Heat stroke
Reading File
Finding Sources
Searching PubMed
"heat stroke" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of heat stroke based on authoritative emergency medicine textbooks.
Heat Stroke
Heat stroke is an acute, life-threatening emergency with high mortality if left untreated. It is defined by two cardinal features:
- Hyperthermia - core temperature >40°C (>104°F)
- Altered mental status
Types
| Type | Also Called | Who it Affects | Sweating |
|---|---|---|---|
| Classic | Non-exertional | Elderly, chronically ill, sedentary | Often absent (anhidrosis) |
| Exertional (EHS) | EHS | Athletes, military recruits, manual laborers | Usually present (profuse sweating) |
The clinical distinction between the two types is not critical for management - immediate cooling is the priority for both.
Clinical Features
Neurological (CNS is particularly vulnerable):
- The cerebellum is highly heat-sensitive; ataxia is an early sign
- Irritability, confusion, bizarre behavior, combativeness, hallucinations
- Decorticate/decerebrate posturing, hemiplegia, status epilepticus, coma
- Seizures are common, especially during cooling
Cardiovascular:
- Tachycardia, widened pulse pressure, arrhythmia
- Hypotension (common initial finding)
Other:
- Tachypnea (PaCO2 often <20 mmHg from hyperventilation)
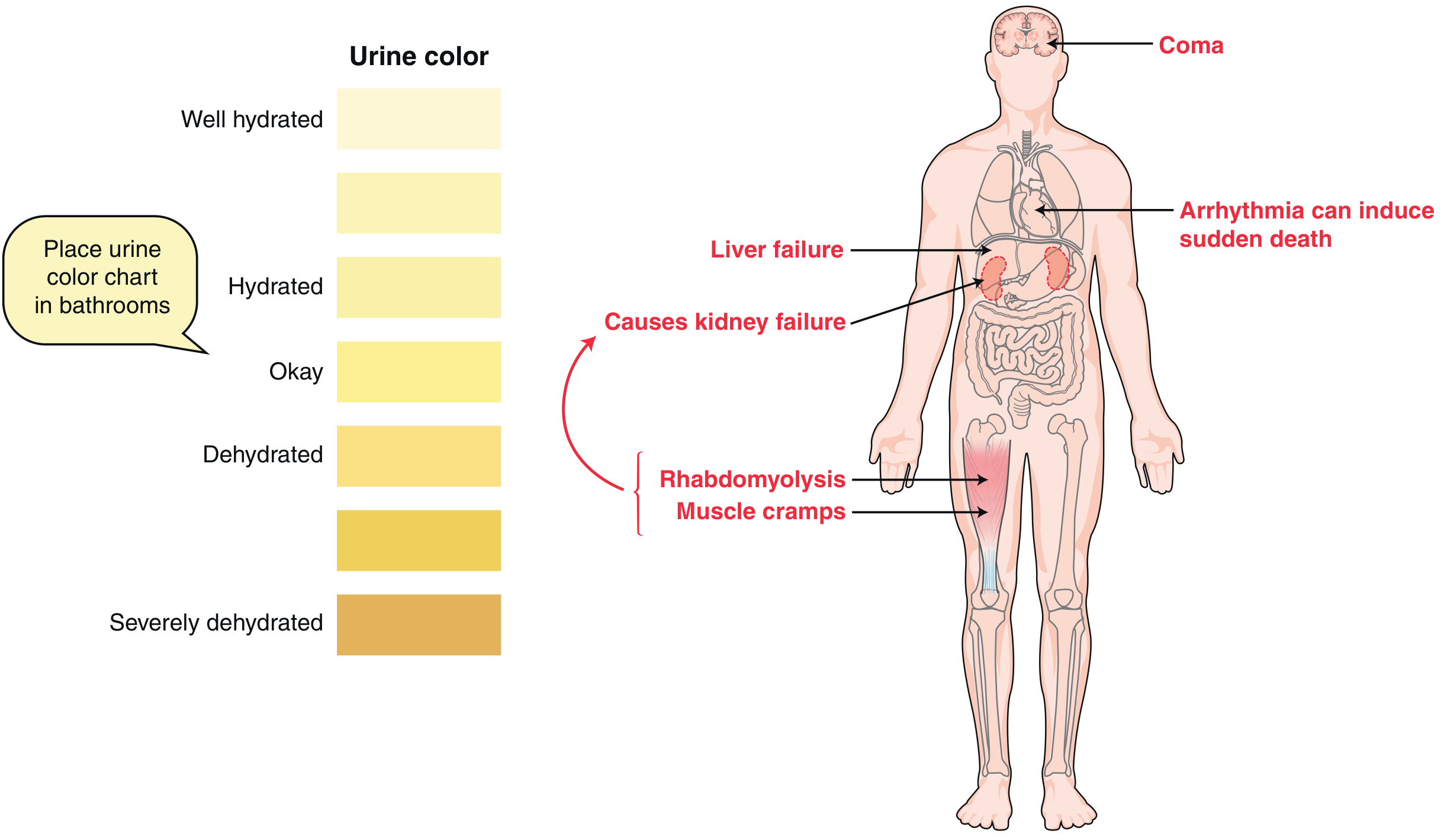
- Nausea/vomiting, oliguria
- Rhabdomyolysis, muscle cramps, flaccidity
- Lactic acidosis and hypoglycemia in exertional type
Diagnosis
There are no diagnostic tests - diagnosis is by history, clinical presentation, and exclusion of other causes.
Workup (directed at end-organ damage):
- CBC, comprehensive metabolic panel, ABG
- Coagulation profile (PT, PTT, fibrinogen)
- CPK, myoglobin, urinalysis (rhabdomyolysis screen)
- ECG, chest X-ray
- Head CT and LP if needed to rule out other causes
Differential Diagnosis:
| Infectious | Neurologic | Endocrine | Toxicologic |
|---|---|---|---|
| Sepsis, meningitis, encephalitis, malaria, typhoid, tetanus | Hypothalamic bleed/infarct, CVA, status epilepticus | Thyroid storm, pheochromocytoma, DKA | Anticholinergic toxidrome, sympathomimetic OD, serotonin syndrome, malignant hyperthermia, NMS |
Management
Prehospital
- Remove from hot environment immediately
- Remove clothing
- Start cooling: spray water + airflow (preferred), wet towels/sheets, or ice packs
- IV normal saline 1-2 L bolus if hypotensive
- Check point-of-care glucose
Emergency Department
Goal: Immediate cooling + aggressive organ support
- Monitor core temperature continuously (rectal thermometer, Foley thermistor, or esophageal probe)
- Target: reduce core temperature to ~39°C (102.2°F) - avoid overshoot hypothermia
Cooling Techniques (none proven superior):
| Method | Notes |
|---|---|
| Evaporative cooling | Remove clothing, spray cool water (~15°C), direct fan; well-tolerated, practical |
| Ice water immersion | Most efficient for young/healthy patients; difficult for monitoring/resuscitation |
| Ice packs to neck, axillae, groin | Readily available adjunct |
- Shivering during cooling: treat with short-acting benzodiazepines (first-line) or phenothiazines (second-line - note: lower seizure threshold, cause hypotension)
- Seizures: benzodiazepines
Hemodynamics:
- IV fluids for hypotension; if low cardiac output + elevated CVP persists after 20 mL/kg bolus - add dopamine or dobutamine
- Avoid norepinephrine (alpha-adrenergic vasoconstriction redirects blood away from skin, impairing cooling)
Complications
Early
- Hypotension, hypothermic overshoot, hyperthermic rebound
- Rhabdomyolysis, oliguria
- Delirium/coma, seizures
- Heart failure, pulmonary edema
- Hypokalemia, hypernatremia/hyponatremia
Late
- Renal failure (direct thermal injury + rhabdomyolysis + volume depletion)
- DIC (thermal endothelial injury → platelet aggregation, clotting factor deactivation)
- Hepatic dysfunction - centrilobular necrosis; peaks at 24-72 hours post-insult (usually reversible)
- ARDS
- Cerebral edema, persistent neurologic deficits
- Myocardial injury, intestinal ischemia, pancreatic injury
- Hyperkalemia (from AKI + rhabdomyolysis), hypocalcemia, hyperuricemia
Mortality predictors: degree of temperature elevation, time to cooling initiation, number of organ systems involved. Anuria, coma, and cardiovascular failure on presentation carry a significantly worse prognosis.
Disposition
- Heat stroke → ICU admission (especially if intubated, hemodynamically unstable, requiring invasive monitoring, or ongoing cooling)
- Minor heat emergencies (heat cramps, heat edema, heat stress) → ED treatment + discharge with instructions
Special Populations
- Elderly: Higher mortality; impaired thermoregulation, immobility, polypharmacy (diuretics, anticholinergics), poor housing insulation
- Young children: Immature thermoregulatory system; cannot self-rescue from hot environments (e.g., closed cars)
- Adolescents/athletes: Poor judgment in heat; require 10-14 days of acclimatization before intense activity - most early-season deaths occur in the first 4 days of practice
Prevention
- Reschedule strenuous activity to cooler times of day
- Wear light, loose-fitting clothing
- Increase carbohydrates, decrease protein intake (reduces endogenous heat production)
- Drink fluids proactively (even when not thirsty)
- Avoid alcohol
- Avoid direct sunlight; use shade
- Allow adequate acclimatization (10-14 days for athletes)
Sources: Tintinalli's Emergency Medicine, Chapter 210; Miller's Review of Orthopaedics, 9th Edition, p. 411
This is a shared conversation. Sign in to Orris to start your own chat.