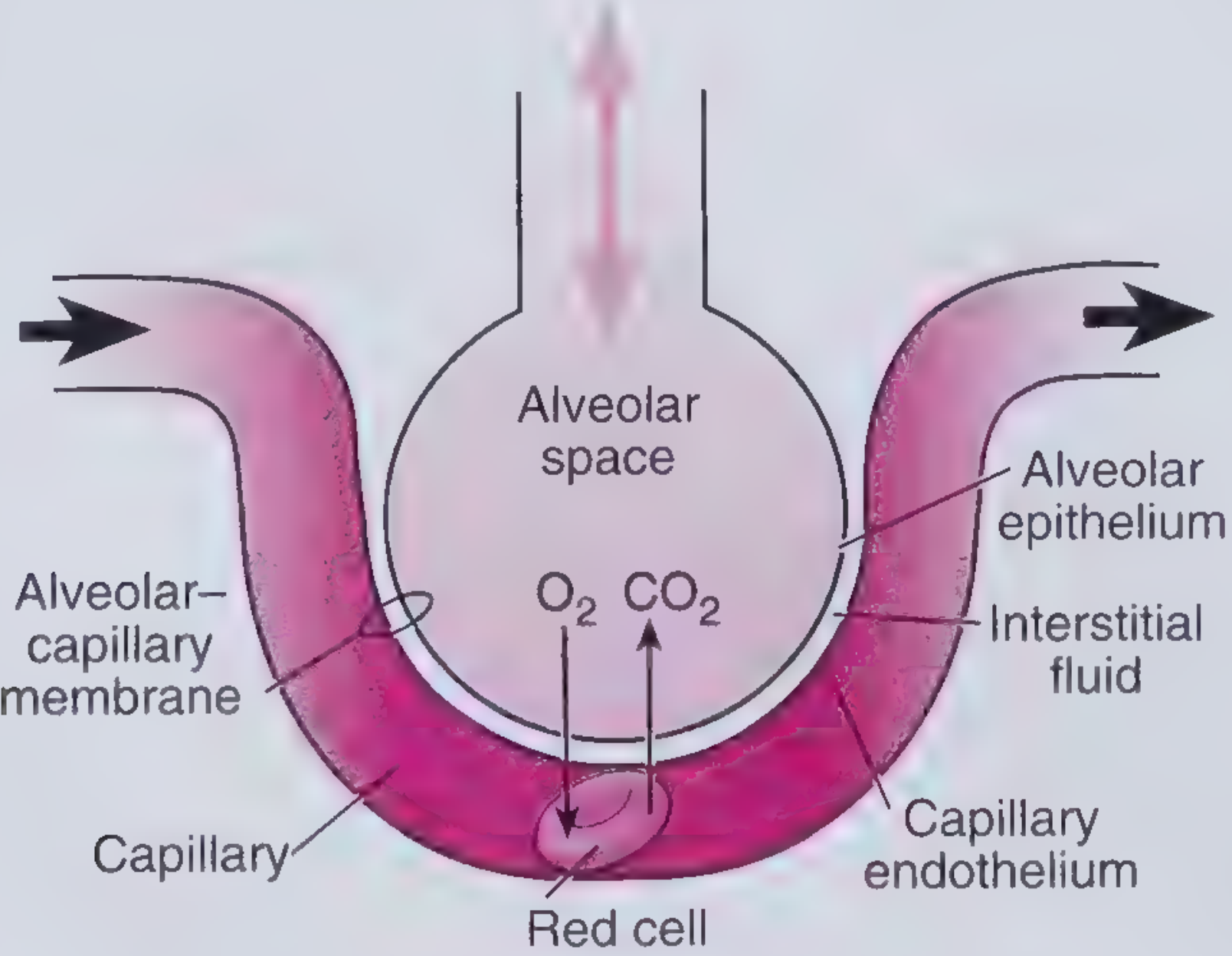
Gas exchange at the alveolar-capillary interface
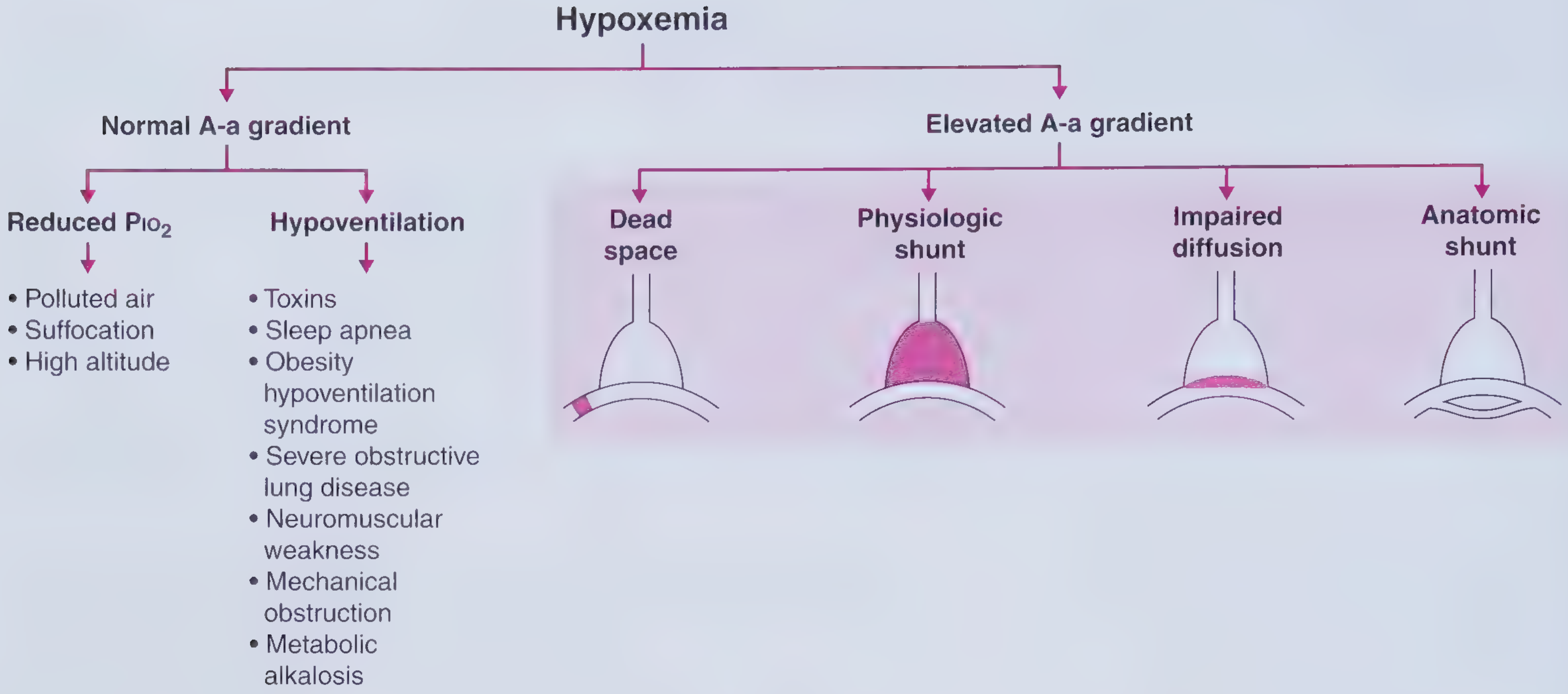
Classification of Hypoxemia by A-a Gradient
A. Hypoxemia with NORMAL A-a Gradient
The lung is intrinsically normal - the problem is insufficient inspired O2 or reduced alveolar ventilation. O2 equilibrates normally across the alveolar-capillary membrane, so PAO2 and PaO2 fall together.
| Mechanism | Explanation | Examples |
|---|
| Reduced PiO2 | Decreased FiO2 or decreased barometric pressure reduces both alveolar and arterial PO2 equally | High altitude, smoke inhalation, suffocation |
| Hypoventilation | Less fresh air enters alveoli per breath; CO2 accumulates and displaces O2. Equilibration is intact so PaO2 falls equally. PaCO2 is elevated | Opioid/sedative overdose, neuromuscular disease, sleep apnea, obesity hypoventilation syndrome, mechanical obstruction, metabolic alkalosis |
Key feature: Both conditions respond well to supplemental O2.
B. Hypoxemia with ELEVATED (Widened) A-a Gradient
The lung itself is diseased - O2 does not equilibrate fully across the alveolar-capillary barrier. PaO2 falls disproportionately compared to PAO2.
1. V/Q Mismatch (Most Common Cause)
- Ventilation and perfusion are mismatched in different lung regions
- Low V/Q regions (perfusion > ventilation): blood passes alveoli with low O2 tension - poorly oxygenated blood enters systemic circulation
- High V/Q regions (dead space physiology): wasted ventilation
- The admixture of blood from low V/Q regions drags down overall PaO2
- Examples: COPD, asthma, pneumonia, pulmonary embolism
- Responds to supplemental O2
2. Right-to-Left Shunt
- Deoxygenated blood bypasses ventilated alveoli entirely (V/Q = 0)
- Anatomic shunt: ASD with reversed shunt, VSD, pulmonary AVM, hepatopulmonary syndrome
- Physiologic shunt: lobar pneumonia, complete atelectasis, ARDS (flooded/collapsed alveoli)
- Hallmark: PaO2 does NOT improve significantly with 100% O2 - this distinguishes shunt from all other causes. Even breathing 100% O2, shunted blood remains unoxygenated and mixes with oxygenated blood, limiting the PaO2 rise
3. Diffusion Impairment
- Thickening of the alveolar-capillary membrane increases diffusion distance, reducing O2 transfer
- O2 does not fully equilibrate across the membrane before blood exits the capillary
- Examples: interstitial pulmonary fibrosis, pulmonary edema, sarcoidosis
- Responds to supplemental O2 (raising driving force for diffusion)
4. Increased Dead Space (V/Q mismatch subtype)
- Pulmonary embolism is the classic example: normal ventilation with no perfusion (V/Q = infinity)
- Embolized lung contributes to dead space; remaining vascular bed receives excess perfusion, creating V/Q mismatch in adjacent lung regions
- Results in widened A-a gradient plus hypocapnia (compensatory hyperventilation)
Summary Table: A-a Gradient in Different Causes of Hypoxemia
| Mechanism | PaO2 | PaCO2 | A-a Gradient | Response to O2 |
|---|
| High altitude | Low | Normal or low | Normal | Yes |
| Hypoventilation | Low | High | Normal | Yes |
| V/Q mismatch | Low | Normal or low | Increased | Yes |
| Diffusion defect | Low | Normal | Increased | Yes |
| Right-to-left shunt | Low | Normal or low | Increased | Limited |
Clinical Uses of the A-a Gradient
1. Differentiating Causes of Hypoxemia
The primary clinical use. A normal A-a gradient immediately localizes the problem to hypoventilation or reduced inspired O2, sparing the need for extensive lung workup.
2. Diagnosing Pulmonary Embolism
- PE causes a widened A-a gradient from dead space V/Q mismatch and often hypocapnia
- ABG showing hypoxemia + respiratory alkalosis + widened A-a gradient raises suspicion for PE
- However, a normal A-a gradient does not exclude PE (can be normal in a minority of cases)
3. Assessing Severity of Lung Disease
- The magnitude of gradient widening reflects the degree of V/Q mismatch
- Used in ICU for serial monitoring - tracks progression or improvement in ARDS, pneumonia, respiratory failure
- In mild pulmonary disease: A-a gradient < 35 mm Hg; in severe disease: > 35 mm Hg (e.g., Pneumocystis pneumonia severity grading)
4. Distinguishing Shunt from Other Causes (100% O2 Test)
- If PaO2 rises to >400-500 mm Hg on 100% O2, there is no significant shunt
- If PaO2 remains low despite 100% O2, an anatomic or physiologic shunt is present
5. Detecting Occult Lung Disease
- A widened A-a gradient on ABG in a patient with normal spirometry suggests underlying parenchymal or vascular disease
Worked Numerical Examples (High-Yield for Exams)
Case 1 - Hypoventilation (e.g., opioid overdose):
- PaO2 = 70, PaCO2 = 60 on room air
- PAO2 = 150 - (1.25 x 60) = 150 - 75 = 75 mm Hg
- A-a gradient = 75 - 70 = 5 mm Hg → Normal
- Interpretation: pure hypoventilation; lungs are intrinsically normal
Case 2 - V/Q Mismatch (e.g., pneumonia):
- PaO2 = 70, PaCO2 = 40 on room air
- PAO2 = 150 - (1.25 x 40) = 150 - 50 = 100 mm Hg
- A-a gradient = 100 - 70 = 30 mm Hg → Widened
- Interpretation: lung parenchymal/vascular disease
Factors That Affect the A-a Gradient
| Factor | Effect on A-a Gradient |
|---|
| Increasing age | Increases |
| Increasing FiO2 | Increases |
| Exercise | Slightly increases |
| Supine position | Decreases (more uniform perfusion) |
| Obesity | Increases |
Key Points to Remember for MD Exams
- Formula: A-a gradient = PAO2 - PaO2; PAO2 is calculated, PaO2 is measured on ABG
- Normal: 5-15 mm Hg (young adult); upper limit = (Age + 10) / 4
- Normal A-a gradient + hypoxemia = hypoventilation or reduced PiO2 (lung is healthy)
- Widened A-a gradient + hypoxemia = V/Q mismatch, shunt, or diffusion defect (lung is diseased)
- Failure to correct with 100% O2 is pathognomonic of right-to-left shunt
- V/Q mismatch is the most common cause of widened A-a gradient in clinical practice
- In pure hypoventilation, PaCO2 is always elevated
- Hepatopulmonary syndrome widens the A-a gradient via intrapulmonary vasodilation (diffusion-perfusion impairment)
Sources: Medical Physiology (Boron & Boulpaep); Costanzo Physiology 7th Ed.; Frameworks for Internal Medicine; Goldman-Cecil Medicine; Comprehensive Clinical Nephrology 7th Ed.; Fishman's Pulmonary Diseases and Disorders; Harrison's Principles of Internal Medicine 22E