chest ap and pa radiography
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Here is a detailed guide on chest AP and PA radiography:
Chest Radiography: AP vs. PA Projections
1. The Two Standard Projections
Posteroanterior (PA) - The Standard View
The PA chest radiograph is the gold standard projection for chest imaging in ambulatory patients. The X-ray beam travels from posterior to anterior - the patient stands erect facing the detector, with the anterior chest wall pressed against it.
Technical parameters:
- Focal spot-to-film distance: 72 inches (183 cm) - this long distance minimizes magnification
- kVp: ~120-130 kVp (higher energy reduces motion blur and improves vascular detail)
- Position: Patient erect, full inspiration, breath held
- Scapulae: Rotated forward and out of the lung fields by placing hands on hips and rolling shoulders forward
Why PA is preferred:
- The heart and anterior mediastinal structures are close to the detector, so they are minimally magnified
- Accurate cardiothoracic ratio (CTR) assessment is only reliable on an erect PA film
- Normal CTR on PA: less than 0.5 (heart width < half of thoracic width)
Anteroposterior (AP) - The Portable/Supine View
The AP projection is used when the patient cannot stand - ICU patients, trauma cases, post-operative patients, or any bedside/portable situation. The beam travels anterior to posterior; the detector is placed behind the patient.
Technical parameters:
- Focal spot-to-film distance: typically 40 inches (portable units)
- kVp: ~100 kVp (lower energy, shorter exposure distance)
- Position: Supine or semi-recumbent (erect AP if possible)
Limitations of AP compared to PA:
| Feature | PA (Standard) | AP (Portable) |
|---|---|---|
| Cardiac size | True size, accurate CTR | Magnified - appears larger |
| Mediastinum | Normal width | Appears wider (false widening) |
| Lung detail | Excellent | Reduced (motion blur, magnification) |
| Vascular detail | Good | Poor at 40" FFD |
| Scapular overlap | Minimal | Scapulae overlie lung fields |
| Pleural effusion | Fluid meniscus visible | May appear as diffuse haziness only |
The image below from Murray & Nadel demonstrates this difference directly:
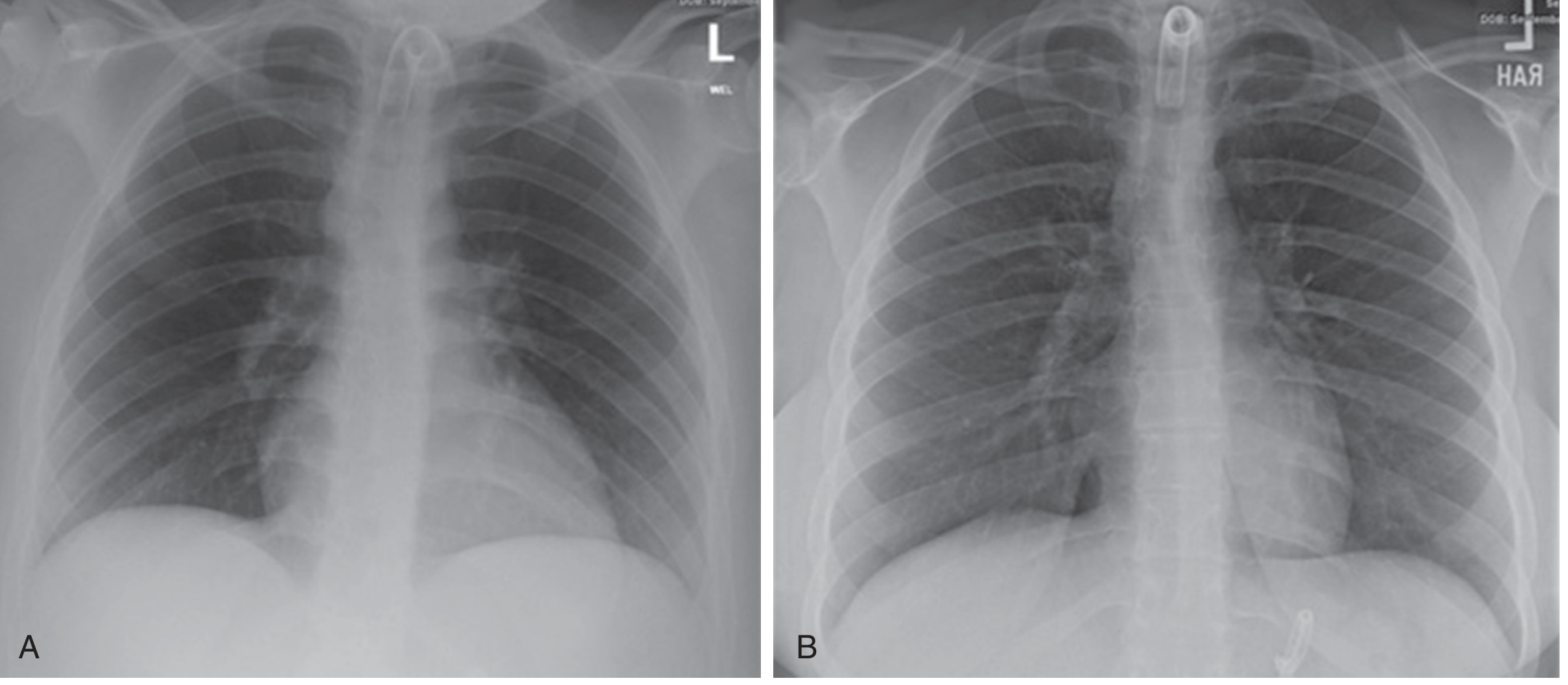
Image A: AP supine portable ICU radiograph (100 kVp, 40" FFD) - poor vascular detail and magnification. Image B: Same patient in the radiology department (130 kVp, 72" FFD) - far superior detail with less magnification. - Murray & Nadel's Textbook of Respiratory Medicine
2. Assessing Radiographic Quality (RIPE)
Before interpreting any chest film, assess technical quality using the RIPE criteria:
R - Rotation
- The medial ends of the clavicles should be equidistant from the spinous processes of the vertebrae
- Rotation causes apparent mediastinal widening and asymmetric lung density
I - Inspiration
- Adequate inspiration: the anterior end of the 6th rib (or posterior end of the 10th rib) should intersect the right hemidiaphragm at the midclavicular line
- Poor inspiration elevates the diaphragm, crowding the lung bases and exaggerating cardiomegaly
P - Projection
- Identify whether AP or PA - an AP label is usually present; if not, look for magnification of the heart or scapular overlap over the lungs
E - Exposure
- On a correctly exposed film, the thoracic vertebrae should be faintly visible through the cardiac shadow
- Overexposure: lung fields appear too dark; interstitial markings may be lost
- Underexposure: lungs appear too white; fat pads at the cardiophrenic angles may be misread as cardiomegaly
3. Systematic Interpretation - Structures to Evaluate
Trachea and Mediastinum
- Trachea: midline or slightly right of center above the carina
- Tracheal deviation away from pathology: tension pneumothorax, large pleural effusion
- Tracheal deviation toward pathology: lung collapse, post-pneumonectomy fibrosis
- Carina angle: normally <70 degrees; widening suggests left atrial enlargement
Heart and Cardiac Borders
- Right heart border: right atrium (lower), superior vena cava (upper)
- Left heart border: aortic knuckle (top), pulmonary trunk, left atrial appendage, left ventricle (lower)
- Cardiothoracic ratio: reliably assessed only on erect PA; ratio >0.5 suggests cardiomegaly (but see AP caveats above)
On the PA radiograph: "The heart is best evaluated on posteroanterior (PA) and lateral radiographs, with the heart closest to the image detector. On the chest radiograph, the heart appears as a homogeneous shadow." - Goldman-Cecil Medicine
Hila
- Left hilum is normally 0.5-1.5 cm higher than the right
- Hilar enlargement: lymphadenopathy, pulmonary artery dilation
- Hilar depression: ipsilateral lower lobe collapse
Lung Fields
Evaluate in zones (upper, mid, lower) and compare sides. Look for:
- Consolidation: airspace opacification that respects lobar boundaries; air bronchograms may be visible
- Collapse: loss of volume + shift of fissures, mediastinum, or diaphragm
- Nodules/masses
- Pneumothorax: absence of lung markings peripheral to a visible pleural line
Pleural Spaces
- Free pleural fluid: on an upright PA, 200-250 mL minimum is needed to see blunting of the lateral costophrenic angle
- A lateral radiograph may detect as little as 50-75 mL
- Classic meniscus: concave upper border, higher laterally than medially
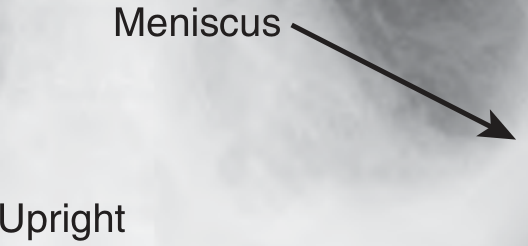
Upright PA radiograph showing the characteristic meniscus of a pleural effusion at the costophrenic angle. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
On a supine AP film, pleural effusion is far harder to detect - it spreads as a layer posteriorly and may only show as diffuse hemithorax haziness, apical capping, or obliteration of the hemidiaphragm. Up to 500 mL can be missed.
Diaphragm
- Right hemidiaphragm is normally higher than the left by ~15 mm (up to 30 mm is acceptable)
- Normal level: anterior end of the 5th or 6th rib interspace at the midlung field
- Flattening: emphysema, acute severe asthma
- Unilateral elevation: phrenic nerve palsy, adjacent pulmonary/pleural/subphrenic disease
- Bilateral elevation: supine position, poor inspiration, obesity, pregnancy, ascites
On the PA film: "Each hemidiaphragm is normally represented by a smooth, curved line which is convex upwards. The lateral attachment to the ribs forms the costophrenic recess, a sharply defined acute angle." - Grainger & Allison's Diagnostic Radiology
Bones and Soft Tissues
- Ribs: count carefully for fractures; first and second rib fractures suggest major force and raise concern for aortic injury
- Clavicles, scapulae, vertebrae
- Soft tissues: surgical emphysema, masses, breast shadows
4. AP-Specific Pitfalls in Trauma and the ICU
From Bailey & Love's Surgery and Rosen's Emergency Medicine:
- Mediastinal widening on AP/supine does not necessarily indicate aortic injury - portable AP magnification and patient positioning routinely produce a wider-appearing mediastinum. Always try to get an erect PA before declaring the mediastinum abnormal.
- Haemothorax on supine AP appears as a homogeneous increase in opacity of the hemitorax - be careful not to confuse the haemothorax (less radiolucent) with a pneumothorax (more radiolucent); look carefully for lung markings.
- Pneumothorax is best seen on an erect PA or lateral decubitus; on a supine AP, air rises anteriorly and may be invisible at the apex - look for deep sulcus sign instead.
- Up to 300 mL of blood may pool behind the diaphragm and may not be visible even on an erect view.
5. Summary Comparison
| Parameter | PA Chest | AP Chest |
|---|---|---|
| Beam direction | Posterior → Anterior | Anterior → Posterior |
| Patient position | Erect, standing | Supine or sitting |
| FFD | 72 inches | ~40 inches |
| Heart magnification | Minimal (true size) | Significant (overestimates) |
| Cardiac assessment | Reliable CTR | Unreliable CTR |
| Pleural fluid detection | 200-250 mL threshold | Poorly sensitive |
| Lung detail | Superior | Inferior |
| Scapulae | Outside lung fields | Overlap lung fields |
| Clinical use | Outpatient, elective | ICU, trauma, bedside |
Sources: Grainger & Allison's Diagnostic Radiology | Murray & Nadel's Textbook of Respiratory Medicine | Rosen's Emergency Medicine | Roberts and Hedges' Clinical Procedures in Emergency | Bailey and Love's Short Practice of Surgery | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.