Acne vulgaris
Reading File
Finding Sources
Searching PubMed
"acne vulgaris"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Acne Vulgaris

Acne vulgaris with inflammatory papules, pustules, and comedones. (Harrison's Principles of Internal Medicine 22E, Fig. 60-1)
Definition & Overview
Acne vulgaris is a chronic inflammatory disease of the pilosebaceous unit, clinically characterized by comedones, papules, pustules, nodules, and often scars. It affects approximately 40-50 million individuals annually in the United States alone, accounting for ~0.3% of the total global disease burden and ~15% of the dermatologic disease burden. It has an undeniable psychosocial impact - affected individuals have increased rates of social isolation, anxiety, depression, and suicidal ideation.
- Dermatology 2-Volume Set 5e, p. 2252
- Andrews' Diseases of the Skin, p. 280
Epidemiology
-
Affects ~85% of young people between ages 12-24 years
-
Peak incidence at ages 15-18 in both genders
-
Males tend to have more severe nodulocystic disease
-
Persists into adulthood in 35% of women and 20% of men in their 30s
-
About 12% of women and 3% of men continue to have clinical acne until age 44
-
Preadolescent acne (ages 7-11) is becoming more common with earlier puberty onset
-
Risk groups: XYY karyotype, polycystic ovarian syndrome (PCOS), hyperandrogenism, hypercortisolism, precocious puberty
-
Dermatology 2-Volume Set 5e, p. 2262-2263
Pathogenesis
Four key factors contribute (Robbins & Cotran):
- Follicular hyperkeratinization - Keratinization of the lower follicular infundibulum forms a keratin plug that blocks sebum outflow
- Sebaceous gland hypertrophy - Driven by androgens at puberty; castrated males historically did not develop acne
- Cutibacterium acnes (formerly Propionibacterium acnes) - Lipase-synthesizing bacteria colonize the hair follicle, converting sebum lipids into proinflammatory free fatty acids; also activates toll-like receptors and triggers cytokine release
- Inflammation - Rupture of the comedone wall releases oily/keratinous debris, triggering a foreign-body inflammatory reaction
Androgens are permissive: sebum production rises with puberty, and sebum quantity/quality is a central driver. Genetic factors influence the number, size, and activity of sebaceous glands.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 134
- Harrison's Principles of Internal Medicine 22E, p. 434
Clinical Features
Lesion Types
| Lesion | Description |
|---|---|
| Closed comedo (whitehead) | 1-2 mm pebbly white papule; keratin plug trapped beneath epidermis; potential source of rupture and inflammation |
| Open comedo (blackhead) | Dilated follicular orifice with oxidized, darkened oily debris; color is oxidized melanin, NOT dirt; rarely causes inflammatory acne |
| Papule | 1-5 mm inflammatory erythematous lesion |
| Pustule | As above but with visible pus |
| Nodule/cyst | Larger deep inflammatory lesion; may coalesce into fluctuant plaques with sinus tracts; major scarring risk |
Distribution
- Face: cheeks (most common), nose, forehead, chin; ears (comedones in concha, cysts in lobes)
- Neck: especially nuchal area - large cystic lesions
- Upper trunk and upper arms (chest and back common)
Temporal Pattern
- Comedonal acne starts first (forehead and cheeks at ages 8-12)
- More severe inflammatory disease develops in mid-teens
- Women: papulopustular flares ~1 week premenstrually
- Adult female acne (20-35 years): papules, pustules, and deep painful nodules on jawline, chin, and upper neck
Sequelae
-
Post-inflammatory erythema (reddish-purple macules) - short-lived in light skin
-
Post-inflammatory hyperpigmentation (PIH) - in dark skin, may persist months
-
Scar types: ice pick scars (temples/cheeks), canyon-type atrophic scars (face), hypertrophic/keloidal scars (neck/trunk), anetoderma-type scars (trunk)
-
Andrews' Diseases of the Skin, p. 280-281
-
Harrison's Principles of Internal Medicine 22E, p. 433-434
Exacerbating Factors
-
Friction/trauma (headbands, chin straps, athletic helmets)
-
Comedogenic cosmetics or hair preparations
-
Industrial chemical exposure (cutting oils, chlorinated hydrocarbons, coal tars)
-
Drugs: glucocorticoids (topical or systemic), progestin-only contraception, lithium, isoniazid, androgens, EGFR inhibitors, anabolic steroids
-
High-glycemic diet (evidence is moderate but relevant)
-
Large quantities of skim milk (the skim milk - insulin-IGF-1 hypothesis)
-
Obesity / insulin resistance / metabolic syndrome
-
Harrison's Principles of Internal Medicine 22E, p. 434
-
Andrews' Diseases of the Skin, p. 282
Classification (Severity)
| Severity | Features |
|---|---|
| Mild | Mostly comedones ± few papules/pustules |
| Moderate | More numerous papules and pustules, possibly some nodules |
- Severe | Nodules, cysts, confluent lesions; significant scarring risk |
Treatment
All topical treatments are preventive - 8-12 weeks of treatment is required to judge efficacy. The entire acne-prone area (not just individual lesions) should be treated.
Topical Agents
| Agent | Mechanism | Notes |
|---|---|---|
| Retinoids (tretinoin, adapalene, tazarotene) | Normalize follicular desquamation; comedolytic; anti-inflammatory; enhance penetration of other agents | Preferred for maintenance therapy; tretinoin apply at night; 8-12 weeks for response |
| Benzoyl peroxide (BPO) | Bactericidal against C. acnes; no resistance | Should be combined with topical antibiotics to prevent resistance |
| Clindamycin / Erythromycin | Anti-C. acnes + anti-inflammatory | Always combine with BPO to prevent resistance; never use topical antibiotic alone long-term |
| Azelaic acid | Antimicrobial + anti-inflammatory + comedolytic; reduces PIH | Good option in PIH-prone skin |
| Dapsone gel | Anti-inflammatory | FDA approved; particularly useful in adult women |
| Salicylic acid | Keratolytic; comedolytic | OTC option |
| Clascoterone cream | Topical androgen receptor antagonist | FDA approved; novel mechanism |
Oral Systemic Agents
Antibiotics (for moderate-to-severe inflammatory acne):
- Doxycycline: 100 mg BID or extended-release preparations; first-line; also has anti-inflammatory properties independent of antibacterial effect
- Minocycline: 50-100 mg once or twice daily; less affected by food; watch for vestibular side effects (vertigo), pigmentation (skin/mucosa/scars), and rare lupus-like syndromes
- Sub-antimicrobial doxycycline (20 mg BID or 40 mg SR daily): anti-inflammatory dose only; no resistance risk
- Amoxicillin: for those intolerant to tetracyclines, or during pregnancy (category B)
- Adequate response expected at 3 months; limit duration to prevent resistance
Antibiotic resistance is a real concern: always combine with BPO, avoid dissimilar oral + topical antibiotics simultaneously, limit duration, encourage isotretinoin when clearance cannot be maintained without long-term antibiotics.
Hormonal therapy (females):
- Oral contraceptive pills (OCPs): several are FDA-approved for acne; target androgen-driven sebum production
- Spironolactone: safe, effective, and durable antiandrogen; particularly useful for adult female acne with jawline/chin distribution
Isotretinoin (13-cis-retinoic acid):
-
Reserved for severe nodulocystic acne unresponsive to other therapies
-
Mechanism: strong antisebaceous action; also reduces C. acnes colonization and inflammation
-
Dosing: weight-based, cumulative dose-driven duration
-
Side effects: dry skin, cheilitis (very common); rare severe extracutaneous effects
-
Highly teratogenic: regulated under iPLEDGE program in the US; requires two negative pregnancy tests before initiation and negative test before each refill
-
Results are excellent in appropriately selected patients
-
Harrison's Principles of Internal Medicine 22E, p. 434-435
-
Andrews' Diseases of the Skin, p. 282-284
Treatment by Severity (Andrews' Box 13.1 Summary)
| Severity | First-line Approach |
|---|---|
| Mild (comedonal) | Topical retinoid ± BPO or salicylic acid |
| Mild-moderate (papulopustular) | Topical retinoid + topical antibiotic + BPO |
| Moderate-severe (inflammatory) | Topical combination + oral doxycycline or minocycline |
| Severe (nodulocystic/scarring) | Oral isotretinoin; hormonal therapy in women |
Special Situations
Neonatal Acne (Neonatal Cephalic Pustulosis)
- Develops days after birth; male preponderance; transient facial papules/pustules
- Most clear spontaneously within days to weeks
- Persistent cases may need topical benzoyl peroxide
Adult Female Acne
- Distribution: jawline, chin, upper neck
- Deep, painful, persistent nodules
- Responds well to hormonal therapy (spironolactone, OCPs)
Acne with PCOS
- More severe, less responsive to standard therapy
- Dietary counseling (low-glycemic diet, reduce skim milk) important, especially with insulin resistance
Differential Diagnosis
Key conditions to distinguish from acne vulgaris:
-
Rosacea (no comedones; central facial erythema and telangiectasia)
-
Perioral/periorificial dermatitis
-
Folliculitis (staphylococcal, gram-negative, Malassezia, eosinophilic)
-
Drug-induced acneiform eruptions (steroids, EGFR inhibitors, lithium)
-
Keratosis pilaris (follicular plugging without inflammation)
-
Angiofibromas (as in tuberous sclerosis)
-
Syndromes: PAPA, PAPASH, SAPHO, Apert syndrome
-
Dermatology 2-Volume Set 5e, p. 2693-2720
Patient Education Points
- Overly vigorous scrubbing aggravates acne by mechanically rupturing comedones
- Avoid comedogenic cosmetics (use noncomedogenic, pressed powder preferred over oil-based)
- High-glycemic foods and large amounts of skim milk may worsen acne
- Treatment takes 8-12 weeks to show effect - adherence is the most common cause of treatment failure
- Apply topical treatments to the entire affected area, not just individual lesions
- Distinguish active inflammatory lesions from resolved PIH macules (the latter do not need active treatment)
Recent Evidence (2024-2026)
- A 2025 systematic review on acne and the cutaneous microbiome (PMID 39269130) highlights the role of the skin microbiome in pathogenesis and its implications for treatment selection - supporting the move toward microbiome-preserving strategies rather than broad antibiotic use.
- A 2025 meta-analysis (PMID 39509291) found that isotretinoin combined with laser/light-based treatments outperforms isotretinoin alone for acne vulgaris, supporting combination approaches in appropriate candidates.
- A 2024 network meta-analysis (PMID 39110247) compared microneedling combinations for acne scarring, confirming microneedling with PRP or radiofrequency as effective options for post-acne scarring management.
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), pp. 433-435
- Andrews' Diseases of the Skin - Clinical Dermatology, pp. 279-284
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 134
- Dermatology 2-Volume Set 5e, pp. 2252-2265, 2691-2742
One line for neet pg
Here are the high-yield one-liners for NEET PG:
- Most common cause of acne - Cutibacterium acnes (formerly Propionibacterium acnes)
- Primary lesion - Comedone
- Open comedone (blackhead) - Color due to oxidized melanin, NOT dirt
- Closed comedone (whitehead) - Precursor to inflammatory lesions
- Pathogenesis - Androgen → ↑ sebum → follicular plugging → C. acnes → free fatty acids → inflammation
- Drug of choice for severe nodulocystic acne - Isotretinoin (13-cis-retinoic acid)
- Isotretinoin MOA - Strong antisebaceous action (reduces sebum production)
- Most teratogenic anti-acne drug - Isotretinoin
- Topical antibiotic always combined with - Benzoyl peroxide (to prevent resistance)
- Topical androgen receptor antagonist - Clascoterone (FDA approved)
- Antiandrogen for adult female acne - Spironolactone
- Sub-antimicrobial doxycycline - 40 mg SR once daily; anti-inflammatory only, no resistance
- First-line topical maintenance - Retinoids (tretinoin, adapalene)
- Acne NOT seen in - Castrated males (androgens are permissive)
- Scarring type on face - Ice pick scars (temples/cheeks); keloidal scars on trunk/neck
- Adult female acne distribution - Jawline, chin, upper neck
- Drug causing acneiform eruption - Steroids, lithium, isoniazid, EGFR inhibitors
Find recent treatment protocols for severe acne scarring
Searching PubMed
"acne scars"[MeSH Terms] AND treatment
Finding Sources
Searching the Web
severe acne scarring treatment protocol guidelines 2024 2025
Searching PubMed
"acne scarring" AND (laser OR microneedling OR treatment)
Finding Sources
Reading Article
PMID: 38059974
Reading Article
PMID: 39630683
Reading Article
PMID: 38845186
Reading Article
PMID: 39110247
Reading Article
PMID: 35792196
Finding Sources
I now have comprehensive evidence to compile a thorough answer.
Recent Treatment Protocols for Severe Acne Scarring (2023-2025)
Scar Classification - Treatment Foundation
Before any protocol can be applied, scar subtype must be identified, as each responds differently to specific modalities:
| Scar Type | Morphology | Best Location | Preferred Treatment |
|---|---|---|---|
| Ice pick | Deep, narrow, V-shaped | Temples, cheeks | Punch excision, TCA CROSS |
| Boxcar | Broad, well-defined walls | Cheeks, temples | Ablative fractional laser, subcision |
| Rolling | Undulating surface, fibrous bands | Cheeks | Subcision, radiofrequency microneedling |
| Hypertrophic/Keloidal | Raised, firm | Neck, trunk, jawline | Intralesional steroids, PDL, silicone |
| PIH / Erythema | Flat, pigmented or red macules | Face | Chemical peels, IPL, topical agents |
Using validated assessment tools (ECCA grading, SCAR-S, Goodman-Baron scale) before and during treatment is now considered best practice for tracking outcomes.
- Jennings et al., J Am Acad Dermatol 2024 [PMID: 35792196]
Core Principle: Combination Therapy is Superior to Monotherapy
The 2023-2025 literature consistently shows that combined modality approaches outperform any single treatment across all scar types. No single "gold standard" exists, and treatment must be individualized.
1. Lasers and Energy-Based Devices
Ablative Fractional Lasers (AFL)
- CO2 (10,600 nm) and Er:YAG (2940 nm) - the most effective overall for atrophic scars
- AFL offers the greatest improvement but with more downtime (7-14 days), risk of post-inflammatory hyperpigmentation (PIH), and longer healing
- CO2 fractional laser is preferred for moderate-to-severe atrophic scarring on the face
- Er:YAG has a better safety profile in darker skin types (Fitzpatrick III-VI)
Non-Ablative Fractional Lasers (NAFL)
- 1550 nm (Fraxel Restore), 1540 nm - heat dermis without ablating epidermis
- Less downtime (2-3 days), lower risk of PIH
- Requires more sessions (4-6), less dramatic single-treatment improvement
- Better tolerated in darker skin types
Combination: Ablative + Non-Ablative
- A 2023 RCT (Kim et al., PMID: 37992744) found that combining fractional microneedling radiofrequency (FMRF) + ablative fractional CO2 laser significantly outperformed ablative laser alone for both acne and acne scars
Pulsed Dye Laser (PDL, 595 nm)
- First-line for hypertrophic scars, keloidal scars, and erythematous PIH
- Also used alongside isotretinoin (see below)
IPL (Intense Pulsed Light)
-
Effective for erythema and mild pigmentary changes post-acne
-
Useful adjunct, not primary treatment for textural scarring
-
Ziebart et al., J Drugs Dermatol 2024 [PMID: 39630683]
2. Microneedling and Combinations
A 2024 network meta-analysis (Li et al., Arch Dermatol Res) analyzed 24 RCTs with 1,546 participants and ranked treatments:
Ranking by efficacy (best to adequate):
- Microneedling + Chemical Peel - best overall in degree of improvement, patient satisfaction, and efficacy
- Microneedling + PRP - strong results, widely used
- Microneedling + Botulinum toxin-A - promising, especially for rolling scars
- Microneedling + Hyaluronic acid - good for skin texture
- Microneedling alone - effective but inferior to combinations
- PRP alone and Chemical Peel alone - less effective than microneedling combinations
Key finding: side effects (erythema, pain, PIH) were not significantly different across all treatment groups - meaning combination approaches gain efficacy without increasing harm.
- Li et al., Arch Dermatol Res 2024 [PMID: 39110247]
Fractional Microneedling Radiofrequency (FMRF)
- Delivers RF energy directly into dermis via insulated needles
- Stimulates deep collagen remodeling
- Particularly effective for rolling and boxcar scars
- Safer in darker skin types compared to ablative lasers (less epidermal damage)
- Evidence supports combination with ablative CO2 laser for enhanced results
3. Isotretinoin + Energy-Based Devices (Updated Evidence)
The traditional 6-month delay between isotretinoin and laser treatment is no longer evidence-based.
A 2024 systematic review (Xu et al., J Cosmet Dermatol) of 16 studies (including 6 RCTs) found:
-
PDL, NAFL, and FMRF are safe and effective during or immediately after isotretinoin treatment
-
The evidence does not justify delaying energy-based interventions for patients on isotretinoin
-
This is a significant protocol shift - early treatment of scars while controlling active acne is now recommended
-
Xu et al., J Cosmet Dermatol 2024 [PMID: 38845186]
⚠️ Note: Ablative CO2 laser remains cautious territory on isotretinoin - the evidence for safety is stronger for non-ablative and PDL modalities.
4. Chemical Peels
| Peel | Depth | Best For |
|---|---|---|
| Glycolic acid (20-70%) | Superficial | Mild PIH, surface texture |
| Salicylic acid (20-30%) | Superficial | Active acne + mild scars, oily skin |
| TCA CROSS (trichloroacetic acid 65-100%, focal) | Deep focal | Ice pick scars specifically |
| TCA 15-35% (full face) | Medium | Boxcar, surface irregularities |
| Jessner's solution | Superficial-medium | PIH, combined with TCA |
| Phenol peel | Deep | Severe atrophic scarring (light skin only) |
TCA CROSS (Chemical Reconstruction of Skin Scars) technique - focal application of high-concentration TCA into ice pick scar base - remains the most targeted non-laser approach for ice pick scars.
5. Subcision
- Technique: hypodermic needle or Nokor needle breaks fibrous bands tethering rolling scars to deep dermis
- Most effective for rolling scars
- Often combined with fillers (HA) or PRP injected immediately after to maintain separation
- Repeated sessions (3-5) typically needed
- Evidence is lower quality (uncontrolled studies) but clinical utility is well-established
6. Dermal Fillers
- Hyaluronic acid (HA) fillers: temporary (6-12 months), good for atrophic rolling/boxcar scars
- Poly-L-lactic acid (PLLA): biostimulatory, longer lasting
- Autologous fat grafting / lipoaspirate: emerging evidence for volume restoration in severe scarring
7. Platelet-Rich Plasma (PRP)
- Used as an adjunct, not monotherapy
- Injected alone or combined with microneedling, laser, or subcision
- Promotes collagen synthesis via growth factor release (TGF-β, PDGF, EGF)
- A 2025 systematic review (Periodontol 2000, PMID: 39086171) confirmed PRP's role in aesthetic regeneration, including acne scars
8. Punch Techniques (Surgical)
| Technique | Scar Type | Method |
|---|---|---|
| Punch excision | Ice pick, deep boxcar | Remove scar core, close primarily or graft |
| Punch elevation | Boxcar | Elevate scar base to surface level |
| Punch grafting | Deep ice pick | Fill with autologous graft |
Reserved for individual deep scars not responding to other treatments; can be followed by resurfacing at 4-6 weeks.
Practical Protocol by Severity
Mild Atrophic Scarring
- Topical retinoids + AHA/BHA
- Superficial chemical peels (glycolic/salicylic)
- 1-2 sessions microneedling
Moderate Atrophic Scarring (Mixed Types)
- Fractional non-ablative laser (4-6 sessions) OR FMRF
- Microneedling + PRP or chemical peel
- Subcision if rolling scars present
- TCA CROSS for any ice pick scars
Severe Atrophic Scarring
- Ablative fractional CO2 laser (1-3 sessions, spaced 3-4 months)
- Combined FMRF + AFL for maximal collagen remodeling
- Subcision + HA filler for rolling scars
- Punch excision/elevation for isolated deep scars
- Start energy treatments early - do not wait 6 months post-isotretinoin if using PDL or NAFL
Hypertrophic/Keloidal Scarring
- Intralesional triamcinolone (10-40 mg/mL) every 4-6 weeks
- PDL (595 nm) - reduces vascularity and flattens
- Silicone gel sheets (continuous use)
- Combined steroid + PDL superior to either alone
Key 2024-2025 Protocol Updates
| Old Thinking | Current Evidence |
|---|---|
| Wait 6 months post-isotretinoin before lasers | PDL, NAFL, FMRF are safe during/after isotretinoin - no delay needed |
| Microneedling alone is sufficient | Microneedling + chemical peel is now the best-ranked combination |
| One treatment type per session | Combination modalities in same session improve outcomes without added risk |
| Ablative laser is always best | FMRF offers comparable results with less downtime in appropriate candidates |
Summary of Evidence Strength
| Modality | Evidence Level |
|---|---|
| Ablative fractional lasers | Strong (multiple RCTs, meta-analyses) |
| Non-ablative fractional lasers | Strong |
| Microneedling ± PRP/chemical peel | Strong (2024 network meta-analysis, 24 RCTs) |
| FMRF | Moderate-strong (RCTs) |
| Chemical peels | Moderate |
| Subcision | Moderate (mostly cohort/uncontrolled) |
| Dermal fillers | Moderate |
| PRP monotherapy | Moderate (best as adjunct) |
| Punch techniques | Low (expert consensus, case series) |
Key References:
- Kim et al. (2023) - FMRF + CO2 laser RCT - Yonsei Med J
- Kim EY et al. (2023) - Evidence-based management of atrophic acne scarring - Arch Dermatol Res
- Li et al. (2024) - Microneedling network meta-analysis, 24 RCTs - Arch Dermatol Res
- Xu et al. (2024) - Isotretinoin + energy devices systematic review - J Cosmet Dermatol
- Ziebart et al. (2024) - Lasers for acne scarring review - J Drugs Dermatol
- Jennings et al. (2024) - JAAD acne scarring: pathophysiology and diagnosis - J Am Acad Dermatol
Treatment easy for neet pg
Acne Scarring Treatment - NEET PG Quick Revision
Scar Types (Memory First)
"Ice Box Rolls in a Keloid"
| Type | Shape | Site |
|---|---|---|
| Ice pick | Deep, narrow, V | Temples, cheeks |
| Boxcar | Broad, sharp walls | Cheeks |
| Rolling | Wavy, fibrous bands | Cheeks |
| Keloidal | Raised, firm | Neck, trunk |
Treatment by Scar Type - High Yield
| Scar | DOC / Best Tx |
|---|---|
| Ice pick | TCA CROSS (focal high-conc. TCA) + Punch excision |
| Boxcar | Ablative fractional CO2 laser + Subcision |
| Rolling | Subcision (breaks fibrous bands) + FMRF |
| Keloidal/Hypertrophic | Intralesional triamcinolone + PDL laser |
| PIH (dark spots) | Chemical peels + Topical retinoids + IPL |
| Erythema (red marks) | PDL (pulsed dye laser, 595 nm) |
Treatment Ladder (Severity-Based)
MILD → Topical retinoids + Chemical peels
↓
MODERATE → Microneedling + NAFL (non-ablative laser)
↓
SEVERE → Ablative CO2 laser + Subcision + Punch techniques
One-Liners for MCQs
- Best overall for atrophic scars - Ablative fractional CO2 laser
- Best for ice pick scars - TCA CROSS
- Best for rolling scars - Subcision
- Best for keloidal scars - Intralesional triamcinolone + PDL
- Best combination (network meta-analysis 2024) - Microneedling + Chemical peel
- PRP - Used as adjunct (NOT monotherapy); combined with microneedling/laser
- FMRF - Safer than CO2 in dark skin (Fitzpatrick III-VI); less PIH risk
- TCA CROSS - High concentration TCA (65-100%) applied focally into ice pick base
- Subcision tool - Nokor needle or hypodermic needle; breaks dermal tethering bands
- Punch excision - For single deep ice pick scars unresponsive to other treatment
Isotretinoin + Lasers - Exam Trap ⚠️
Old rule (WRONG now): Wait 6 months after isotretinoin before lasersCurrent evidence (2024): PDL, non-ablative laser, FMRF are SAFE during/after isotretinoin - no delay needed
Skin Type Matters (Fitzpatrick)
| Skin Type | Preferred Laser |
|---|---|
| Fair (I-III) | Ablative CO2 / Er:YAG |
| Dark (III-VI) | FMRF or Non-ablative 1550 nm (less PIH risk) |
Quick Mnemonics
- "SLIM" for atrophic scar treatments - Subcision, Laser, Injectable fillers, Microneedling
- PDL = Pulsed Dye Laser = Red/vascular lesions (erythema, keloids, telangiectasia)
- TCA CROSS = only for ice pick (focal, not full face)
Ug level treatment
Acne Vulgaris Treatment — UG Level (MBBS)
The 4 Goals of Treatment
- Reduce sebum production
- Normalize follicular keratinization (unclog pores)
- Kill Cutibacterium acnes
- Reduce inflammation
Step 1 — Classify Severity First
| Severity | Lesions |
|---|---|
| Mild | Comedones ± few papules/pustules |
| Moderate | Multiple papules, pustules, few nodules |
| Severe | Nodules, cysts, scarring |
Step 2 — Treatment by Severity
🟡 MILD Acne
Topical only:
- Topical retinoid (tretinoin 0.025-0.05%) — mainstay; comedolytic
- Benzoyl peroxide (BPO) 2.5-10% — bactericidal, no resistance
- Salicylic acid — keratolytic, OTC option
- Apply to entire face, not just spots
- Takes 8-12 weeks to show effect
🟠 MODERATE Acne
Topical + Oral combination:
| Drug | Dose | Notes |
|---|---|---|
| Topical retinoid | Nightly | Continue throughout |
| Topical BPO | Morning | Prevents antibiotic resistance |
| Doxycycline (oral) | 100 mg BD | First-line oral antibiotic |
| Minocycline (oral) | 50-100 mg OD/BD | If doxycycline fails |
⚠️ Always combine topical antibiotic with BPO to prevent C. acnes resistance ⚠️ Never use topical antibiotic alone long-term
🔴 SEVERE / Nodulocystic Acne
Drug of Choice = Isotretinoin (oral)
| Feature | Detail |
|---|---|
| Drug | 13-cis-retinoic acid (isotretinoin) |
| Dose | 0.5-1 mg/kg/day (weight-based) |
| Duration | Until cumulative dose ~120-150 mg/kg |
| MOA | ↓ Sebum (antisebaceous) + anti-inflammatory + ↓ C. acnes |
| Side effects | Dry skin, cheilitis (most common), teratogenicity |
| Monitoring | LFTs, lipids, pregnancy test |
| Contraindication | Pregnancy (Category X) |
📌 iPLEDGE Program (USA) — mandatory registration to prevent fetal exposure
Step 3 — Special Situations
Female Patients with Hormonal Acne
(Jawline, chin, premenstrual flares)
| Drug | Use |
|---|---|
| Oral contraceptive pills (OCPs) | FDA-approved for acne; ↓ androgens |
| Spironolactone 50-100 mg/day | Antiandrogen; safe, effective, durable |
Pregnancy
- Topical azelaic acid — safe
- Topical BPO — relatively safe
- Amoxicillin oral — if systemic needed (Category B)
- ❌ Avoid: tetracyclines, isotretinoin
All Topical Agents — Summary Table
| Agent | Action | Key Point |
|---|---|---|
| Tretinoin (retinoid) | Comedolytic, anti-inflammatory | Apply at night; 8-12 wk response |
| Adapalene | Retinoid; less irritating | Good starter retinoid |
| BPO | Bactericidal | No resistance; combine with antibiotics |
| Clindamycin | Anti-C. acnes | Never use alone; always + BPO |
| Erythromycin | Anti-C. acnes | High resistance now; avoid alone |
| Azelaic acid | Antimicrobial + anti-PIH | Good for dark skin; safe in pregnancy |
| Dapsone gel | Anti-inflammatory | Good for adult women |
| Salicylic acid | Keratolytic | OTC; mild acne |
| Clascoterone | Topical androgen blocker | Newest FDA-approved topical |
Oral Antibiotics — Summary
| Drug | Notes |
|---|---|
| Doxycycline | First-line; 100 mg BD; take with food |
| Minocycline | Second-line; vestibular SE (vertigo); pigmentation |
| Sub-antimicrobial doxycycline | 40 mg SR OD; anti-inflammatory only; no resistance |
| Amoxicillin | Pregnancy / tetracycline intolerance |
| Erythromycin | Pregnancy; high resistance |
📌 Limit antibiotics to 3 months — then switch to topical maintenance
Antibiotic Resistance — Prevention Rules
- Always combine oral/topical antibiotic with BPO
- Don't use oral + topical different antibiotics simultaneously
- Limit duration — move to isotretinoin if can't wean off antibiotics
- Same antibiotic on re-treatment unless lost efficacy
One Flow Chart
Acne
├── Mild ──────→ Topical retinoid ± BPO
├── Moderate ──→ Topical retinoid + BPO + Oral doxycycline
├── Severe ────→ Oral Isotretinoin
└── Female ────→ Add OCP or Spironolactone
Must-Know Exam Facts (UG)
| Question | Answer |
|---|---|
| DOC severe nodulocystic acne | Isotretinoin |
| MOA of isotretinoin | ↓ Sebum production (antisebaceous) |
| Most teratogenic anti-acne drug | Isotretinoin |
| Topical antibiotic always combined with | Benzoyl peroxide |
| Safe anti-acne drug in pregnancy | Azelaic acid / BPO / Amoxicillin |
| Antiandrogen for female acne | Spironolactone |
| Newest topical androgen blocker | Clascoterone |
| Time to judge topical treatment | 8-12 weeks |
| Open comedone (blackhead) color due to | Oxidized melanin (not dirt) |
Rccrine gland
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive textbook data. Here is the full answer:
Eccrine Gland (Eccrine Sweat Gland)
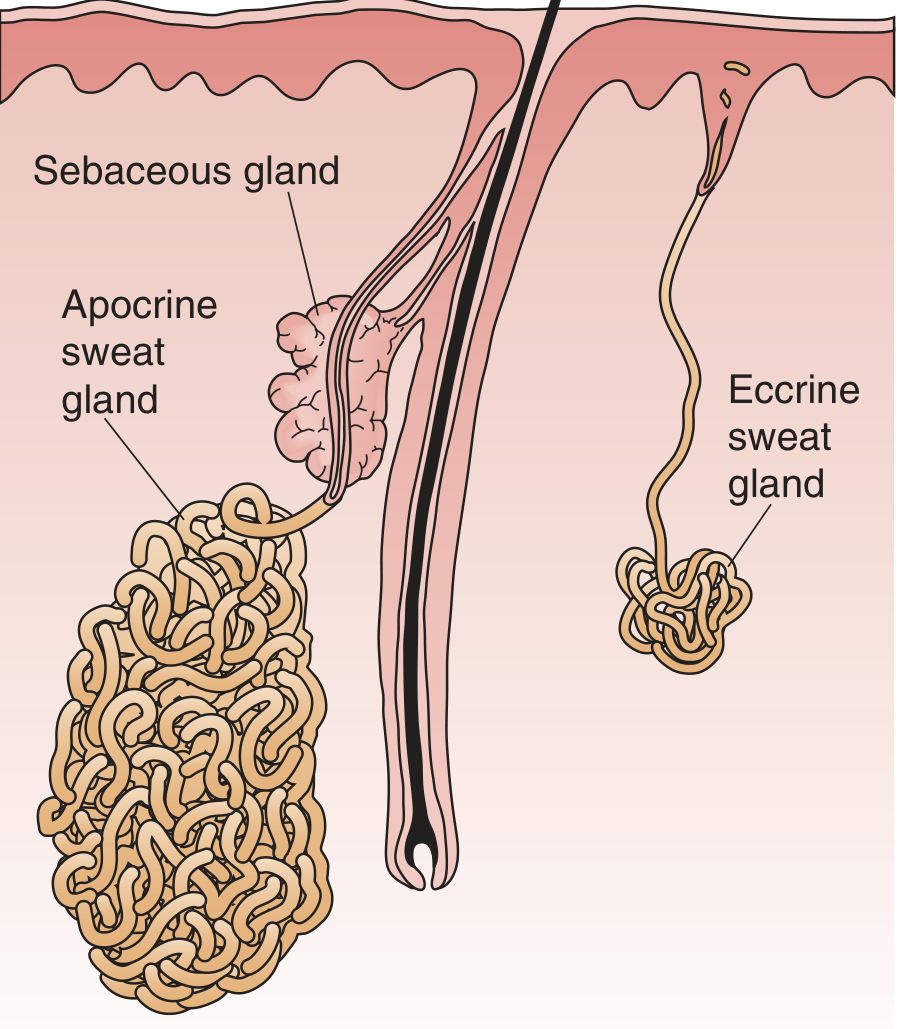
Eccrine vs Apocrine sweat glands - Medical Physiology (Boron & Boulpaep)
Structure
The eccrine gland is a simple tubular gland with two parts:
1. Secretory Coil (Acinus)
- Located deep in the dermis (or superficial panniculus in thick-skinned areas like the back)
- Blind-ended, coiled structure
- Lined by two cell types:
- Clear (pale) cells - large, glycogen-rich; initiate primary sweat formation
- Dark cells - smaller, darker; function like duct cells; reabsorb Na⁺
- Surrounded by a layer of myoepithelial cells (contract to express sweat pulsatilely; hydrostatic pressure can exceed 500 mmHg)
- Rich microvascular network surrounds the entire gland
2. Duct
-
Long, wavy tube passing outward through dermis → epidermis → sweat pore
-
Double layer of cuboidal epithelial cells, lined by an eosinophilic cuticle on the luminal side
-
Reabsorbs Na⁺ and Cl⁻, making final sweat hypotonic
-
Rich in mitochondria (high energy demand for sustained ion transport)
-
Andrews' Diseases of the Skin; Medical Physiology (Boron)
Location
- Found at virtually all skin sites in humans (unlike other mammals, where apocrine is dominant)
- Highest density: palms, soles, axillae, forehead
- Total number: ~2-4 million eccrine glands in humans
Eccrine vs Apocrine - Key Comparison
| Feature | Eccrine | Apocrine |
|---|---|---|
| Origin | Surface epidermis | Upper hair follicle (infundibulum) |
| Location | All skin sites | Axillae, genitals, areola, eyelids |
| Opens into | Skin surface (sweat pore) | Hair follicle |
| Secretion mode | Merocrine (exocytosis) | Decapitation secretion (apical cytoplasm pinched off) |
| Product | Clear, odorless, hypotonic | Milky white, protein/lipid-rich; odorless until bacteria act |
| Innervation | Cholinergic (sympathetic, unusual) | Adrenergic + circulating catecholamines |
| Stimulus | Heat + emotional stress | Emotional stress, hormones |
| Function | Thermoregulation | Pheromone-like signaling |
| Odor | None | Becomes odorous at skin surface (bacteria) |
| Development | Active postnatally | Quiescent in neonate; active post-puberty |
Physiology of Secretion
Step 1 - Primary Secretion (Coil)
- Stimulus → Heat / emotional stress → postganglionic sympathetic (cholinergic) fibers release acetylcholine
- ACh activates muscarinic receptors on acinar cells → activates phospholipase C → ↑ PKC + ↑ [Ca²⁺]ᵢ
- This triggers Cl⁻ secretion: Na⁺/K⁺/2Cl⁻ cotransporter brings Cl⁻ into cell across basolateral membrane → Cl⁻ exits apically through Cl⁻ channel
- Lumen-negative charge drives Na⁺ out paracellularly
- NaCl + urea + lactate in lumen → osmotic gradient → water follows → primary secretion is isotonic to plasma
Step 2 - Modification (Duct)
- Duct cells reabsorb Na⁺ via apical ENaC (epithelial Na⁺ channel)
- Cl⁻ reabsorbed via CFTR (cystic fibrosis transmembrane conductance regulator)
- Duct has low water permeability → water cannot follow → final sweat is hypotonic
Final sweat composition
-
Hypotonic to plasma
-
Contains: Na⁺, Cl⁻, K⁺, urea, lactate
-
Same electrolytes as plasma but more dilute
-
Medical Physiology (Boron & Boulpaep), p. 1778-1779
Flow Rate and NaCl Content
| Condition | Sweat Rate | Duct Reabsorption | Final [NaCl] |
|---|---|---|---|
| Mild sweating | Low | Nearly complete | ~10-20 mEq/L |
| Intense sweating | High | Overwhelmed | ~60-70 mEq/L |
| Acclimatization | High | Aldosterone ↑ reabsorption | Low (conserves salt) |
Acclimatization to heat → aldosterone → ↑ ENaC expression in duct → more Na⁺ reabsorption → more hypotonic sweat → salt conservation
Cystic Fibrosis - Classic Eccrine Connection
- CFTR is the Cl⁻ channel in duct cells
- In CF: CFTR mutated → Cl⁻ cannot be reabsorbed → Na⁺ stays in lumen too → sweat rich in NaCl
- Basis of the sweat chloride test: sweat Cl⁻ >60 mEq/L = diagnostic of CF
- Medical Physiology (Boron), p. 1779
Development
-
Palmoplantar eccrine glands: first to develop; begin during 1st trimester
-
Fully developed by 2nd trimester
-
Canalization of dermal duct: complete by 16 weeks EGA
-
Canalization of epidermal duct: complete by 22 weeks EGA
-
Interfollicular (general body) eccrine glands: form during 5th month of gestation
-
Eccrine glands mature and become functional postnatally (unlike apocrine, which is transiently active in utero then quiescent)
-
Dermatology 2-Volume Set 5e, p. 2632-2636
Disorders of Eccrine Glands
| Disorder | Key Feature |
|---|---|
| Hyperhidrosis | Excess sweating; primary (idiopathic, palmoplantar/axillary) or secondary; treated with antiperspirants (AlCl₃), botulinum toxin, iontophoresis, surgery |
| Anhidrosis / Hypohidrosis | Absent/reduced sweating; risk of hyperthermia; seen in ectodermal dysplasia |
| Miliaria | Obstruction of sweat duct; subtypes by level of blockage |
| Neutrophilic Eccrine Hidradenitis (NEH) | After cytotoxic drugs (esp. cytarabine, doxorubicin); perieccrine neutrophilic infiltrate; self-limiting |
| Syringosquamous Metaplasia | Chemotherapy-induced (esp. cytarabine); squamous metaplasia of upper duct |
| Hypohidrotic Ectodermal Dysplasia | Mutation in EDA/EDAR pathway; absent/↓ sweat glands + hypotrichosis + hypodontia |
Miliaria Subtypes (High Yield)
| Type | Level of Obstruction | Lesion | Setting |
|---|---|---|---|
| Miliaria crystallina | Stratum corneum (most superficial) | Clear, non-inflamed vesicles | After fever, neonates |
| Miliaria rubra ("prickly heat") | Stratum spinosum | Red papules/vesicles, itchy | Hot humid climate |
| Miliaria profunda | Dermoepidermal junction (deepest) | Flesh-colored papules, no itch | Tropics, repeated miliaria |
High-Yield Facts for Exams
| Question | Answer |
|---|---|
| Innervation of eccrine gland | Cholinergic sympathetic (unusual - sympathetic but ACh, not noradrenaline) |
| Innervation of apocrine gland | Adrenergic |
| Primary secretion of eccrine | Isotonic to plasma |
| Final sweat | Hypotonic (duct reabsorbs NaCl) |
| Sweat chloride raised in | Cystic fibrosis (CFTR defect in duct) |
| Eccrine opens into | Skin surface directly (NOT hair follicle) |
| Apocrine opens into | Hair follicle |
| Most common sweat gland in humans | Eccrine (all skin sites) |
| Secretion mode of eccrine | Merocrine |
| Secretion mode of apocrine | Decapitation (apocrine) secretion |
| Drug that prevents NEH | Dapsone (prophylactic) |
| Cytotoxic drug most linked to NEH | Cytarabine |
| Ectodermal dysplasia pathway | EDA/EDAR signaling |
- Andrews' Diseases of the Skin; Medical Physiology (Boron); Dermatology 2-Volume Set 5e; Fitzpatrick's Dermatology
Rosacea
Finding Sources
Reading File
Reading File
Searching PubMed
"rosacea"[MeSH Terms] AND treatment
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I have all I need for a comprehensive answer. Let me compile it now.
Rosacea

Definition
Rosacea is a chronic inflammatory disease of the facial pilosebaceous units and blood vessels, characterized by persistent central facial erythema, telangiectasia, flushing, papules, and pustules - occurring in the absence of comedones (key distinguishing feature from acne vulgaris).
Epidemiology
- Affects up to 3% of the US population
- Most common in light-skinned women aged 30-50 (Celtic/northern European descent)
- Severe phymatous type (rhinophyma) occurs almost exclusively in men
- Ocular rosacea occurs equally in men and women
- Associated comorbidities: migraine, cardiovascular disease, IBD
Subtypes (2017 NRS Classification)
| Subtype | Key Features |
|---|---|
| 1. Erythematotelangiectatic (ETR) | Persistent central facial erythema + telangiectasia; prolonged flushing (>10 min); easily irritated skin; burning/stinging without sweating |
| 2. Papulopustular | Strikingly red central face + erythematous papules + pinpoint pustules; NO comedones; may have edema (Morbihan disease) |
| 3. Phymatous | Thickened skin, widened pores; rhinophyma (bulbous nose); almost exclusively men |
| 4. Ocular | Blepharitis, chalazion, conjunctivitis, keratitis; gritty/burning eyes; may precede skin disease |
Morbihan disease = solid facial edema complicating papulopustular/glandular rosacea; forehead, eyelids, cheeks affected
Clinical Images

Stages (Robbins)
- Pre-rosacea - flushing episodes only
- Persistent erythema + telangiectasia
- Papules and pustules
- Rhinophyma - permanent nasal thickening from sebaceous gland hypertrophy + follicular plugging
Triggers (Aggravating Factors)
- Sun exposure (most important)
- Heat, hot beverages, hot baths
- Alcohol (esp. red wine)
- Spicy foods
- Emotional stress
- Exercise
- Cold weather
- Topical corticosteroids (long-term use on face can induce/worsen rosacea)
Key exam fact: Flushing lasts >10 minutes, without sweating, lightheadedness, or palpitations (distinguishes from carcinoid/phaeochromocytoma)
Pathogenesis
Multifactorial and incompletely understood:
-
Innate immune dysregulation
- ↑ cutaneous cathelicidin antimicrobial peptides (qualitatively abnormal due to alternative processing by kallikrein 5 / stratum corneum tryptic enzyme)
- TLR2 activation → upregulates kallikrein 5 in keratinocytes → aberrant cathelicidin → inflammation + vascular dilation
- When cathelicidin peptides from rosacea patients are injected into mice - they induce rosacea-like changes
-
Neurovascular dysregulation
- Abnormal vasomotor response to thermal and other stimuli
- Chronic vasodilation → edema → compromise of lymphatic drainage → telangiectasia + fibrosis
-
Chronic solar damage
- Important especially in ETR subtype; dermal matrix and ground substance damage
-
NOT implicated (despite popular belief):
- Demodex and Helicobacter pylori - extensively investigated; not central to etiology
- Pilosebaceous/androgen abnormalities - not typically part of pathogenesis (except possibly glandular type)
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 158-159
- Andrews' Diseases of the Skin, p. 292-293
Histopathology (Robbins)
- Nonspecific perifollicular infiltrate - lymphocytes + dermal edema + telangiectasia
- Pustular phase: neutrophils colonize follicles; follicle rupture → granulomatous dermal response
- Rhinophyma: hypertrophy of sebaceous glands + follicular plugging by keratotic debris
Ocular Rosacea
- Blepharitis, recurrent chalazion, conjunctivitis
- Keratitis, iritis, episcleritis (sight-threatening)
- Abnormal Schirmer test in 40% of rosacea patients
- Symptoms: gritty, stinging, itchy, burning eyes; photophobia; foreign body sensation
- May precede skin disease - always ask about eye symptoms in rosacea
- Managed by ophthalmologist in conjunction with dermatologist
Treatment
General Measures (All Types)
- Sun protection - broad-spectrum SPF ≥30 daily (most important)
- Identify and avoid individual triggers (food diary, avoid alcohol, spicy foods)
- Gentle non-irritating skincare; avoid harsh cleansers, astringents
- Green-tinted cosmetics to neutralize redness
Topical Therapy (Mild-Moderate)
| Agent | Use | Notes |
|---|---|---|
| Metronidazole 0.75-1% cream/gel | Papulopustular | First-line topical; anti-inflammatory |
| Azelaic acid 15% gel | Papulopustular + ETR | Anti-inflammatory + antikeratinizing; good for PIH |
| Ivermectin 1% cream | Papulopustular | Newer agent; anti-Demodex + anti-inflammatory; once daily |
| Brimonidine 0.33% gel | Erythema (ETR) | α2-adrenergic agonist; vasoconstrictor; for persistent redness only; paradoxical rebound erythema possible |
| Oxymetazoline 1% cream | Erythema (ETR) | α1-adrenergic agonist; for persistent facial erythema |
| Tacrolimus / Pimecrolimus | Steroid-induced rosacea | Used when withdrawing topical steroids |
Ivermectin vs metronidazole: Ivermectin 1% once daily is superior to metronidazole 0.75% twice daily for papulopustular rosacea (multiple RCTs)
Systemic Therapy (Moderate-Severe)
| Drug | Dose | Indication |
|---|---|---|
| Sub-antimicrobial doxycycline | 20 mg BD or 40 mg SR OD | Mild-moderate inflammatory rosacea; anti-inflammatory only, no resistance |
| Doxycycline | 100 mg BD | Moderate-severe papulopustular |
| Minocycline | 100 mg BD | Alternative to doxycycline |
| Low-dose isotretinoin | 0.25 mg/kg/day | Severe/refractory; especially glandular/phymatous type |
| Carvedilol (β-blocker) | Low dose | Severe flushing/persistent erythema; non-selective β-blocker |
2025 meta-analysis (King et al., PMID: 39239956): Low-dose isotretinoin is effective and safe for rosacea management - particularly for the glandular and papulopustular subtypes unresponsive to antibiotics.
Physical/Laser Treatments
| Modality | Indication |
|---|---|
| PDL (Pulsed Dye Laser, 595 nm) | Telangiectasia, persistent erythema |
| IPL (Intense Pulsed Light) | Erythema, telangiectasia, flushing |
| CO2 laser / Electrosurgery / Dermabrasion | Rhinophyma (surgical reshaping) |
| Radiofrequency | Telangiectasia; compared favorably to PDL in some trials |
2024 meta-analysis (Zhai et al., PMID: 39240125): Both IPL and PDL are effective for rosacea; IPL may have a slight advantage for erythema reduction, PDL for individual telangiectasia.
Steroid-Induced Rosacea - Special Protocol
- Stop topical corticosteroid
- Start topical tacrolimus (calcineurin inhibitor)
- Cover with short-term oral doxycycline or minocycline (tacrolimus alone can paradoxically worsen flushing)
- Resolution expected within 2 months
Ocular Rosacea Treatment
- Lid hygiene (warm compresses, lid scrubs)
- Lubricating eye drops
- Topical cyclosporine eye drops
- Oral doxycycline - first-line systemic; improves both skin and eye disease
- Ophthalmology referral for keratitis, iritis, or vision-threatening disease
Key Differentiating Features
Rosacea vs Acne Vulgaris
| Feature | Rosacea | Acne Vulgaris |
|---|---|---|
| Comedones | Absent | Present (hallmark) |
| Age | >30 years | Teens/young adults |
| Location | Central face (convexities) | Face, chest, back |
| Sebum/oily skin | Not typical (except glandular) | Yes |
| Androgens | Not implicated | Yes |
| Flushing | Prominent | Not a feature |
| Telangiectasia | Yes | No |
| C. acnes | Not central | Central pathogen |
Rosacea vs SLE Malar Rash
| Feature | Rosacea | SLE Malar Rash |
|---|---|---|
| Spares nasolabial folds | No (involves convexities) | Yes (classic) |
| Papules/pustules | Yes | No |
| Telangiectasia | Yes | No |
| Systemic features | No | Yes (joints, renal, etc.) |
Exam High-Yield Summary
| Fact | Answer |
|---|---|
| Key differentiating feature from acne | No comedones in rosacea |
| Most important trigger | Sun exposure |
| Phymatous change almost exclusively in | Men |
| Rhinophyma pathology | Hypertrophy of sebaceous glands + follicular plugging |
| Pathogenesis key molecule | Abnormal cathelicidin (via kallikrein 5 / TLR2 pathway) |
| "Demodex causes rosacea" | False - not proven to be central cause |
| Topical for erythema only | Brimonidine gel (α2-agonist vasoconstrictor) |
| Newest topical (best for papulopustular) | Ivermectin 1% cream |
| Sub-antimicrobial doxycycline dose | 40 mg SR once daily |
| Rhinophyma treatment | CO2 laser / surgical reshaping |
| Ocular rosacea Schirmer test | Abnormal in 40% |
| Steroid-induced rosacea: stop steroid + give | Tacrolimus + oral antibiotic |
| Morbihan disease | Solid facial edema from rosacea (lymphedema) |
Sources:
- Andrews' Diseases of the Skin, pp. 291-295
- Goldman-Cecil Medicine 2-Volume Set, p. 4452-4457
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 158-164
- King et al., J Eur Acad Dermatol Venereol 2025 [PMID: 39239956] - low-dose isotretinoin for rosacea
- Zhai et al., J Cosmet Dermatol 2024 [PMID: 39240125] - IPL vs PDL meta-analysis
This is a shared conversation. Sign in to Orris to start your own chat.