second part of maxillary artery with its supplies
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a detailed account of the second part of the maxillary artery based on Gray's Anatomy for Students.
Second Part of the Maxillary Artery (Pterygoid Part)
Location / Relation
The second part is the segment of the maxillary artery that lies in relation to the lateral pterygoid muscle in the infratemporal fossa. It may pass either lateral or medial to the lower head of the lateral pterygoid. All its branches travel alongside branches of the mandibular nerve (V3).
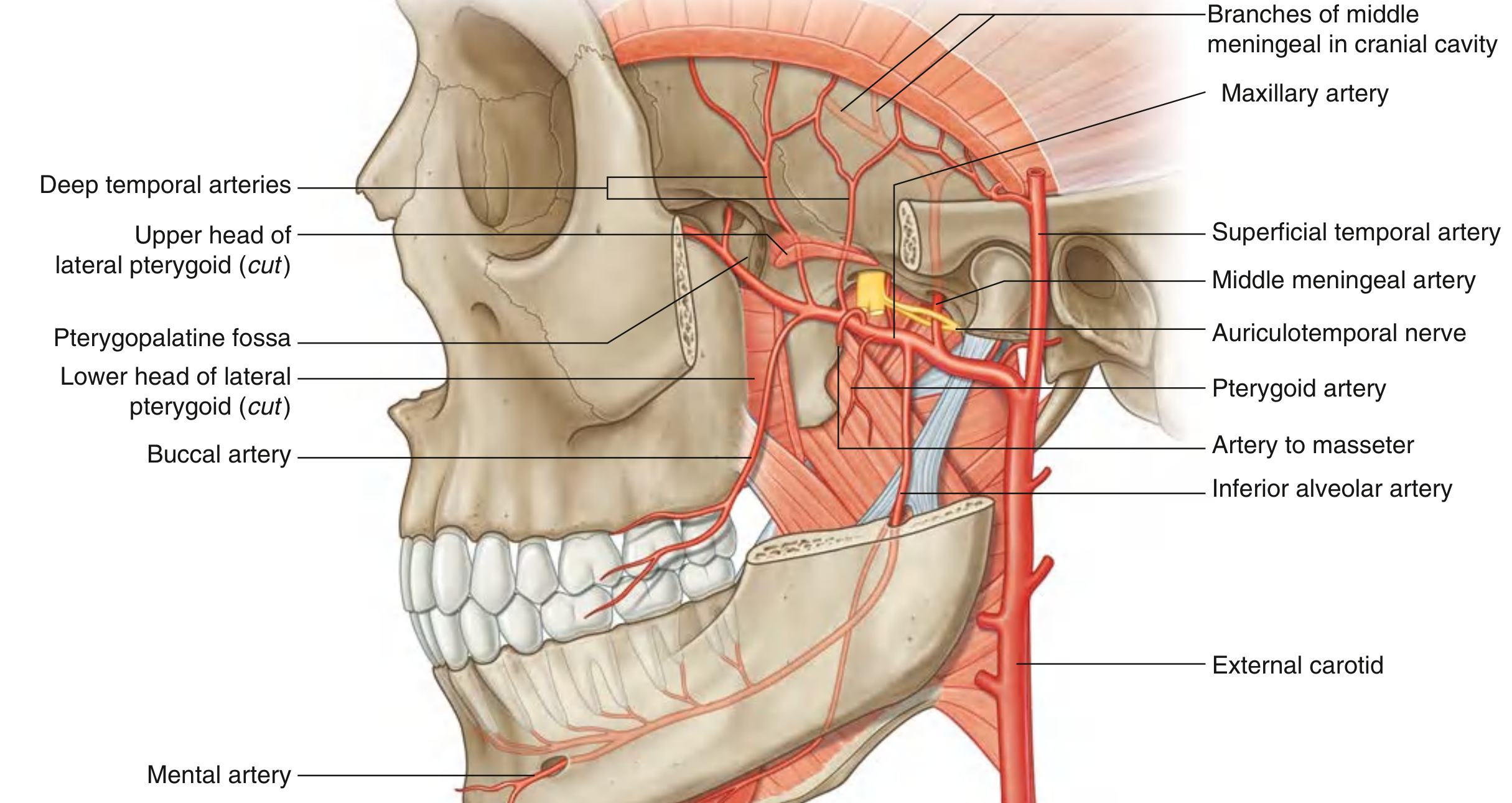
Branches and Their Supplies
The second part gives off 4 sets of branches (mnemonic: DMPB - Deep temporal, Masseteric, Pterygoid, Buccal):
| Branch | Course | Supply |
|---|---|---|
| Deep temporal arteries (anterior & posterior) | Travel with deep temporal nerves into the temporal fossa | Temporalis muscle |
| Pterygoid arteries (multiple small branches) | Directly into the pterygoid muscles | Medial and lateral pterygoid muscles |
| Masseteric artery | Accompanies the masseteric nerve laterally through the mandibular notch | Masseter muscle |
| Buccal artery | Distributed with the buccal nerve to the cheek | Skin, buccinator muscle, and oral mucosa of the cheek |
Key Points
- All branches of the second part accompany branches of V3 (mandibular nerve) - a classic exam point.
- The deep temporal arteries are usually two (anterior and posterior).
- The pterygoid arteries are numerous small vessels supplying both heads of the pterygoid muscles.
- The masseteric artery passes through the mandibular notch (sigmoid notch) to reach the masseter.
- The buccal artery is the only branch that reaches the cheek mucosa and skin.
Overview of All Three Parts (for context)
| Part | Location | Key Branches |
|---|---|---|
| 1st (Mandibular) | Between neck of mandible & sphenomandibular ligament | Middle meningeal, inferior alveolar, deep auricular, anterior tympanic, accessory meningeal |
| 2nd (Pterygoid) | Related to lateral pterygoid muscle | Deep temporal (x2), pterygoid branches, masseteric, buccal |
| 3rd (Pterygopalatine) | Pterygopalatine fossa | Posterior superior alveolar, infraorbital, descending palatine, pharyngeal, artery of pterygoid canal, sphenopalatine |
- Gray's Anatomy for Students, p. 1130
venous drainage of oral cavity
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Here is a comprehensive account of the venous drainage of the oral cavity, compiled from multiple authoritative sources.
Venous Drainage of the Oral Cavity
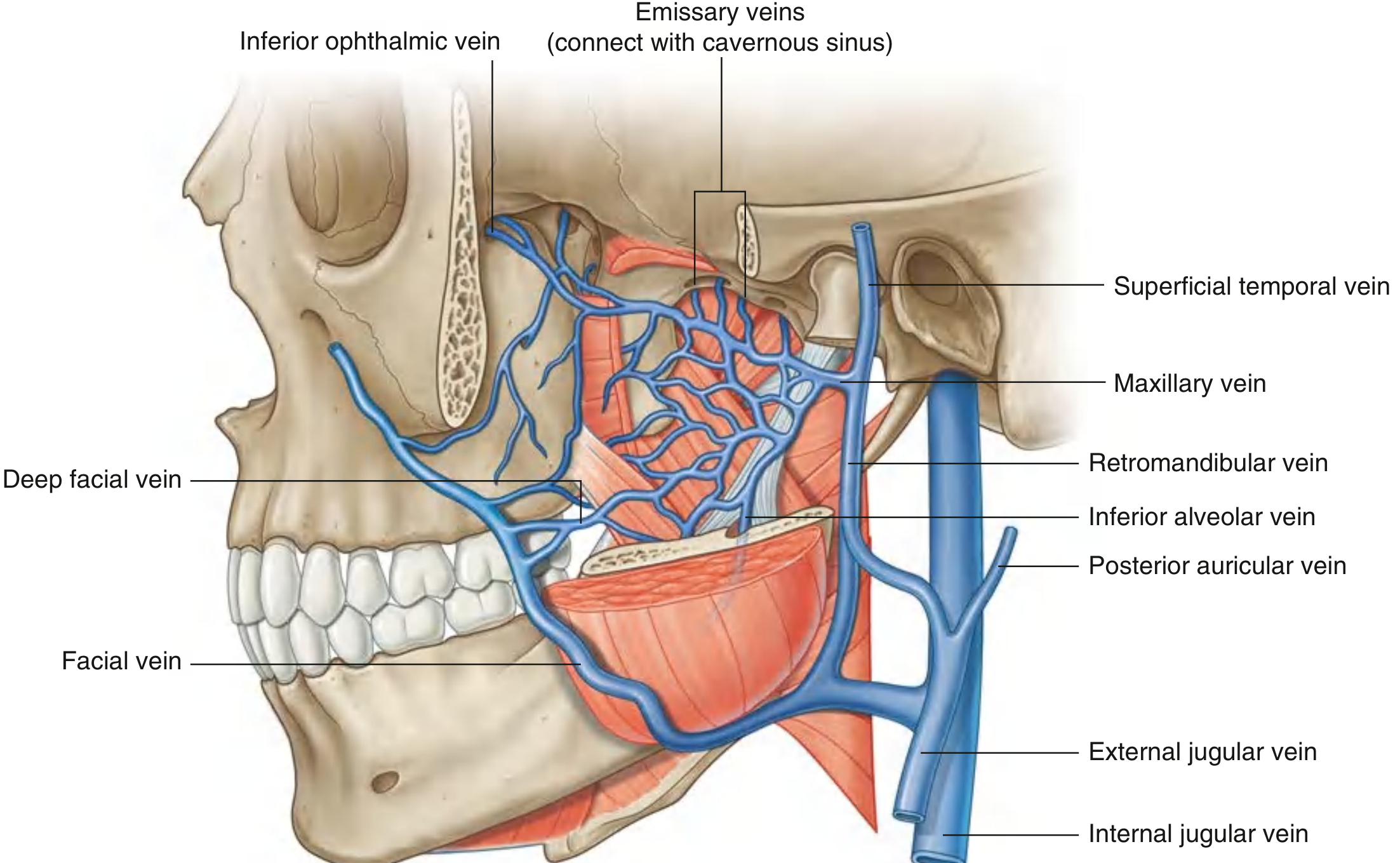
The oral cavity drains through two main channels: the lingual veins (directly into the internal jugular vein) and the pterygoid plexus (which then drains into the retromandibular/facial veins and ultimately into the internal jugular vein). The facial vein also receives direct drainage from the cheeks and lips.
1. Tongue
The tongue is drained by two sets of veins:
a) Deep lingual vein (Ranine vein)
- Begins near the apex of the tongue, visible through the mucosa on the ventral surface
- Runs posteriorly on the underside of the tongue alongside (then separated by) the hyoglossus muscle
- Accompanies the hypoglossal nerve (CN XII) on the external surface of hyoglossus - this vein is prone to injury during hypoglossal nerve dissection
- Joins a sublingual vein (from the sublingual salivary gland) to form the vena comitans nervi hypoglossi
- Drains into the internal jugular vein (or may join the lingual or facial vein first)
b) Dorsal lingual veins
- Drain the dorsum and sides of the tongue
- Follow the lingual artery between the hyoglossus and genioglossus muscles
- Drain into the internal jugular vein at the level of the hyoid bone
2. Palate, Teeth, Cheeks, and Gingiva - via Pterygoid Plexus
The pterygoid plexus is a network of veins lying between the medial and lateral pterygoid muscles (and between the lateral pterygoid and temporalis). It receives drainage from:
| Structure | Veins draining into plexus |
|---|---|
| Hard and soft palate | Palatine veins (greater palatine, nasopalatine) |
| Cheek mucosa and skin | Buccal veins |
| Upper and lower teeth | Alveolar veins |
| Roof and lateral wall of oral cavity | Corresponding venous tributaries |
| Paranasal sinuses, nasal cavity | Nasal venous tributaries |
| Mandible/lower teeth | Inferior alveolar vein |
The pterygoid plexus then connects:
- Posteriorly via a short maxillary vein into the retromandibular vein
- Anteriorly via the deep facial vein into the facial vein
The retromandibular and facial veins form a venous plexus in the submandibular triangle that drains via the common facial vein into the internal jugular vein.
3. Lips
The lips drain via labial veins into the facial vein, which descends to join the internal jugular vein.
Summary Flowchart
Tongue (deep & dorsal lingual veins)
↓
Internal Jugular Vein ←────────────────────────┐
│
Palate / Teeth / Cheeks / Gingiva │
→ Pterygoid Plexus │
↓ (posterior) ↓ (anterior) │
Maxillary Vein Deep Facial Vein │
↓ ↓ │
Retromandibular Vein → Facial Vein │
↓ │
Common Facial Vein ───────────────────────┘
Lips → Facial Vein → Common Facial Vein → Internal Jugular Vein
Clinically Important Note: Pterygoid Plexus Connections
The pterygoid plexus communicates with the cavernous sinus in the cranial cavity via small emissary veins passing through the foramen ovale, foramen lacerum, and a small sphenoidal foramen. Because the veins of the head and neck have no valves, this creates a dangerous route for:
-
Spread of dental/oral infections to the cavernous sinus (cavernous sinus thrombosis)
-
Retrograde spread of anesthetic agents injected under pressure near the pterygoid plexus
-
Gray's Anatomy for Students, p. 1131
-
Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, Ch. 41
-
Cummings Otolaryngology Head and Neck Surgery, Ch. 91
Lymphatic drainage of oral cavity detailed
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Here is a detailed, region-by-region account of the lymphatic drainage of the oral cavity.
Lymphatic Drainage of the Oral Cavity
Lymph node groups diagram (Cummings Otolaryngology):
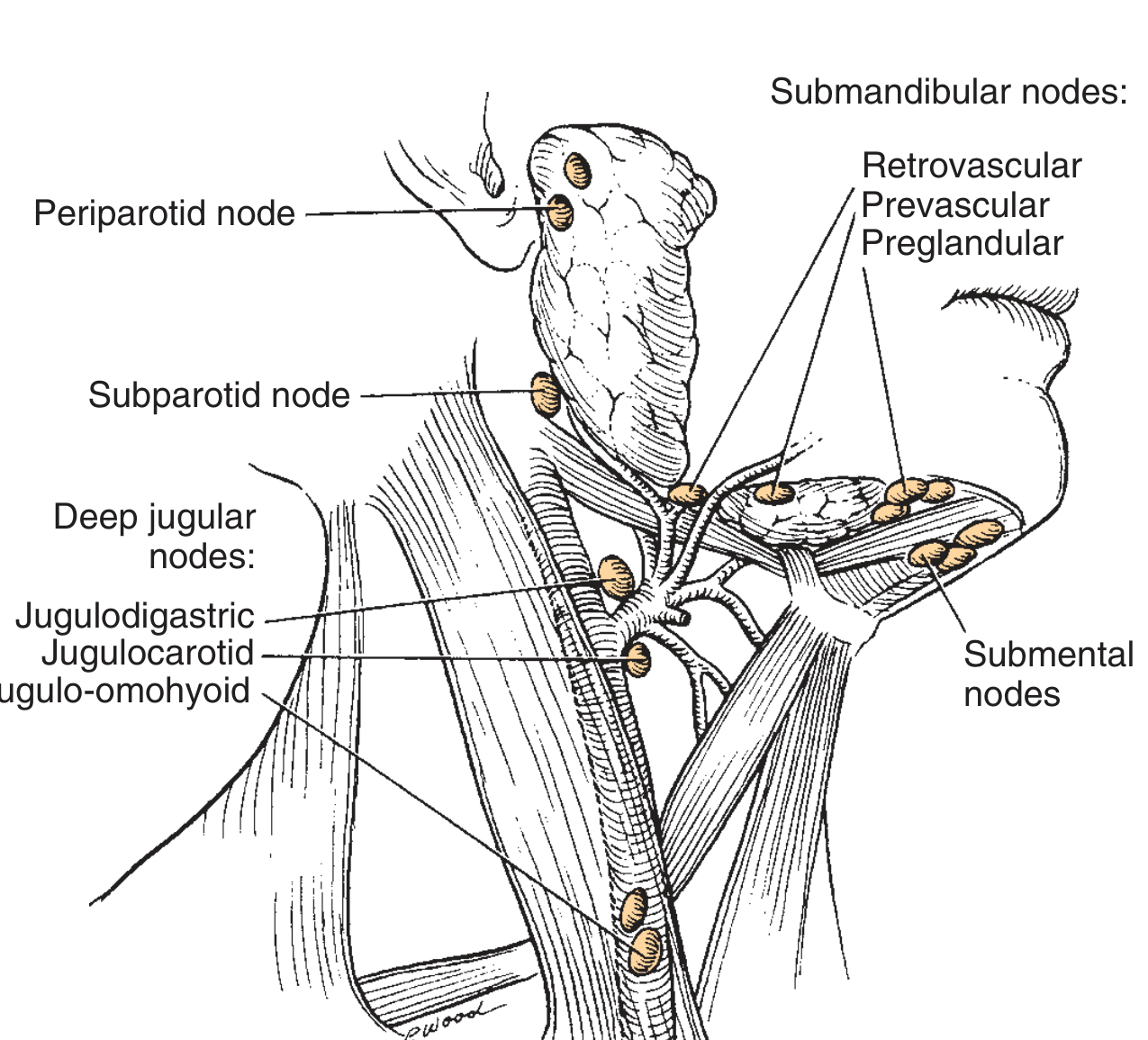
The principal node groups receiving oral cavity drainage are:
- Level Ia - Submental nodes (between anterior bellies of digastric, above hyoid)
- Level Ib - Submandibular nodes (within submandibular triangle)
- Level II - Upper deep cervical nodes (jugulodigastric = most important)
- Level III/IV - Jugulo-omohyoid nodes (at omohyoid-IJV crossing)
1. Tongue
The tongue is the most anatomically complex structure to drain and has three drainage channels - marginal, central, and dorsal.
Lymph drainage of the tongue (S Das Clinical Surgery):
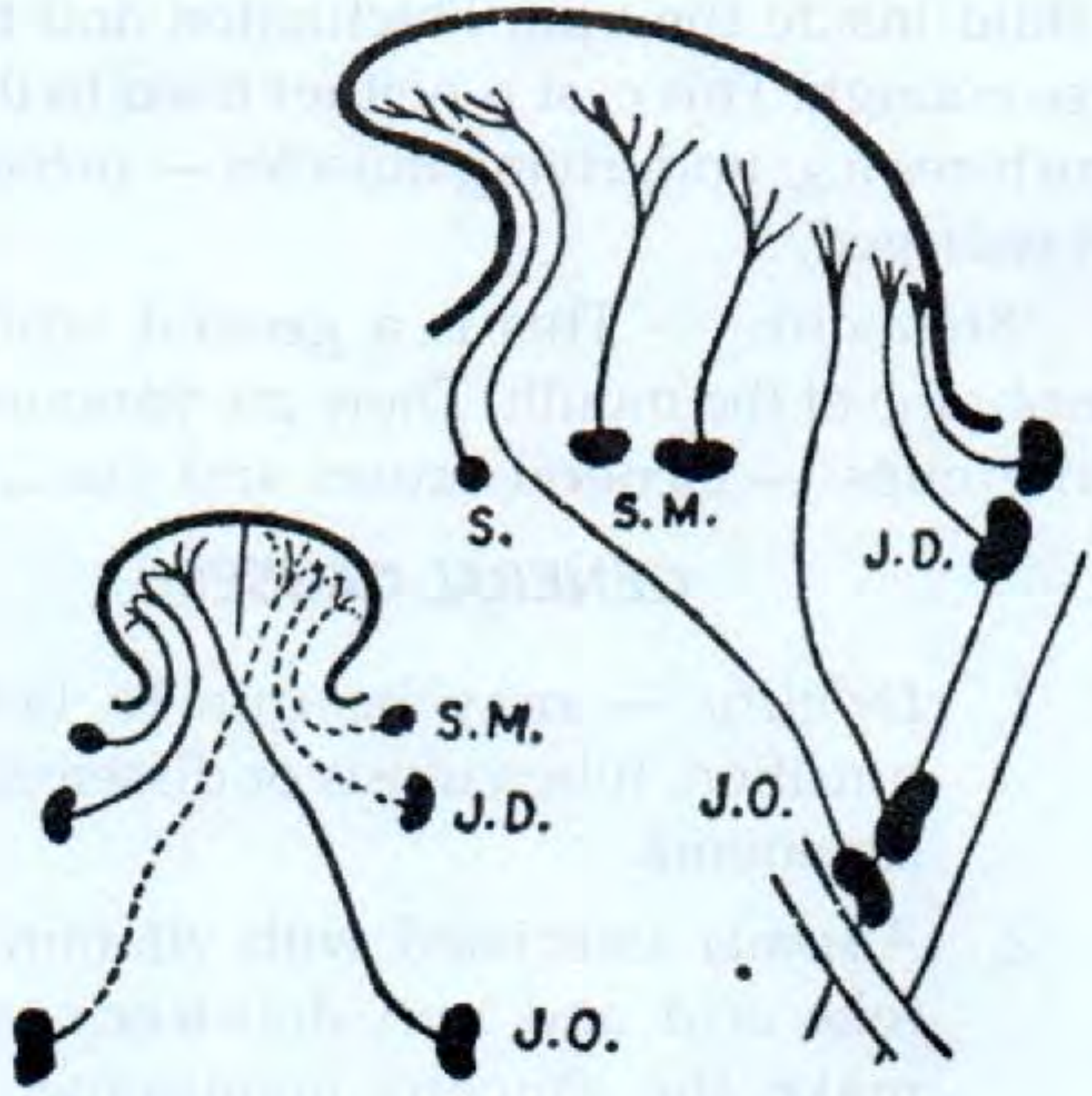
| Region | Primary drainage | Notes |
|---|---|---|
| Tip / Apex | Submental nodes (Level Ia) + Jugulo-omohyoid nodes (Level III/IV) | Vessels may cross the frenulum to drain contralaterally |
| Lateral margins (anterior) | Submandibular nodes (Level Ib) | Ipsilateral |
| Lateral margins (posterior) | Jugulodigastric nodes (Level II) | Traverse the pharyngeal wall to reach these nodes |
| Central region | Deep cervical nodes, bilaterally | Vessels may pierce mylohyoid to reach submandibular nodes |
| Dorsum (near circumvallate papillae & posterior) | Jugulodigastric + Jugulo-omohyoid nodes | Near median plane drains to either or both sides |
Key clinical point: Central tongue vessels can drain bilaterally - this means midline tongue tumours carry a risk of bilateral neck node metastasis and both sides of the neck must be examined even for unilateral lesions.
2. Floor of Mouth
| Sub-region | Drainage |
|---|---|
| Anterior floor of mouth | Submental nodes (Level Ia) - bilateral (to both left and right deep cervical chains). Lingual lymph nodes in the floor of mouth (above mylohyoid) may also be involved |
| Posterior floor of mouth | Ipsilateral upper cervical nodes (Level II) |
3. Lips
| Region | Drainage |
|---|---|
| Upper lip | Submandibular nodes (Level Ib) |
| Lateral lower lip | Submandibular nodes (Level Ib) |
| Central lower lip | Submental nodes (Level Ia) |
4. Cheeks (Buccal Mucosa)
- Drains to submental and submandibular nodes (Levels Ia and Ib)
- The buccal surface extends posteriorly to the pterygomandibular raphe; lesions in this region also tend to drain to Level Ib
5. Teeth and Gingivae
| Structure | Drainage |
|---|---|
| Most teeth | Submandibular nodes (Level Ib) - ipsilateral |
| Mandibular incisors | Submental nodes (Level Ia) |
| Mandibular molars | Occasionally directly to jugulodigastric nodes (Level II) |
| Lingual and palatal gingivae | Jugulodigastric nodes (Level II), directly or via submandibular nodes |
6. Palate
| Region | Drainage |
|---|---|
| Bulk of palate (hard palate) | Jugulodigastric nodes (Level II) + lateral retropharyngeal nodes |
| Soft palate | Upper cervical/retropharyngeal nodes |
- Venous drainage from the hard palate goes to the pterygoid plexus; lymphatics follow a separate path to upper cervical nodes
7. Final Efferent Pathway
All nodes ultimately drain into the deep cervical chain (along the internal jugular vein), then into the thoracic duct on the left and the right lymphatic duct on the right, entering the venous system at the jugulosubclavian junction.
Oral cavity structures
↓
Submental (Ia) + Submandibular (Ib) nodes
↓
Upper deep cervical - Jugulodigastric nodes (Level II)
↓
Mid/lower deep cervical - Jugulo-omohyoid nodes (Levels III/IV)
↓
Thoracic duct (left) / Right lymphatic duct (right)
↓
Venous system (jugulosubclavian angle)
Clinical Significance
- Bilateral drainage of the tongue tip, central floor of mouth, and posterior tongue means bilateral neck node dissection may be needed for midline lesions.
- The jugulodigastric node (Level II) is the first node enlarging in tonsillar, posterior tongue, and oropharyngeal malignancies - it is the sentinel node for much of the upper aerodigestive tract.
- The jugulo-omohyoid node (Level III/IV) is particularly important for anterior floor of mouth, oropharyngeal, and laryngeal drainage.
- Retropharyngeal nodes are an important skip route for hard palate tumours - these nodes are not removed in standard neck dissections and must be specifically addressed.
- Approx. 150 lymph nodes exist on each side of the neck; examination of both sides is mandatory even for clinically unilateral oral cavity lesions.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Ch. 41
- Cummings Otolaryngology Head and Neck Surgery, Ch. 91
- S Das Manual of Clinical Surgery, 13th Ed.
innervation and nerve supply for moutj
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, detailed account of the nerve supply of the mouth (oral cavity).
Nerve Supply of the Oral Cavity
Innervation of the tongue diagram - Gray's Anatomy for Students:
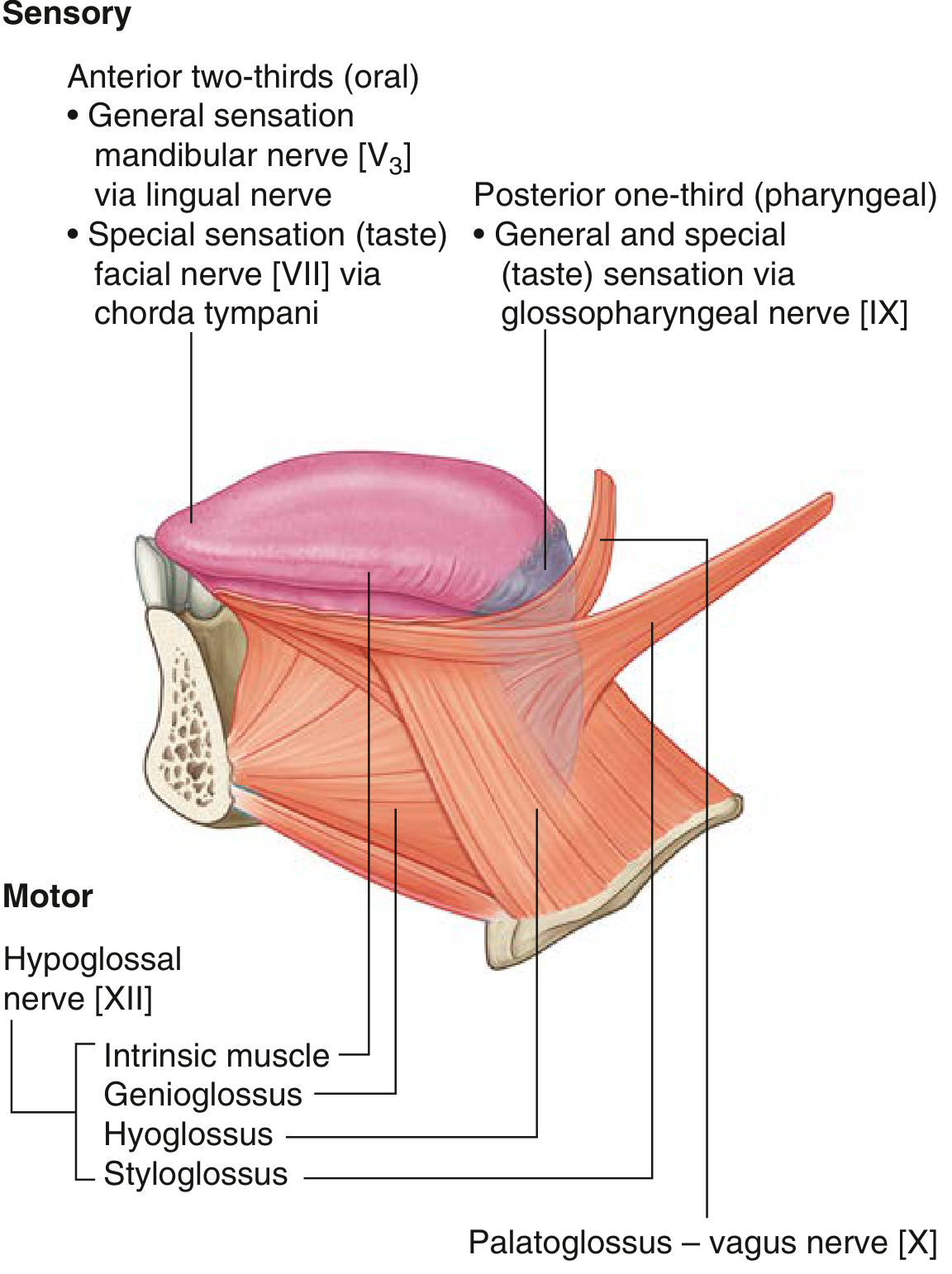
Overview
The oral cavity receives four types of nerve supply:
- General sensation (GSA) - predominantly trigeminal nerve (V2 and V3)
- Special sensation / taste (SA) - facial nerve (VII) via chorda tympani (anterior 2/3 tongue), glossopharyngeal (IX) for posterior 1/3
- Motor (GSE) - hypoglossal nerve (XII) for tongue; V3 for floor muscles; vagus (X) for soft palate
- Autonomic - parasympathetic via VII and IX; sympathetic from T1 via superior cervical ganglion
A. SENSORY (GENERAL SENSATION)
1. Maxillary Nerve (V2) - Upper Oral Cavity
| Structure | Nerve Branch | Foramen/Route |
|---|---|---|
| Hard palate (posterior to canine) | Greater palatine nerve | Descends pterygopalatine canal → exits greater palatine foramen |
| Soft palate + uvula + tonsil | Lesser palatine nerves | Exit through lesser palatine foramina |
| Anterior hard palate (behind incisors) | Nasopalatine nerve (from V2) | Enters palate via incisive foramen |
| Upper lip | Infraorbital nerve (terminal V2) | Exits infraorbital foramen |
| Upper teeth, gingiva, maxillary sinus | Posterior, middle, anterior superior alveolar nerves | From V2 / infraorbital nerve |
| Maxillary vestibule mucosa | V2 branches | - |
2. Mandibular Nerve (V3) - Lower Oral Cavity
| Structure | Nerve Branch | Route |
|---|---|---|
| Cheeks (buccal mucosa) | Buccal nerve (long buccal nerve) | Emerges between heads of lateral pterygoid → crosses buccinator |
| Floor of mouth, gums (lingual side), anterior 2/3 tongue (general sensation) | Lingual nerve | Passes through oropharyngeal triangle → loops under submandibular duct → ascends in tongue |
| Lower lip + chin | Mental nerve (terminal branch of inferior alveolar nerve) | Exits mental foramen |
| Lower teeth, gingiva | Inferior alveolar nerve | Enters mandibular foramen → traverses mandibular canal |
| Mylohyoid muscle area | Nerve to mylohyoid | Branch of inferior alveolar before entering foramen |
B. TASTE (SPECIAL SENSATION)
| Region | Nerve | Pathway |
|---|---|---|
| Anterior 2/3 of tongue | Chorda tympani (branch of facial nerve, CN VII) | Joins the lingual nerve (V3) in infratemporal fossa → travels with lingual nerve to tongue |
| Posterior 1/3 of tongue + vallate papillae | Glossopharyngeal nerve (CN IX) | Passes around stylopharyngeus, enters tongue via oropharyngeal triangle |
| Palate (taste) | Greater petrosal nerve (VII) | Via pterygopalatine ganglion → palatine nerves |
| Epiglottis / extreme posterior tongue | Vagus nerve (CN X) | Internal laryngeal branch |
Key point: The vallate papillae sit ON the sulcus terminalis - they receive taste from CN IX (not VII). CN IX branches also creep anterior to the sulcus terminalis to supply taste from these papillae.
C. MOTOR SUPPLY
Tongue Muscles - Hypoglossal Nerve (CN XII)
All intrinsic and most extrinsic tongue muscles are supplied by CN XII:
- Intrinsic muscles (superior/inferior longitudinal, transverse, vertical)
- Genioglossus (most important - tongue protrusion)
- Hyoglossus (tongue depression)
- Styloglossus (tongue retraction/elevation)
- Exception: Palatoglossus is supplied by the vagus nerve (CN X)
Floor of Mouth
- Mylohyoid and anterior belly of digastric - nerve to mylohyoid (branch of V3)
- Geniohyoid - C1 fibers traveling with CN XII
Soft Palate Muscles - Vagus Nerve (CN X) via Pharyngeal Plexus
- Levator veli palatini, palatoglossus, palatopharyngeus, musculus uvulae
- Exception: Tensor veli palatini - nerve to medial pterygoid (V3)
Lips and Cheeks - Facial Nerve (CN VII)
- All muscles of facial expression including orbicularis oris (lip sealing) and buccinator (cheek muscle) - supplied by facial nerve (CN VII)
D. AUTONOMIC SUPPLY
| Function | Nerve | Pathway |
|---|---|---|
| Parasympathetic to submandibular & sublingual glands | Chorda tympani (VII) → submandibular ganglion | Postganglionic fibers travel with lingual nerve |
| Parasympathetic to parotid gland | Lesser petrosal nerve (IX) → otic ganglion | Postganglionic fibers via auriculotemporal nerve (V3) |
| Parasympathetic to palatine glands | Greater petrosal nerve (VII) → pterygopalatine ganglion | Distributed with palatine nerves |
| Sympathetic (all glands/vessels) | T1 → superior cervical ganglion | Perivascular plexus or with trigeminal branches |
E. Summary Table by Structure
| Structure | Sensory | Taste | Motor |
|---|---|---|---|
| Tongue ant 2/3 | Lingual nerve (V3) | Chorda tympani (VII) | CN XII |
| Tongue post 1/3 | CN IX | CN IX | CN XII |
| Hard palate | Greater palatine + nasopalatine (V2) | Greater petrosal (VII) | - |
| Soft palate | Lesser palatine (V2) | - | Vagus (X); tensor: V3 |
| Cheeks | Long buccal nerve (V3) | - | Facial (VII) |
| Upper lip | Infraorbital (V2) | - | Facial (VII) |
| Lower lip | Mental nerve (V3) | - | Facial (VII) |
| Upper teeth | Superior alveolar nerves (V2) | - | - |
| Lower teeth | Inferior alveolar nerve (V3) | - | - |
| Floor of mouth | Lingual nerve (V3) | - | Nerve to mylohyoid (V3) |
| Pillars of fauces | CN IX | - | Vagus (X) |
Clinical Notes
-
The lingual nerve passes medial to the lower third molar - at risk during wisdom tooth extraction, causing loss of anterior 2/3 tongue sensation
-
Chorda tympani injury (in middle ear surgery or parotid surgery) causes loss of taste from anterior 2/3 tongue + reduced submandibular/sublingual salivation
-
CN XII palsy causes tongue deviation toward the side of the lesion (ipsilateral genioglossus paralysis)
-
Referred otalgia (ear pain) from oral cavity lesions is via CN IX (posterior tongue/tonsil → tympanic branch of IX → ear)
-
Gray's Anatomy for Students, p. 1240
-
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Ch. 41
-
Cummings Otolaryngology Head and Neck Surgery, Ch. 91
1st part of maxillary artery
Finding Sources
Reading File
Reading File
Reading File
Loading Image
First Part of the Maxillary Artery (Mandibular Part)
Location / Relations
The first (mandibular) part runs horizontally between the neck of the mandible medially and the sphenomandibular ligament laterally, within the parotid gland substance. This is the segment before the artery enters the infratemporal fossa proper.
Branches
The first part gives 2 major branches + 3 small branches (mnemonic: DAAMI - Deep auricular, Anterior tympanic, Accessory meningeal, Middle meningeal, Inferior alveolar):
Major Branches
1. Middle Meningeal Artery
- Ascends vertically from the maxillary artery
- In the infratemporal fossa, passes superiorly between the sphenomandibular ligament (medially) and lateral pterygoid muscle (laterally)
- Passes between the two roots of the auriculotemporal nerve just below the foramen spinosum (classic exam point)
- Enters the cranial cavity through the foramen spinosum
- Inside the skull it runs in the periosteal (outer) layer of dura mater
- Divides into a frontal (anterior) branch and a parietal (posterior) branch
- Is the largest meningeal vessel - supplies most of the dura mater, cranial bone, and bone marrow of the calvaria
- Clinical: Rupture of the anterior branch by a temporal blow causes an extradural (epidural) hematoma - blood collects between dura and inner table of skull, causing a lucid interval then rapid deterioration
2. Inferior Alveolar Artery
- Descends from the maxillary artery
- Before entering the mandible, gives off a mylohyoid branch (accompanies the nerve to mylohyoid in the mylohyoid groove)
- Enters the mandibular canal through the mandibular foramen alongside the inferior alveolar nerve
- Inside the canal it supplies all lower teeth, mandibular bone, and buccal gingivae
- Terminates as two branches:
- Incisive branch - continues forward to supply incisor teeth
- Mental artery - exits through the mental foramen to supply chin, lower lip, and labial gingiva
Minor Branches (3 small branches)
| Branch | Foramen / Route | Supply |
|---|---|---|
| Deep auricular artery | Pierces cartilage or bone of external acoustic meatus | Skin of external acoustic meatus (EAM), anterior wall of EAM, outer surface of tympanic membrane, temporomandibular joint |
| Anterior tympanic artery | Passes through petrotympanic fissure | Deep (inner) surface of tympanic membrane + tympanic cavity |
| Accessory meningeal artery | Passes through foramen ovale into cranial cavity | Dura mater (supplementing middle meningeal artery); also gives small branches to pterygoid muscles in infratemporal fossa before ascending |
Summary Table
| Branch | Route | Supply |
|---|---|---|
| Middle meningeal | Foramen spinosum | Dura mater, cranial bone, bone marrow |
| Inferior alveolar | Mandibular foramen → mandibular canal | All lower teeth, mandibular bone, chin, lower lip |
| - Mylohyoid branch | Mylohyoid groove | Mylohyoid muscle |
| - Mental branch (terminal) | Mental foramen | Chin, lower lip |
| Deep auricular | Pierces EAM cartilage/bone | EAM skin, outer TM, TMJ |
| Anterior tympanic | Petrotympanic fissure | Tympanic cavity, inner TM |
| Accessory meningeal | Foramen ovale | Dura mater + pterygoid muscles |
Clinical Importance
-
Extradural hematoma - the anterior (frontal) branch of the middle meningeal artery runs in a groove on the inner surface of the temporal bone (pterion - thinnest part of skull). A blow here fractures the bone and tears the artery, causing a classic presentation: brief loss of consciousness → lucid interval → rapid deterioration as blood under arterial pressure strips dura from bone.
-
The inferior alveolar nerve block (dental anaesthesia) targets the inferior alveolar nerve near the mandibular foramen; the artery accompanies the nerve at this point and inadvertent intravascular injection is possible.
-
The accessory meningeal artery provides an important collateral meningeal supply and also communicates with orbital and ophthalmic vessels.
-
Gray's Anatomy for Students, p. 1130
-
Color Atlas of Human Anatomy Vol. 2, p. 97
This is a shared conversation. Sign in to Orris to start your own chat.