Write this more organized from standard opthal textbooks like khurana or basar and send me not that detailed but just approbation info regarding the orcoedure if possible attach the pictures of the relevant instruments mentioned
Reading File
Reading File
Running Command
Finding Sources
Finding Sources
Running Command
Finding Sources
Running Command
Finding Sources
Running Command
Finding Sources
Running Command
Reading File
Running Command
Loading Image
Reading File
Finding Sources
Reading File
Searching Content
Searching Content
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have all the material I need. I can see from the OCR that your notes cover both SICS/MSICS and phacoemulsification. The Kanski text confirms MSICS steps. Let me also grab the Fig 10.11B (trypan blue staining) image - it should be near line 7008. Let me now compile the full organized response.
Small Incision Cataract Surgery (SICS / MSICS)
Reorganized from Kanski's Clinical Ophthalmology, 10th ed.
Overview
Manual Small-Incision Cataract Surgery (MSICS) is a variant of extracapsular cataract extraction (ECCE). It was developed for high-volume surgical management of dense cataracts, particularly in lower-resource settings. It does not require phacoemulsification technology yet achieves comparable visual outcomes.
"MSICS is faster and avoids the need for expensive technology. Visual rehabilitation is comparable to phacoemulsification."
- Kanski's Clinical Ophthalmology, 10th ed., p. 336
Context: Cataract Extraction Methods
| Technique | Incision | Key Feature |
|---|---|---|
| ICCE (old) | ~12 mm | Whole lens + capsule removed; cryoprobe used |
| ECCE (conventional) | 8-10 mm | Nucleus expressed; sutures required; risk of astigmatism |
| MSICS | ~5-7 mm | Self-sealing sclero-corneal tunnel; no sutures needed |
| Phacoemulsification | 2.4-2.8 mm | Ultrasonic fragmentation; most technologically advanced |
Pre-operative Preparation
- Position: Supine on operating table
- Antisepsis: Povidone-iodine (Betadine) 5% applied to the periocular area
- Draping & Speculum: Universal (lid) speculum to keep eye open
- Microscope: Operating microscope; interpupillary distance adjusted for monocular viewing
Anaesthesia
Performed under local anaesthesia (LA). Two main options:
1. Topical / Surface Anaesthesia
- Agent: Oxybuprocaine (proxymetacaine) eye drops
- Quick, avoids injection; ~5% of patients still experience intraoperative pain
2. Peribulbar Block (preferred for SICS/MSICS)
- Injection sites:
- Upper lateral 1/3 of the orbit
- Lower medial 2/3 / lateral 1/3 junction
- Nerves blocked: CN III, V (branches), VI, and VII (orbicularis) - i.e., cranial nerves 3, 5, 6, and 7
- Provides both akinesia and analgesia
Sub-Tenon's block (blunt cannula injection under Tenon's capsule) is an alternative with fewer complications than sharp needle blocks.
Surgical Steps
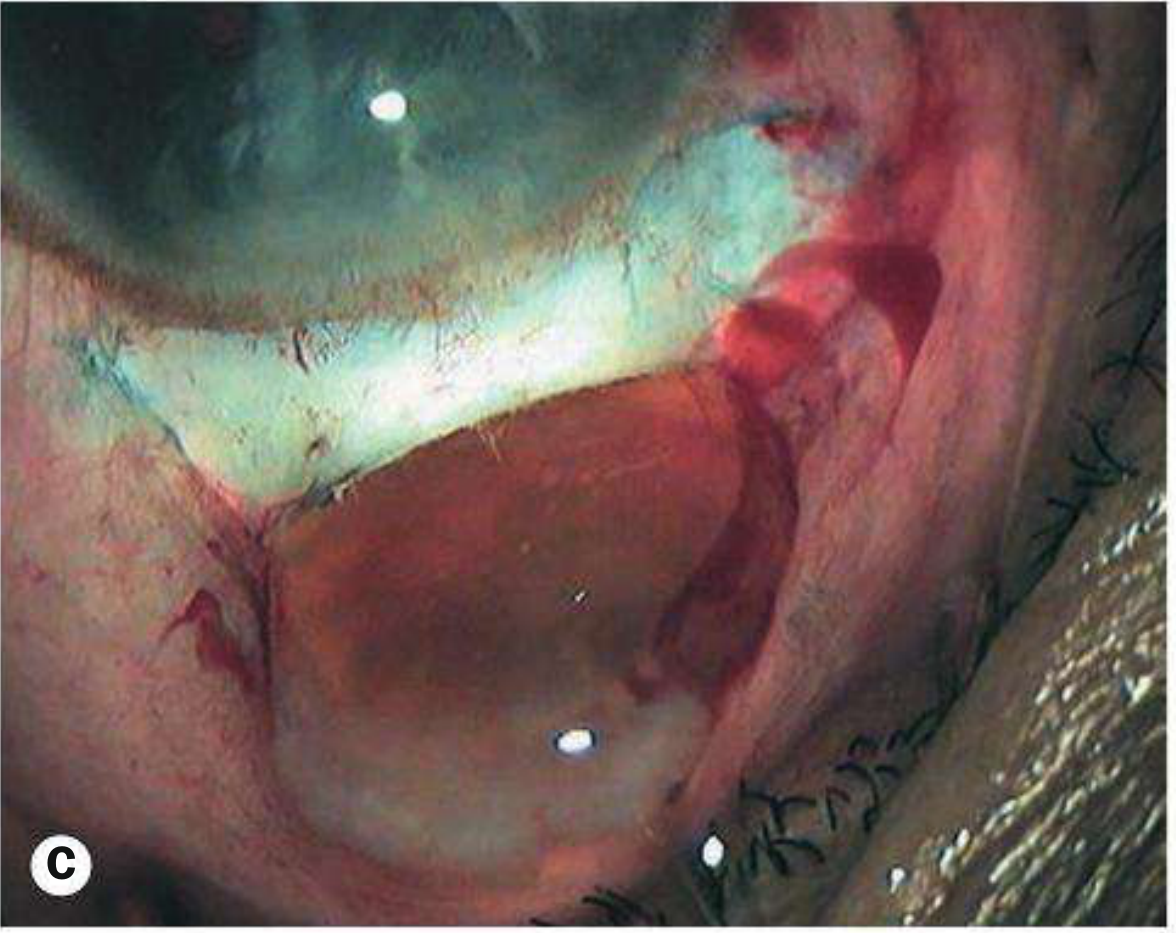
Step 1 - Sclero-Corneal Tunnel Incision
A self-sealing scleral tunnel is constructed starting ~2 mm posterior to the limbus:
- Incision length: ~5-7 mm (allowing nucleus delivery without sutures)
- Tunnel is beveled to create a valve effect - no sutures required
- Internal opening into anterior chamber is slightly larger than external opening
Instrument: Crescent knife / scleral tunnel knife (preset blade)
Step 2 - Side Port Entry
A small paracentesis (side port) is made at approximately 90° from the main incision using a:
- Instrument: Microvitreoretinal (MVR) blade or keratome (preset to 2.8 mm)
- Provides entry for second instrument (chopper/vectis)
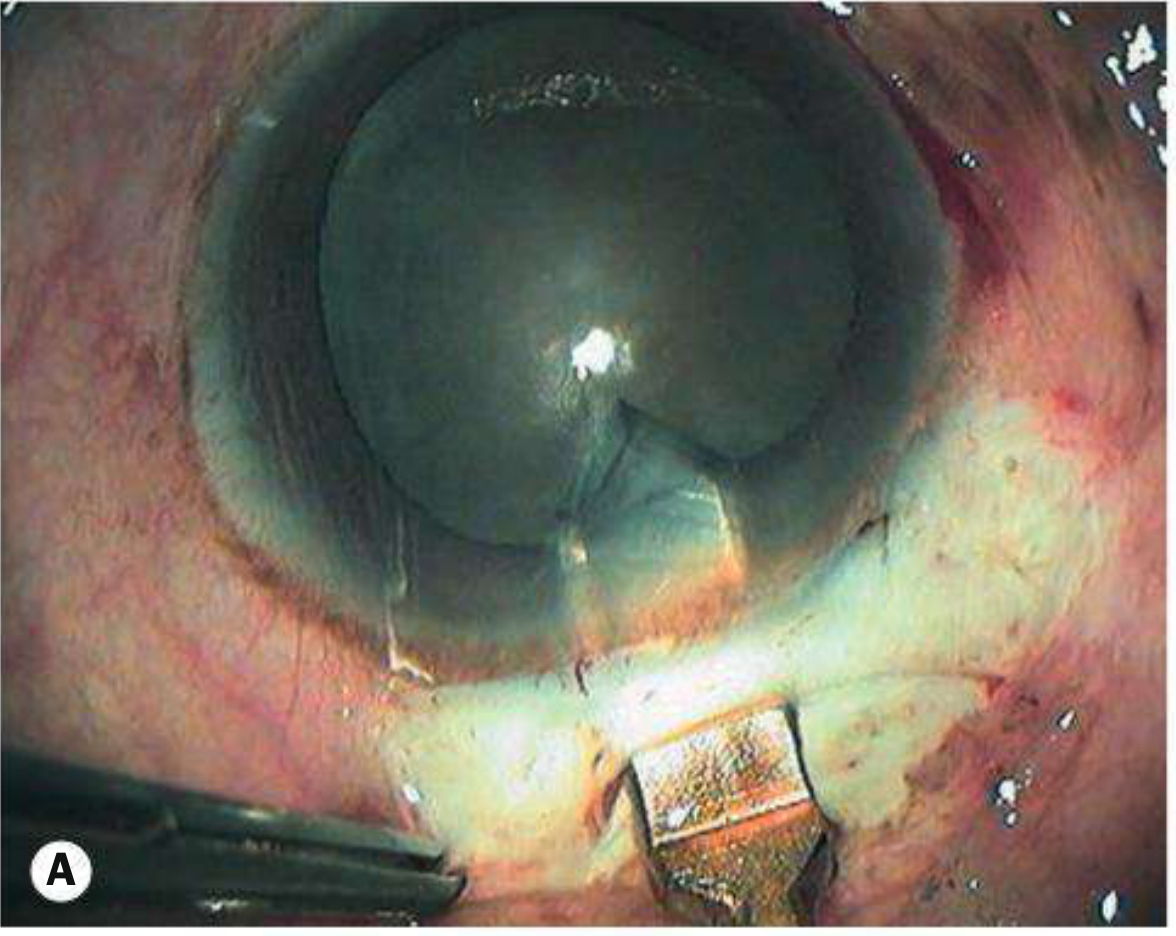
Step 3 - Anterior Capsulotomy (CCC)
- Staining: Trypan blue dye injected under viscoelastic to stain the anterior capsule blue (essential for visualization, especially in mature cataracts with absent red reflex)
- Technique: Continuous curvilinear capsulorhexis (CCC) performed with cystotome or Utrata forceps
- No capsular tags are permitted - an intact, round rhexis is essential
Step 4 - Hydrodissection
- Balanced salt solution (BSS) injected beneath the anterior capsule using a hydrodissection cannula to separate the lens cortex from the capsule
- Confirmed when the lens rotates freely within the capsular bag
- Hydrodelineation (injection into the nucleus) can also be performed to separate the nucleus from the epinucleus
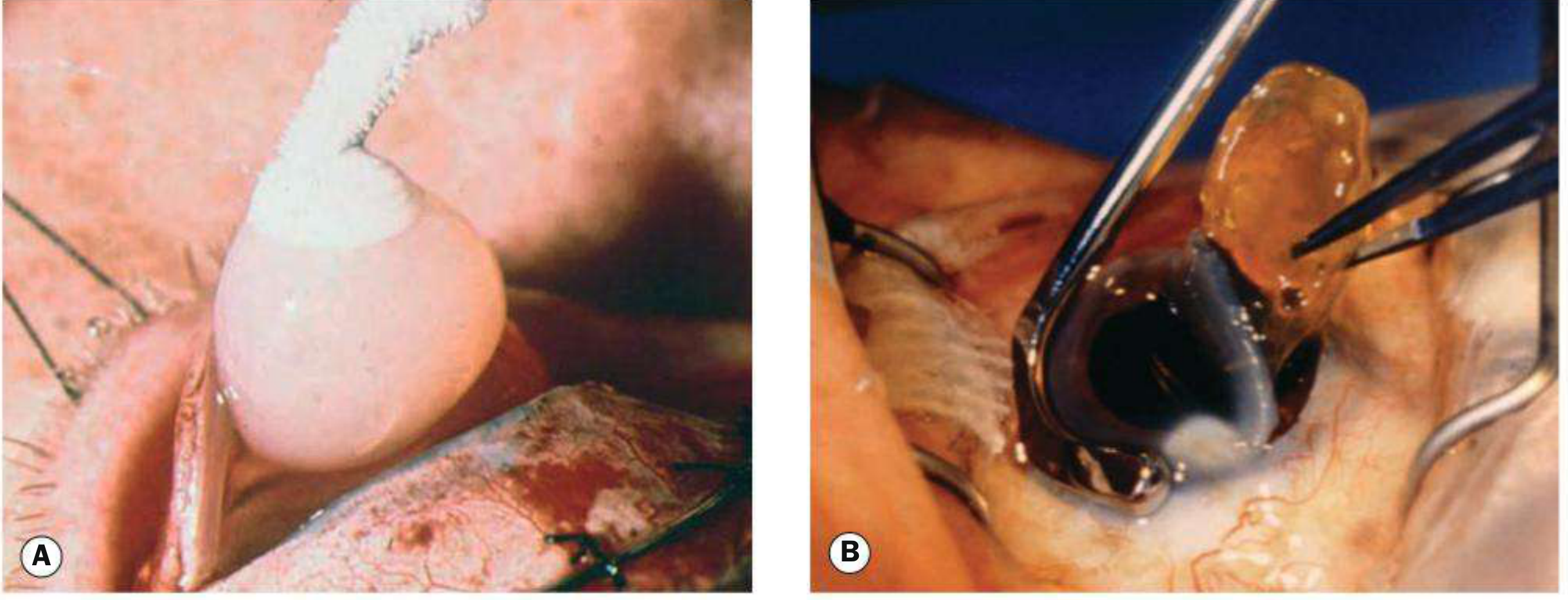
Step 5 - Nucleus Expression
The nucleus is delivered en bloc through the tunnel using an irrigating vectis (wire loop with infusion):
- Viscoelastic is injected into the anterior chamber first to protect the endothelium
- The vectis slides beneath the nucleus and the nucleus is gently expressed out through the tunnel
- This is the key distinction from phaco - no fragmentation required
Step 6 - Cortical Aspiration
Residual cortical material is aspirated using a:
- Simcoe cannula (double-lumen: one lumen irrigates, other aspirates simultaneously)
- Manual irrigation-aspiration cleans the capsular bag
Step 7 - IOL Implantation
- Viscoelastic (OVD) re-injected into the capsular bag and anterior chamber
- Preferred OVDs: sodium hyaluronate (highest molecular weight, best protection) or hydroxymethylcellulose
- A rigid PMMA IOL (one-piece, designed for MSICS) or foldable IOL implanted into the capsular bag
- After IOL placement, viscoelastic is thoroughly irrigated out to prevent postoperative IOP rise / secondary glaucoma
- IOP maintained post-irrigation with Ringer's lactate
Step 8 - Wound Closure
- The self-sealing tunnel requires no sutures in most cases
- Wound integrity checked by gentle pressure / cotton swab; anterior chamber must be well-formed
- Corneal wound sealed by hydration with BSS if needed
Key Instruments Summary
| Instrument | Use |
|---|---|
| Universal speculum | Lid retraction |
| Crescent / tunnel knife | Sclero-corneal tunnel construction |
| MVR blade / keratome (2.8 mm) | Side port / paracentesis |
| Cystotome / Utrata forceps | Capsulorhexis |
| Hydrodissection cannula | Cortical separation |
| Irrigating vectis | Nucleus delivery |
| Simcoe cannula | Cortical aspiration (I/A) |
| PMMA or foldable IOL injector | Lens implantation |
MSICS vs Phacoemulsification
| Feature | MSICS | Phaco |
|---|---|---|
| Incision | ~5-7 mm scleral tunnel | 2.4-2.8 mm clear corneal |
| Technology needed | Low (manual) | High (phaco machine) |
| Cost | Low | High |
| Dense cataracts | Excellent | Challenging (high power needed) |
| Astigmatism | Low (scleral incision) | Very low |
| Visual outcomes | Comparable | Comparable |
| Sutures | Usually none | None |
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition, Chapter 10 - Cataract (pp. 335-336)
Send me the clean pdf form of this
Reading File
Running Command
Writing File
Running Command
Running Command
Your PDF is ready. Here it is:
SICS MSICS Ophthalmology
PDF Document · PDF
The PDF includes:
- Titled header banner with source citation
- Comparison table - ICCE vs ECCE vs MSICS vs Phaco
- Pre-op prep & anaesthesia sections (topical, peribulbar, sub-Tenon's)
- 8 numbered surgical steps in styled step-boxes
- 3 intraoperative images from Kanski's Fig. 10.10 and 10.11 (ICCE/ECCE comparison, scleral tunnel, trypan blue/nucleus expression)
- Instruments table and MSICS vs Phaco comparison table
- Footer source line
U have mixed both scis and pacho procedure...write it separately
Reading File
Reading File
Reading File
Reading File
Running Command
Writing File
Writing File
Writing File
Running Command
Editing File
Running Command
Running Command
Both PDFs are ready - completely separated:
PDF 1 — SICS / MSICS only:
01 SICS MSICS
PDF Document · PDF
Contains: Overview, technique comparison table, pre-op prep, anaesthesia (topical / peribulbar / sub-Tenon's), 8 surgical steps (tunnel incision → CCC → hydrodissection → nucleus expression with vectis → Simcoe aspiration → IOL → wound closure), Kanski's Fig. 10.10 + 10.11 images, instruments table, advantages/limitations table.
PDF 2 — Phacoemulsification only:
02 Phacoemulsification
PDF Document · PDF
Contains: Overview, phacodynamics table (AFR/vacuum/surge), pump types (peristaltic/Venturi/hybrid), handpiece anatomy, OVDs (cohesive/dispersive/soft-shell), pre-op prep, 8 surgical steps (side port → corneal incision → CCC → hydrodissection → divide-and-conquer/phaco chop/stop-and-chop → cortical I/A → IOL → hydrosealing + prophylaxis), instruments table, operative complications table, Kanski's Fig. 10.12 + 10.13 images.
This is a shared conversation. Sign in to Orris to start your own chat.