Eye signs in hyperthyroidism
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I have comprehensive textbook content and clinical images. Here is the full detailed answer:
Eye Signs in Hyperthyroidism (Thyroid Eye Disease / Graves Ophthalmopathy)
Eye signs in hyperthyroidism fall into two broad categories: (1) sympathetic overactivity signs - seen in any cause of hyperthyroidism, and (2) infiltrative/autoimmune signs - specific to Graves disease (Graves Ophthalmopathy, GO).
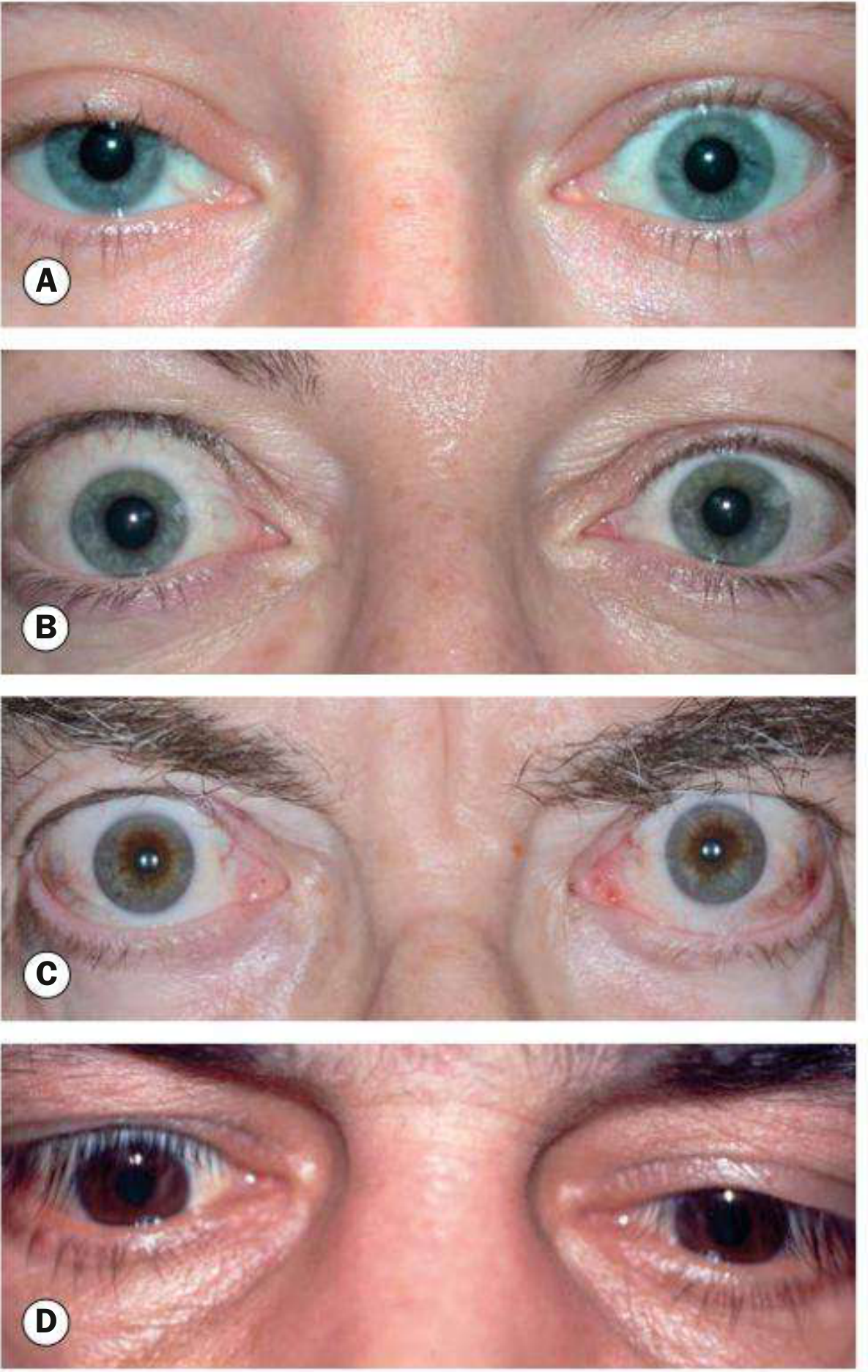
Lid Signs
These are the most classic and frequently tested signs.
| Sign | Description | Mechanism |
|---|---|---|
| Dalrymple's sign | Lid retraction in primary gaze - widened palpebral opening, sclera visible above the limbus | Sympathetic overactivity of Müller's muscle (smooth muscle part of levator palpebrae) |
| Von Graefe's sign | Retarded descent of the upper lid on downgaze (lid lag) - the upper lid cannot keep pace with the eyeball as it follows a downward-moving target | Lagging of the overactive levator muscle |
| Kocher's sign | Staring, frightened appearance with marked lid retraction, especially on attentive fixation | Exaggerated Dalrymple's + sympathetic overactivity |
| Stellwag's sign | Staring look + infrequent blinking + widening of palpebral fissure | Toxic contraction of striated fibres of levator palpebrae superioris |
| Joffroy's sign | Absence of forehead wrinkling when the patient looks upward with the face tilted downward | Failure of frontalis to compensate |
| Moebius' sign | Inability or failure to converge the eyeballs | Weakness of medial recti / convergence insufficiency |
Key distinction: Lid retraction and lid lag are not the same as exophthalmos. In lid retraction, the upper eyelid is higher than normal but the eyeball is not displaced forward. In exophthalmos, the eyeball itself is pushed forward. - S Das Manual on Clinical Surgery, p. 387-388
Exophthalmos / Proptosis
Exophthalmos (proptosis) is the forward displacement of the eyeball due to increased volume in the retro-orbital space from glycosaminoglycan deposition, enlargement of extraocular muscles, and expansion of orbital fat. It is the leading cause of proptosis in adults.
- Can be unilateral or bilateral (and is often asymmetric)
- When severe, leads to lagophthalmos (inability to fully close the eye)
- Complications: exposure keratopathy, corneal ulceration, bacterial keratitis
The sclera below the lower limbus becomes visible first, followed by sclera above the upper limbus with increasing severity.
Soft Tissue Signs
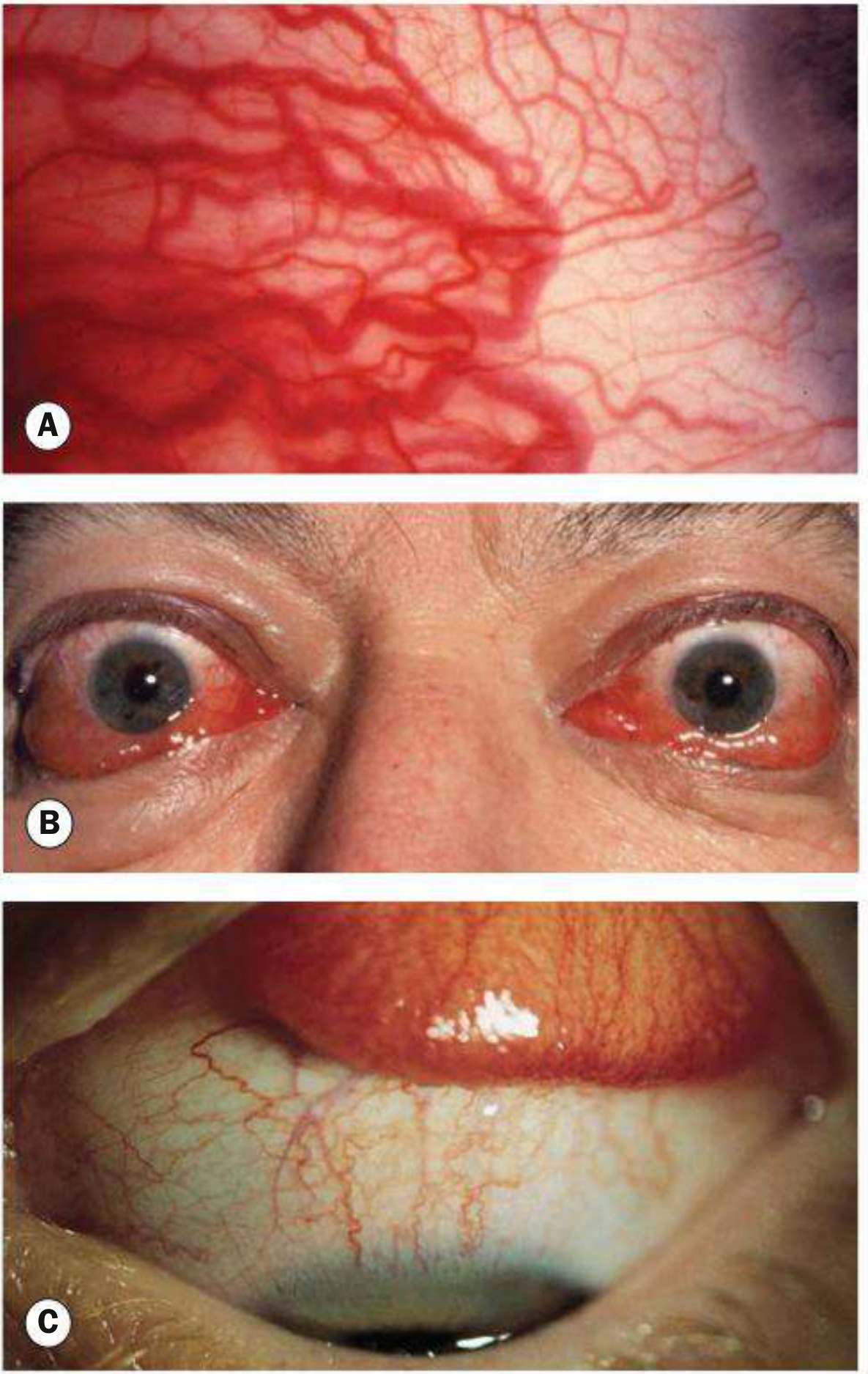
- Periorbital and eyelid oedema
- Conjunctival injection (Goldzeiher's sign - conjunctival redness)
- Chemosis - oedema of the conjunctiva (becomes thickened, crinkled) due to obstruction of venous and lymphatic drainage by raised retro-orbital pressure
- Tearing, photophobia, orbital discomfort
- Superior limbic keratoconjunctivitis
Restrictive Myopathy (Ophthalmoplegia)
30-50% of patients with thyroid eye disease develop ophthalmoplegia. The muscles are affected by inflammatory oedema then fibrosis. Importantly, the fibrosis spares the tendinous insertions - causing a "tight" rather than "weak" muscle restriction.
Muscle involvement frequency (mnemonic: "I'M SO"):
- I - Inferior rectus (most common) → defective elevation (mimics superior rectus palsy)
- M - Medial rectus → defective abduction (mimics 6th nerve palsy)
- S - Superior rectus → defective depression
- O - Oblique muscles
- Lateral rectus is rarely involved; an exotropia in thyroid disease should raise suspicion of concurrent myasthenia gravis
Diplopia is typically worse in the morning and improves as the day progresses.
Optic Neuropathy (Most Serious Complication)
Compressive optic neuropathy occurs in ~6% of cases. Enlarged, congested recti compress the optic nerve at the orbital apex.
- Critical point: Optic nerve compression can occur with little or no proptosis
- Presents with reduced visual acuity, colour desaturation, afferent pupillary defect
- Patients should be advised to self-monitor by alternately occluding each eye and checking colour perception
Summary Table (All Named Signs)
| Sign | What you see |
|---|---|
| Dalrymple's | Lid retraction in primary gaze (widened fissure, scleral show above iris) |
| Von Graefe's | Lid lag on downgaze |
| Kocher's | Staring, frightened look on attentive fixation |
| Stellwag's | Stare + infrequent blinking |
| Joffroy's | No forehead wrinkling on upward gaze with face down |
| Moebius' | Failure of convergence |
| Goldzeiher's | Conjunctival injection (redness) |
Important Notes
- Lid retraction is the single most common clinical feature of Graves ophthalmopathy - Localization in Clinical Neurology, 8e, p. 428
- Sympathetic signs (Dalrymple's, Von Graefe's, Stellwag's, Joffroy's, Moebius') can occur in any cause of thyrotoxicosis
- Infiltrative signs (proptosis, restrictive myopathy, optic neuropathy, chemosis) are specific to Graves disease
- Ophthalmopathy may appear before, during, or after thyroid disease and can even occur in the absence of thyroid dysfunction
- Radioiodine therapy may worsen ophthalmopathy
Sources: Kanski's Clinical Ophthalmology 10e; S Das Manual on Clinical Surgery 13e; Localization in Clinical Neurology 8e; Cummings Otolaryngology; Bradley & Daroff's Neurology; Adams & Victor's Neurology
Mechanism of proptosis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive mechanistic content from multiple authoritative textbooks. Here is the complete answer:
Mechanism of Proptosis in Hyperthyroidism (Graves Ophthalmopathy)
Proptosis in hyperthyroidism is almost exclusively a feature of Graves disease (not seen in other causes of hyperthyroidism), and results from autoimmune-mediated expansion of the orbital contents within the fixed bony orbit.
The Core Problem: Fixed Space, Expanding Contents
The orbit is a rigid bony box. When its contents expand, the only direction the eyeball can go is forward - producing proptosis. The expansion has two components:
- Enlarged extraocular muscles (dominant contributor)
- Increased orbital fat volume
Step-by-Step Mechanism
Step 1 - Loss of Immune Tolerance
Graves disease results from a loss of immune tolerance to thyroid antigens. Autoreactive T lymphocytes are sensitised to antigens that are shared by both the thyroid gland and the orbital tissues - the TSH receptor (TSH-R) being the key shared antigen, expressed in both locations.
Step 2 - T Cell Infiltration of the Orbit
Autoreactive T lymphocytes migrate into the retrobulbar space and infiltrate the extraocular muscles and orbital fat. This triggers local release of inflammatory cytokines, particularly:
- Interferon-γ (IFN-γ)
- Tumour necrosis factor (TNF)
- Interleukin-1 (IL-1)
Step 3 - Orbital Fibroblast Activation (Key Step)
The cytokines activate retrobulbar fibroblasts, which then:
- Secrete large amounts of glycosaminoglycans (GAGs) - particularly hyaluronic acid - and deposit collagen fibrils in the extraocular muscles and orbital fat
- These GAGs are extremely hydrophilic and can bind many times their weight in water
- This causes massive water retention, oedema, and swelling of the extraocular muscles
"Retrobulbar fibroblasts secrete glycosaminoglycans, causing engorgement of the extraocular muscles and orbital fat and increasing the volume of the orbital contents." - Cummings Otolaryngology, p. 2429
Step 4 - IGF-1R Pathway (Additional Mechanism)
Aberrant signalling via insulin-like growth factor 1 receptors (IGF-1R) on orbital fibroblasts has also been implicated. TSH-R and IGF-1R form complexes on fibroblasts, further amplifying fibroblast activation and GAG synthesis.
Step 5 - Orbital Volume Expansion
The net result:
- Extraocular muscles become massively engorged and swollen
- Orbital fat volume increases
- Intra-orbital pressure rises
- The eyeball is displaced forward = proptosis
Step 6 - Late-Stage Fibrosis
As the disease becomes inactive, atrophy and irreversible muscle fibrosis dominate the histological picture. This is the basis of the restrictive myopathy (diplopia) seen in chronic disease.
Diagram of Mechanism
TSH-R autoantibodies (TRAb/TSI)
↓
Autoreactive T cells sensitised to TSH-R
(shared antigen: thyroid + orbital tissues)
↓
T cell infiltration of orbit + cytokine release
(IFN-γ, TNF, IL-1) + IGF-1R co-signalling
↓
Orbital fibroblast activation
↓
↑ Glycosaminoglycan synthesis (hyaluronic acid)
+ collagen deposition in extraocular muscles & fat
↓
GAGs bind water → oedema + muscle swelling
+ Increased orbital fat volume
↓
↑ Intra-orbital pressure in rigid bony orbit
↓
Eyeball displaced forward = PROPTOSIS
↓ (late)
Irreversible fibrosis → restrictive myopathy
Consequences of Raised Intra-orbital Pressure
| Consequence | Mechanism |
|---|---|
| Proptosis | Eyeball pushed forward |
| Diplopia | Restricted EOM movement (tight fibrosed muscles) |
| Optic neuropathy | Compression of optic nerve at orbital apex by enlarged EOMs |
| Exposure keratopathy | Lagophthalmos from severe proptosis |
| Conjunctival chemosis | Obstruction of venous/lymphatic drainage |
Important: Optic nerve compression can occur in the absence of significant proptosis - the apex of the orbit is where the muscles are most crowded and compression of the optic nerve can occur even when forward displacement is minimal. - Kanski's Clinical Ophthalmology, p. 135
Therapeutic Relevance
Understanding the mechanism directly explains the treatments:
- Corticosteroids / IV methylprednisolone - suppress the inflammatory cytokine phase
- Orbital radiation - targets infiltrating lymphocytes
- Teprotumumab (monoclonal antibody) - blocks TSH-R/IGF-1R complexes on orbital fibroblasts, directly targeting the fibroblast activation step; reduces proptosis significantly
- Orbital decompression surgery - physically enlarges the bony orbit to reduce pressure
- Smoking cessation - smoking upregulates inflammatory cytokines and increases orbital venous congestion, worsening disease by 7-8 fold
Sources: Harrison's Principles of Internal Medicine 22e (2025); Cummings Otolaryngology Head & Neck Surgery; Schwartz's Principles of Surgery 11e; Kanski's Clinical Ophthalmology 10e
Approach to paraparesis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have excellent textbook content. Let me compile the full structured approach to paraparesis:
Approach to Paraparesis
Paraparesis = weakness of both lower limbs (incomplete). Paraplegia = complete paralysis of both lower limbs. The approach follows a systematic sequence: define the type, localise the lesion, narrow the differential, then investigate.
Step 1 - Define the Pattern of Weakness
Before anything else, determine: Is this UMN or LMN paraparesis?
| Feature | UMN (Spastic) | LMN (Flaccid) |
|---|---|---|
| Tone | Increased (spasticity) | Decreased / flaccid |
| Power | Reduced | Reduced |
| Reflexes (DTR) | Exaggerated (hyperreflexia) | Diminished / absent |
| Plantar response | Extensor (Babinski +ve) | Flexor or absent |
| Clonus | Present | Absent |
| Wasting | Late / mild | Early / prominent |
| Fasciculations | Absent | Present (if LMN cell body affected) |
| Bladder | Spastic (urgency, frequency) | Flaccid (retention, overflow) |
Note: In acute spinal cord injury ("spinal shock"), a UMN lesion presents initially as a flaccid areflexic paraplegia before spasticity develops over days-weeks.
Step 2 - Localise the Lesion
A. Is the lesion in the SPINAL CORD (most common) or elsewhere?
Other sites causing paraparesis:
- Bilateral cerebral/parasagittal lesions (e.g., meningioma compressing both motor strips, bilateral anterior cerebral artery infarcts) - rare, but brain imaging will show it
- Peripheral - bilateral peripheral neuropathy, Guillain-Barré syndrome (ascending flaccid paralysis)
- Neuromuscular junction - rare
- Muscle - myopathy (proximal weakness, no sensory loss)
Clue: The presence of a sensory level on the trunk almost always means a spinal cord lesion.
B. If spinal cord - what level?
Determine the segmental level by:
| Finding | Localisation |
|---|---|
| Weakness of arms + legs (quadriparesis), diaphragm spared | Cervical cord (C3-C8) |
| Weakness of legs only, arms normal | Thoracic cord (T1-T12) |
| Weakness of legs + saddle anaesthesia | Conus medullaris (L1-S2) |
| Asymmetric flaccid areflexic leg weakness, no clear sensory level | Cauda equina (below L1) |
Key rules for level determination:
- The sensory level (highest dermatomal level of impaired sensation on trunk) identifies the approximate cord level - but the actual lesion is typically a few segments above the sensory level
- Root pain / radicular pain and focal back tenderness are the most reliable guides to the exact vertebral level
- The motor deficit level is less reliable than the pain/sensory level
C. If spinal cord - is the lesion Extradural, Intradural-Extramedullary, or Intramedullary?
This is the most clinically important localisation step:
| Feature | Extradural | Intradural Extramedullary | Intramedullary |
|---|---|---|---|
| Pain | Local back pain, bilateral root pain, percussion tenderness | Unilateral radicular pain (early), contralateral tract signs | Central aching, less radicular |
| Motor vs sensory | Motor symptoms precede sensory | Motor and sensory involvement together | Sensory often early; dissociated sensory loss (pain/temp lost, touch preserved) |
| Brown-Séquard | Possible | Classic presentation (ipsilateral motor + proprioception loss; contralateral pain/temp loss) | Rare/partial |
| Sphincters | Late involvement | Moderate | Early involvement |
| Progression | Rapid (days-weeks) in metastases | Gradual (months) | Variable |
| Examples | Metastases, disc prolapse, TB (Pott's), abscess, haematoma | Meningioma, neurofibroma, arachnoiditis | Glioma, ependymoma, syringomyelia, MS, AVM, transverse myelitis |
"The findings of segmental amyotrophy and sensory loss of dissociated type (loss of pain and temperature with preservation of tactile sensation) point to an intramedullary lesion." - Adams & Victor's Neurology, p. 1278
"If root pain developed early and is bilateral, pain and aching in the spine are prominent, percussion tenderness is marked, and motor symptoms below the lesion preceded sensory ones, and sphincter disturbances were late - suspect extradural lesion." - Adams & Victor's Neurology, p. 1278
Step 3 - Differential Diagnosis by Mode of Onset
Acute Paraparesis (hours to days)
| Cause | Key Clue |
|---|---|
| Spinal cord trauma | History of injury, vertebral fracture on imaging |
| Epidural haematoma | Anticoagulants, post-procedure, sudden back pain |
| Epidural abscess | Fever, back pain, immunocompromised, IV drug use |
| Transverse myelitis | Post-infectious, preceded by fever/viral illness; rapid progression |
| Anterior spinal artery infarction | Sudden onset, aortic surgery, pain at onset; dissociated sensory loss (pain/temp affected, dorsal columns spared) |
| Spinal cord haemorrhage (haematomyelia) | Sudden severe pain, anticoagulation |
| Acute disc prolapse with cord compression | Known back disease, trauma |
| Guillain-Barré syndrome | Ascending flaccid areflexic, post-infectious, albuminocytological dissociation in CSF |
Subacute Paraparesis (days to weeks)
| Cause | Key Clue |
|---|---|
| Metastatic spinal cord compression | Known malignancy, back pain preceding weakness |
| Tuberculous (Pott's) spondylitis | Endemic area, constitutional symptoms, gibbus deformity |
| Multiple sclerosis | Relapsing-remitting, young adult, other demyelinating episodes |
| Neuromyelitis optica (NMO) | Severe myelitis + optic neuritis, anti-AQP4 antibodies |
| Pyogenic osteomyelitis/discitis | Fever, elevated CRP/ESR |
Chronic/Progressive Paraparesis (months to years)
| Cause | Key Clue |
|---|---|
| Cervical/thoracic spondylotic myelopathy | Older patient, neck/back pain, most common cause overall |
| Spinal cord tumour (meningioma, glioma, ependymoma) | Slow progressive, no fever |
| Subacute combined degeneration (Vit B12 deficiency) | Posterior + lateral column signs, macrocytic anaemia, peripheral neuropathy |
| Hereditary spastic paraplegia (HSP) | Positive family history, pure spastic paraparesis from childhood |
| Tropical spastic paraparesis (HTLV-1 myelopathy) | Endemic area, insidious onset |
| Syringomyelia | Dissociated sensory loss (cape distribution), wasting of hands |
| Motor neuron disease (PLS) | Pure UMN syndrome, no sensory loss, gradual |
| Hypocupremia | Spine + peripheral neuropathy, similar picture to B12 deficiency |
| Spinal AVM / dural arteriovenous fistula | Middle-aged male, progressive myelopathy, worse with exercise |
| Friedreich's ataxia | Young, cerebellar signs, pes cavus, cardiomyopathy |
Step 4 - Important Clinical Syndromes
Brown-Séquard Syndrome (hemisection of cord)
- Ipsilateral: UMN weakness + loss of proprioception/vibration (dorsal column)
- Contralateral: loss of pain and temperature (spinothalamic tract - crosses at entry level)
- Causes: trauma, MS, tumour, disc herniation
Conus Medullaris Syndrome
- Mixed UMN + LMN features (both cord and nerve root involved)
- Early bladder/bowel dysfunction (urinary retention, constipation)
- Saddle anaesthesia (S3-S5)
- Loss of bulbocavernosus and anal reflexes
- Impotence
Cauda Equina Syndrome
- Pure LMN - flaccid, areflexic, wasting
- Asymmetric weakness (roots compressed differentially)
- Saddle anaesthesia
- Bladder: flaccid retention with overflow incontinence
- Causes: central disc prolapse (L4/5, L5/S1), tumours, trauma - surgical emergency
Step 5 - Investigations
Urgent (if acute)
- MRI whole spine (with contrast) - investigation of choice; shows cord, lesion, level
- CT spine if MRI unavailable (good for bone/fractures)
- Bloods: FBC, CRP/ESR, coagulation, cultures if infective cause suspected
Routine workup
- MRI brain (if bilateral cerebral cause suspected, or to look for MS plaques)
- CSF analysis: protein (elevated in cord compression - Froin's syndrome in complete block), cells (inflammatory/infective), oligoclonal bands (MS), cytology (malignancy)
- Nerve conduction studies + EMG: differentiate cord from peripheral nerve/root cause
- Evoked potentials: SEPs (sensory) and MEPs (motor) - assess cord conduction
- Bloods: vitamin B12, folate, copper, HTLV-1 antibodies, ANA/ANCA, AQP4-IgG (NMO), HIV
- Bone scan / CT chest-abdomen-pelvis: if metastatic disease suspected
Step 6 - Flowchart Summary
PARAPARESIS
|
├── ACUTE onset (< 24h) → Emergency: trauma, infarct, haematoma, abscess
├── SUBACUTE (days-weeks) → Myelitis, metastases, TB, MS, NMO
└── CHRONIC (months-years) → Spondylosis, tumour, B12 def, HSP, HTLV-1
↓
UMN pattern (spastic) vs LMN pattern (flaccid)
↓
Sensory level? → Yes → Spinal cord lesion
↓
Determine vertebral level (sensory level, root pain, percussion)
↓
Extradural vs Extramedullary-Intradural vs Intramedullary
↓
MRI spine (with contrast) → Definitive anatomical localisation
Sources: Adams & Victor's Principles of Neurology 12e; Bradley & Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.