Normocytic normochromic anemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"normocytic anemia" AND classification
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to write a thorough answer. Let me compile everything.
Normocytic Normochromic Anemia
Normocytic normochromic anemia is defined by a normal mean corpuscular volume (MCV: 80-100 fL) and a normal mean corpuscular hemoglobin concentration (MCHC), meaning the red cells are normal in size and color but reduced in number. It is one of the most common and heterogeneous categories of anemia.
Definition and Key Diagnostic Parameters
| Parameter | Normal Range |
|---|---|
| MCV | 80-100 fL |
| MCHC | 32-36 g/dL |
| Hemoglobin | <12 g/dL (women), <13 g/dL (men) |
The Central Diagnostic Step: Reticulocyte Count
The reticulocyte count is the most important first step after identifying normocytic normochromic anemia. It divides all causes into two broad pathophysiologic groups:
1. Hypoproliferative (Low Reticulocyte Count)
The bone marrow is failing to respond appropriately - either due to inadequate stimulation or intrinsic marrow failure.
2. Hyperproliferative (High Reticulocyte Count)
The marrow is responding appropriately to peripheral red cell loss - indicates hemolysis or acute blood loss.
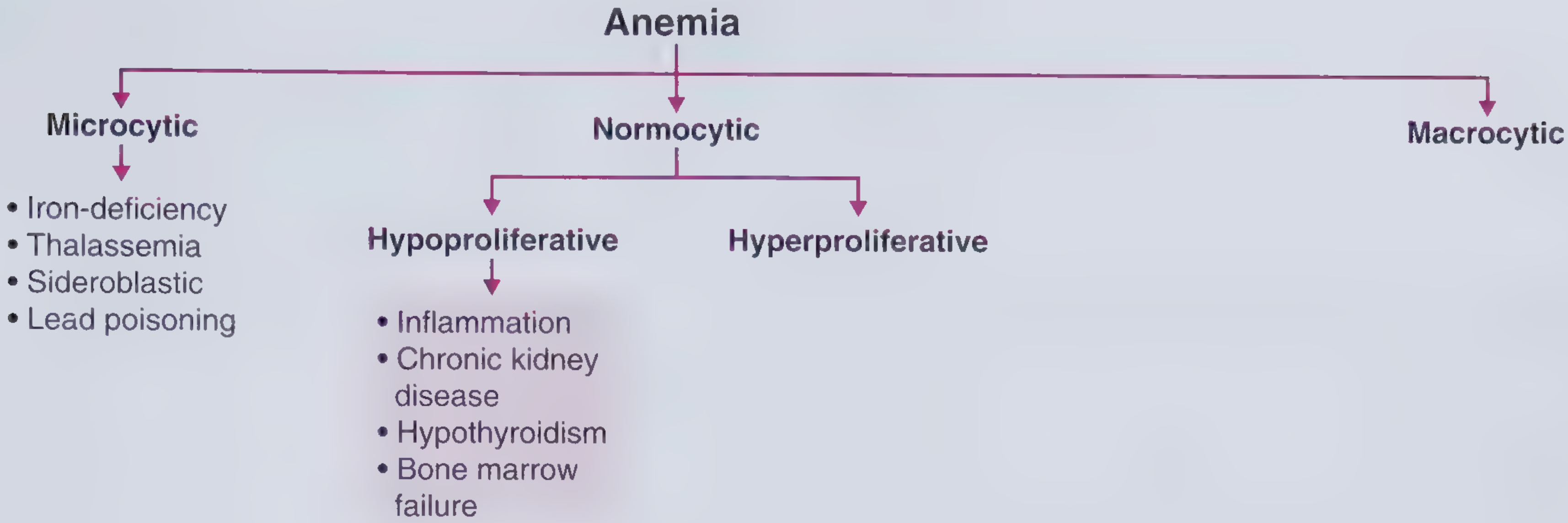
Classification of Causes
A. Hypoproliferative Normocytic Anemias
1. Anemia of Inflammation (Anemia of Chronic Disease)
- Formerly called "anemia of chronic disease (ACD)" - "anemia of inflammation" (AI) is now the preferred term
- Most common cause of anemia in hospitalized patients and the most common normocytic anemia syndrome after acute blood loss or early iron deficiency
- Mechanism: Chronic systemic inflammation elevates hepcidin (via IL-6) - this traps iron in macrophages, reduces iron availability for erythropoiesis, suppresses EPO secretion, and reduces RBC sensitivity to EPO
- Associated conditions: rheumatoid arthritis, collagen vascular diseases, chronic infections (osteomyelitis, bronchiectasis), malignancy
- Usually mild to moderate severity
- Lab findings:
- Serum iron: low
- TIBC: normal to decreased
- Transferrin saturation: >15% (distinguishes from IDA)
- Ferritin: normal to elevated (key distinguishing feature from IDA)
- Soluble transferrin receptor (sTfR): normal
AI vs. Iron Deficiency Anemia (IDA) - Key Comparison:
| Parameter | IDA | AI |
|---|---|---|
| Serum iron | ↓ | Normal to ↓ |
| TIBC | ↑ | Normal to ↑ |
| Transferrin saturation | <10% | >15% |
| Ferritin | ↓ | Normal to ↑ |
| sTfR | ↑ | Normal |
(Quick Compendium of Clinical Pathology, 5th ed., Table 14.13)
2. Anemia of Chronic Kidney Disease (CKD)
- Primarily due to EPO deficiency (reduced production by juxtaglomerular cells)
- Typically normochromic, normocytic
- Severity proportional to degree of kidney disease
- Treatment: erythropoiesis-stimulating agents (ESAs), e.g., darbepoetin - target Hgb 10-11.5 g/dL (higher targets >13 g/dL are associated with adverse cardiovascular outcomes)
3. Hypothyroidism
- Thyroid hormone regulates basal metabolic rate and O2 demand; hypothyroidism reduces EPO stimulus
- Usually mild normocytic anemia (sometimes macrocytic)
- Clues: weight gain, constipation, dry skin, depression, bradycardia
4. Bone Marrow Failure States
- Aplastic anemia: pancytopenia from destruction/suppression of hematopoietic stem cells; may present as normocytic or macrocytic anemia
- Pure red cell aplasia (PRCA): selective absence of erythroid precursors; associated with thymoma, parvovirus B19, and certain medications
- Myelodysplastic syndrome (MDS): clonal disorder; typically macrocytic but can be normocytic
- Marrow infiltration / myelophthisis: replacement by tumor, fibrosis, or granulomas - produces leukoerythroblastic picture
5. Endocrine Deficiencies
- Adrenal insufficiency, androgen deficiency, hypopituitarism
- Androgens normally stimulate EPO and erythropoiesis
6. Early Iron Deficiency
- Before iron stores are fully depleted and microcytosis develops, the MCV is still normal - the anemia is normocytic in its early/transitional phase
7. Anemia of Aging ("Unexplained Anemia of the Elderly")
- A cytokine/hepcidin-driven analog of AI
- Common in elderly individuals; specific treatment is generally not required unless another cause is found
8. Physiologic Anemia of Pregnancy
- Due to plasma volume expansion exceeding RBC mass increase (hemodilution)
B. Hyperproliferative Normocytic Anemias
1. Hemolytic Anemias
The peripheral blood smear is key here - polychromasia and macrocytosis reflect reticulocytosis. Causes include:
| Category | Examples |
|---|---|
| Membrane defects | Hereditary spherocytosis, elliptocytosis |
| Enzyme defects | G6PD deficiency, PK deficiency |
| Hemoglobinopathies | Sickle cell disease (HbSS), HbC disease |
| Immune | Autoimmune hemolytic anemia (AIHA), transfusion reactions |
| Microangiopathic (MAHA) | TTP, HUS, DIC, malignant hypertension |
| Infections | Malaria, Clostridium, Babesia |
| Hypersplenism | Splenic sequestration |
Lab markers of hemolysis:
- LDH: elevated (released from lysed RBCs)
- Indirect bilirubin: elevated (from heme catabolism)
- Haptoglobin: decreased (binds free Hb, gets consumed)
- Direct antiglobulin test (DAT/Coombs): positive in immune hemolysis
- Reticulocytes: elevated
- Peripheral smear: polychromasia, spherocytes, schistocytes (fragmented cells in MAHA), etc.
2. Acute Blood Loss
- Immediately after acute hemorrhage, red cells appear normal in size and color (normocytic, normochromic) because the remaining cells are unaffected
- Reticulocytosis develops within 3-5 days, peaking at 10-15% by day 7
- As reticulocytes (which are larger) increase, MCV may rise transiently
Blood Smear Findings in Normocytic Normochromic Anemia
The peripheral smear is "only occasionally useful" in normocytic normochromic anemia compared to microcytic or macrocytic anemias - Goldman-Cecil Medicine notes that "signs of inflammation may be present" but the smear is nonspecific. However, certain findings do guide diagnosis:
| Smear finding | Suggests |
|---|---|
| Rouleaux | Elevated plasma proteins, paraprotein (myeloma, Waldenström) |
| Red cell agglutination | Cold agglutinin disease, Mycoplasma infection |
| Polychromasia | Reticulocytosis - hemolysis or acute blood loss |
| Spherocytes | Hereditary spherocytosis, AIHA |
| Schistocytes | Microangiopathic hemolytic anemia |
| Nucleated RBCs + immature WBCs | Leukoerythroblastic reaction (marrow infiltration) |
| HbC crystals | Hemoglobin C disease/compound heterozygote |
Diagnostic Approach
Normocytic Normochromic Anemia (MCV 80-100 fL)
|
↓
Reticulocyte Count
/ \
LOW (hypoproliferative) HIGH (hyperproliferative)
| |
Consider: Hemolysis workup:
• Anemia of inflammation LDH, haptoglobin,
• Anemia of CKD indirect bili, DAT
• Hypothyroidism Peripheral smear
• Bone marrow failure OR
• Endocrine deficiency Acute blood loss
• Early iron deficiency
|
Check ferritin, iron studies, creatinine,
TSH, EPO level, +/- bone marrow biopsy
Important Associations
- HIV/AIDS: Normocytic normochromic anemia is a well-recognized complication
- Amphotericin B therapy: Causes gradual normocytic normochromic anemia (hematocrit rarely falls below 20-25% unless compounded by other causes)
- Waldenström macroglobulinemia: Moderate to severe normocytic normochromic anemia with very high IgM levels
- Hereditary enzyme deficiencies (e.g., PK deficiency): Normocytic normochromic hemolytic anemia with absent morphologic abnormalities on smear - diagnosed by specific enzyme assay
Sources
- Goldman-Cecil Medicine, 2-Volume Set - Normocytic Normochromic Anemia section and Table 144-9 (Classification by MCV)
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Hyperproliferative Normocytic Anemias
- Quick Compendium of Clinical Pathology, 5th ed. - Anemia of Inflammation, Table 14.13
- Frameworks for Internal Medicine - Normocytic Hypoproliferative Anemia
- Symptom to Diagnosis: An Evidence-Based Guide, 4th ed. - Differential Diagnosis of Normocytic Anemia
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Acute Blood Loss
This is a shared conversation. Sign in to Orris to start your own chat.