Types of knee pain osteoarthritis differential diagnosis over medial , lateral joint line and below medial joint line
Reading File
Finding Sources
Finding Sources
Searching the Web
knee pain differential diagnosis medial lateral joint line below medial joint line osteoarthritis
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
knee pain differential diagnosis medial lateral joint line below medial
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data. Let me compile the full answer.
Knee Pain: Differential Diagnosis by Location
The knee is best examined with the patient's knee flexed to 90 degrees. Precise localization of tenderness is the single most important step in narrowing the differential. Below is a systematic breakdown by anatomical zone.
OVER THE MEDIAL JOINT LINE
Tenderness directly at the medial joint line points to two principal diagnoses, plus several less common ones.
1. Medial Meniscus Tear
The most common and important cause of medial joint line tenderness. Key features:
- History of a twisting mechanism (acute) or insidious onset in older patients (degenerative tear)
- Localized tenderness directly over the medial joint line
- McMurray test, Thessaly test, or Apley grind test may be positive
- Mild effusion often present; quadriceps (VMO) wasting in chronic cases
- Sensation of locking, catching, or giving way
- MRI is the investigation of choice
"Localized tenderness along the medial or lateral joint line or over the periphery of the meniscus is the most important physical finding." - Campbell's Operative Orthopaedics, 15th Ed.
2. Osteoarthritis (Medial Compartment)
- Most commonly affects the medial compartment of the knee
- Diffuse medial joint line tenderness, crepitus, bony enlargement
- Varus deformity (bow-legged) as medial cartilage wears
- Weight-bearing X-ray shows medial joint space narrowing, osteophytes, subchondral sclerosis
- No acute effusion (unless inflammatory flare)
3. Medial Collateral Ligament (MCL) Sprain
- History of valgus stress (e.g., direct blow to lateral knee)
- Tenderness at the femoral attachment of the MCL (above joint line) or along its course at the joint line
- Pain reproduced by valgus stress testing at 30° flexion
- Grade I/II: intact endpoint; Grade III: no endpoint (complete rupture)
"In lesion of the medial collateral ligament, tenderness is characteristically present at its femoral attachment." - S Das Manual on Clinical Surgery, 13th Ed.
4. Medial Plica Syndrome
- Often overlooked; plica = redundant medial synovial fold
- Tender, mobile, cord-like nodularity just anterior to the medial joint line
- Onset after increase in activity (overuse)
- No effusion; X-rays normal
- Diagnosis confirmed by arthroscopy
OVER THE LATERAL JOINT LINE
1. Lateral Meniscus Tear
- Same mechanism as medial: twisting injury or degenerative
- Localized tenderness over the lateral joint line - palpate just lateral to the inferior patellar pole with knee at 90°
- McMurray test positive with external rotation stress
- Lateral meniscal cysts (ganglion) can form here - visible as a firm swelling at lateral joint line
2. Osteoarthritis (Lateral Compartment)
- Less common than medial compartment OA
- Valgus deformity (knock-knee)
- Lateral joint line tenderness, crepitus, restricted range of motion
3. Lateral Collateral Ligament (LCL) Sprain
- Less common than MCL injury
- Result of varus stress (e.g., planting foot and turning toward ipsilateral side)
- Point tenderness at the lateral joint line (fibular head attachment)
- Pain on varus stress testing at 30° flexion
- May be associated with posterolateral corner injury
4. Iliotibial Band (ITB) Syndrome
- Overuse injury in runners and cyclists - repetitive knee flexion
- Pain and tenderness at the lateral femoral condyle (where ITB crosses), typically at 30° flexion ("impingement zone")
- Reproduced after reaching a certain mileage threshold
- Noble compression test positive
- No effusion
"Iliotibial band syndrome manifests by lateral knee pain caused by repetitive stress between the iliotibial band and the lateral femoral condyle." - Goldman-Cecil Medicine
5. Popliteus Tendinitis
- Posterior-lateral knee pain, worse running downhill
- Tenderness along the lateral joint line (posterior portion) or at proximal posterior tibia insertion
- Webb test: pain on resisted external rotation with knee at 90°
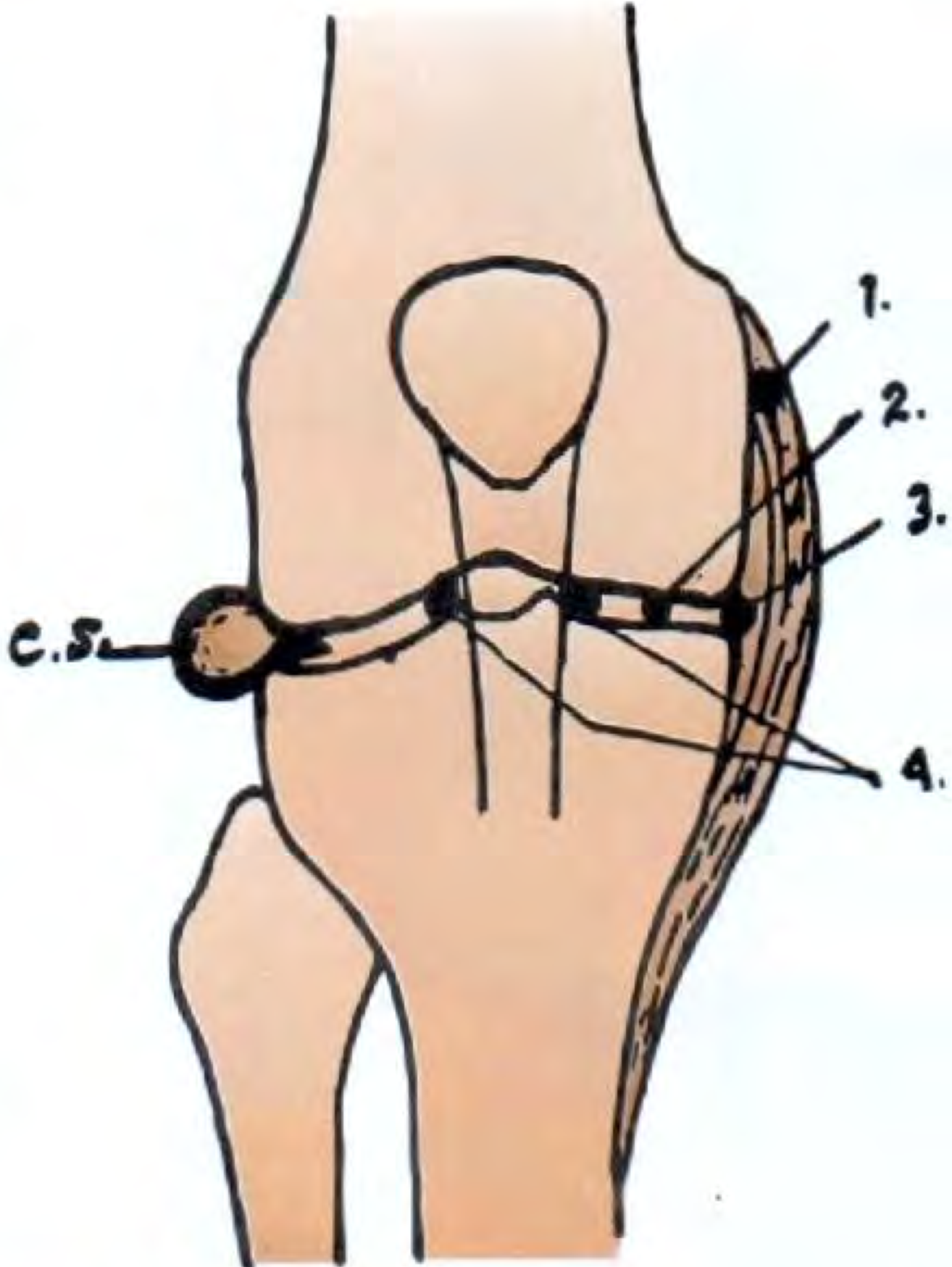
Points of tenderness (S Das, Manual on Clinical Surgery): 1 = MCL sprain (above joint line at femoral attachment), 2 = medial meniscus injury (at joint line), 3 = deep MCL fibers + meniscus (joint line), 4 = infrapatellar fat pad. C.S. = lateral meniscal cyst.
BELOW THE MEDIAL JOINT LINE
This is the zone most often confused with medial compartment OA, and getting this distinction right changes management entirely.
1. Pes Anserine Bursitis / Pes Anserinus Pain Syndrome (PAPS)
The key diagnosis in this zone.
The pes anserine bursa lies deep to the three conjoined tendons (sartorius, gracilis, semitendinosus - "SGT") inserting on the medial tibia, ~2-3 cm below the joint line, superficial to the MCL.
Clinical features:
- Pain and focal tenderness ~2-3 cm distal to the medial joint line (not at the joint line itself)
- Occasional local swelling over the bursa
- Worsened by stair climbing, getting up from a chair, repetitive flexion/extension
- Valgus stress testing or resisted knee flexion may reproduce pain
- No knee joint effusion (distinguishes it from intra-articular pathology)
High-risk profile: Obese women with knee OA + diabetes mellitus. This is a frequent co-morbidity in patients who already carry a diagnosis of knee OA, and the bursitis pain is often mistakenly attributed to the OA itself.
"Pes anserine bursitis is common in obese women with osteoarthritis of the knee, in runners, and with other various overuse syndromes. The patient complains of anterior medial pain below the joint line." - Tintinalli's Emergency Medicine
"Patients with anserine bursitis usually complain of medial knee pain approximately 2 or 3 cm distal to the joint line. Risk factors include osteoarthritis of the knee, diabetes mellitus, and possibly obesity." - Rosen's Emergency Medicine
2. MCL Distal Attachment Injury
- The MCL inserts distally on the medial tibia below the joint line
- Tenderness here indicates injury to the distal MCL or combined menisco-ligamentous injury
- Valgus stress testing is positive
3. Medial Tibial Stress Fracture / Medial Tibial Stress Syndrome (MTSS)
- Diffuse tenderness over the medial tibia below the joint line (not focal at the joint line)
- Common in runners; associated with a recent increase in training load
- X-ray may be normal early; bone scan or MRI is sensitive
4. Saphenous Nerve Entrapment
- Pain and paresthesia along the medial knee and leg
- Aggravated by knee extension, relieved by flexion
Summary Table
| Location | Top Diagnoses | Key Distinguishing Feature |
|---|---|---|
| Medial joint line | Medial meniscus tear, Medial OA, MCL sprain, Medial plica | McMurray test; MRI for meniscus; valgus stress for MCL |
| Lateral joint line | Lateral meniscus tear, Lateral OA, LCL sprain, ITB syndrome, Popliteus tendinitis | McMurray; Noble test; varus stress |
| Below medial joint line | Pes anserine bursitis, Distal MCL injury, MTSS | Tenderness 2-3 cm below joint line; no effusion; OA + DM + obesity risk profile |
Clinical Pearl: OA vs. Pes Anserine Bursitis
These two conditions commonly coexist and are frequently confused. The distinction:
- OA: tenderness at the joint line, crepitus, bony enlargement, X-ray changes, joint effusion
- Pes anserine bursitis: tenderness 2-3 cm below the joint line, no effusion, local bursal swelling, responds to local corticosteroid injection
A patient with known knee OA who reports nocturnal pain waking them from sleep, especially with inner-thigh discomfort, should be assessed specifically for pes anserine bursitis - it is a treatable condition that will not respond to OA management.
Sources: Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Campbell's Operative Orthopaedics 15th Ed (2026); S Das Manual on Clinical Surgery 13th Ed; Miller's Review of Orthopaedics 9th Ed; Goldman-Cecil Medicine; AAFP Knee Pain Differential
If pes ansernius bursitis Give detailed treatment protocol
Reading File
Finding Sources
Finding Sources
Searching PubMed
pes anserine bursitis treatment
Searching the Web
pes anserine bursitis treatment protocol corticosteroid injection physical therapy 2023 2024
Reading File
Reading File
Finding Sources
Reading Web Page
pes anserine bursitis treatment corticosteroid PRP shockwave results
Finding Sources
Finding Sources
Reading File
Searching PubMed
pes anserinus bursitis corticosteroid injection ultrasound guided
I have comprehensive data from authoritative textbooks and recent RCTs. Here is the full detailed treatment protocol:
Pes Anserine Bursitis (PAPS): Detailed Treatment Protocol
STEP 0 - Confirm Diagnosis Before Treating
Before initiating treatment, exclude mimics:
- Septic bursitis - fever, overlying erythema/warmth, leukocytosis - requires aspiration + antibiotics (not steroid injection)
- Medial meniscus tear / medial compartment OA - tenderness at the joint line (not below it)
- MCL injury - tenderness at ligament, valgus instability
- Stress fracture / MTSS - diffuse tibial tenderness, history of increased training load
- Underlying crystal disease (gout, pseudogout) - treat the crystals, not just the bursa
If any doubt - aspirate first, send fluid for WBC, crystals, culture.
Bursal fluid WBC >5000/µL suggests infection even with negative Gram stain. - Rosen's Emergency Medicine
PHASE 1 - Immediate / Acute Management (Days 1-14)
1. Activity Modification (Rest)
- Relative rest - avoid stairs, squatting, incline walking, and repetitive knee flexion activities
- Continue gentle, non-loading activity (swimming, cycling on a flat surface if tolerated)
- Do NOT immobilize completely - this reduces collagen production and delays healing
2. Ice / Cryotherapy
- Ice pack to the medial proximal tibia (NOT the joint line)
- 15-20 minutes, 3-4 times per day
- Wrap in cloth - never apply ice directly to skin
- Continue for the first 1-2 weeks, especially after activity
3. NSAIDs (First-line oral pharmacotherapy)
| Drug | Dose | Duration |
|---|---|---|
| Ibuprofen | 400-600 mg TDS with food | 2 weeks |
| Naproxen | 500 mg BD with food | 2 weeks |
| Diclofenac | 50 mg TDS or 75 mg SR BD | 2 weeks |
| Celecoxib (COX-2, preferred in elderly/OA with GI risk) | 100-200 mg OD/BD | 2-3 weeks |
- Add PPI (omeprazole 20 mg) if >65 years, co-existing OA on long-term NSAIDs, or history of peptic disease
- In diabetics: NSAIDs may mask symptoms; monitor more closely
- In CKD: use with caution; prefer topical diclofenac gel locally
4. Topical Anti-inflammatories
- Diclofenac 1% gel applied over the pes anserine area 3-4x daily
- Effective adjunct, especially in elderly patients to minimize systemic NSAID exposure
5. Compression
- Knee sleeve or elastic bandage to reduce bursal swelling
- Avoids fluid re-accumulation
PHASE 2 - Interventional Treatment (If Phase 1 Fails at 2-4 Weeks, or Severe Presentation)
Corticosteroid Injection - First-Line Intervention
Indication: Failure of 2 weeks of conservative therapy, or severe pain limiting function from day 1.
Agent and dose:
- Triamcinolone acetonide 20-40 mg + 2-3 mL of 1% lidocaine (or 0.5% bupivacaine for longer analgesia)
- Alternative: Methylprednisolone acetate 40 mg
Technique (Landmark-guided):
"Position the patient with the knee flexed 90 degrees. Using an anterior or medial approach with a 2.5- to 3.9-cm, 22-gauge needle, identify the point of greatest tenderness and gently advance the needle until the tibia is reached. Withdraw the needle 2-3 mm and inject 2-4 mL of lidocaine along with approximately 20-40 mg of a corticosteroid suspension." - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Step-by-step:
- Patient supine, knee flexed at 90 degrees
- Identify the point of maximum tenderness (~2-4 cm below the medial joint line, just posterior to the tibial crest)
- Clean skin with antiseptic
- Insert 22-gauge, 1.5-inch (3.8 cm) needle perpendicular to the tibia
- Advance until bony contact with tibia
- Withdraw 2-3 mm (to avoid periosteal injection)
- Aspirate - if fluid present, drain first; if bloody/purulent, send for analysis before injecting steroid
- Inject the lidocaine-steroid mixture using a fan technique if needed
- Do NOT inject directly into the tendon - risk of tendon rupture
Ultrasound guidance is now preferred over landmark technique:
- Increases accuracy of needle placement into the bursa
- A 2024 multicenter RCT (Babaei-Ghazani et al., PMID 37752656) confirmed superiority of US-guided over blind injection
- Particularly helpful in obese patients where anatomical landmarks are obscured
Expected response: Prompt symptomatic relief within 24-72 hours. Duration of benefit is variable and correlates with the patient's weight-bearing activity level.
Maximum injections: Up to 3 injections in a 12-month period at this site. Space injections at least 6-8 weeks apart.
PHASE 3 - Physical Therapy & Rehabilitation (Weeks 2-8, run concurrently with Phase 1/2)
Physical therapy is equally effective as corticosteroid injection in clinical trials (both show significant VAS and WOMAC improvement at 8 weeks with no statistically significant difference between groups).
A. Stretching Program
Hamstring stretching (most important):
- Supine straight-leg raise stretch, hold 30 seconds x 3 repetitions
- Standing hamstring stretch against a wall
- 2x daily
Hip adductor / gracilis stretch:
- Butterfly stretch (seated, soles together, lean forward)
- Hold 30 seconds x 3 reps, 2x daily
- Targets the gracilis component of pes anserine
Calf and gastrocnemius stretch:
- Wall calf stretch, knee straight then knee bent
- 30 seconds x 3 reps
B. Strengthening Program (start after acute pain settles, typically week 2-3)
Quadriceps strengthening (reduces valgus load on medial compartment):
- Straight-leg raises: 3 sets x 15 reps
- Terminal knee extensions with resistance band
- Quad sets (isometric)
Hip abductor strengthening (reduces dynamic valgus):
- Side-lying hip abduction: 3 sets x 15 reps
- Clamshell exercises with resistance band
- This is often under-emphasized - weak hip abductors increase medial knee stress
Gradual return to full weight-bearing activities over 4-6 weeks
C. Physiotherapy Modalities
- Ultrasound therapy (therapeutic)
- TENS / interferential therapy for pain relief
- Kinesiotaping - evidence suggests kinesiotaping may be comparable to NSAIDs + PT for pain reduction
- Hydrotherapy / pool walking
PHASE 4 - Management of Underlying Risk Factors (Concurrent and Long-Term)
This step is frequently missed and leads to recurrence.
| Risk Factor | Intervention |
|---|---|
| Obesity | Weight loss program; every 1 kg reduction in weight = 4 kg less force per step through medial compartment |
| Knee OA | Optimize OA management (see below) |
| Diabetes mellitus | Tight glycaemic control - poorly controlled DM impairs bursal healing and increases susceptibility to infection |
| Valgus knee deformity | Medial wedge insoles (lateral heel wedge for varus) to redistribute load |
| Flat feet / overpronation | Orthotics to correct foot mechanics |
| Tight hamstrings | Ongoing stretching program as above |
Knee OA co-management:
- Intra-articular hyaluronic acid or steroid for the OA component separately
- NICE/OARSI guidelines: exercise, weight loss, topical NSAIDs, knee brace (unloader brace for medial compartment OA)
- Do not conflate OA pain with bursitis pain - they may require separate targeted treatments
PHASE 5 - Second-Line / Emerging Interventions (For Refractory Cases)
Platelet-Rich Plasma (PRP) Injection
- A 2023 RCT (Gouda et al., PMID 37810418) compared corticosteroid, PRP, and ESWT: all three were effective at reducing VAS and improving function; PRP and ESWT were comparable to each other
- PRP offers longer-lasting effect without the tissue atrophy risk of repeated steroids
- Consider as second injection if steroid response was partial and short-lived
Extracorporeal Shockwave Therapy (ESWT)
- Non-invasive; success rate 60-80% for similar peritendinous conditions
- 3-5 sessions weekly; triggers neovascularization and healing
- Comparable to PRP in the 2023 RCT above
- Good option for patients who cannot tolerate or refuse injections
Prolotherapy (Dextrose 20%) / Oxygen-Ozone Injection
- A 2024 multicenter RCT showed prolotherapy and O2-O3 are effective alternatives to corticosteroids for chronic pes anserine bursitis, with potentially more durable results
- Consider in patients with recurrent bursitis who have exhausted standard steroid injections
Mesotherapy
- Intradermal microinjections of dilute anti-inflammatory agents over the bursa
- Some supportive evidence in OA-associated pes anserine bursitis
PHASE 6 - Surgical Treatment (Last Resort)
Indication: Failure of all conservative and interventional measures after 6-12 months
Options:
- Simple incision and drainage - can relieve symptoms in distended bursa
- Bursectomy - excision of the anserine bursa; indicated for chronic recurrence refractory to all conservative measures or when chronic infection cannot be cleared
- Post-surgical rehabilitation follows the same PT protocol as conservative management
Summary Algorithm
ACUTE PAIN (days 1-14)
→ Ice + relative rest + NSAID + topical diclofenac
NO IMPROVEMENT at 2 weeks
→ Corticosteroid injection (US-guided preferred)
+ Start PT (hamstring/adductor stretching + quad strengthening)
+ Address risk factors (obesity, DM, OA, biomechanics)
RECURRENCE / PARTIAL RESPONSE
→ Consider PRP or ESWT or prolotherapy
+ Continue PT
+ Optimize underlying OA management
REFRACTORY (>6-12 months conservative treatment failed)
→ Surgical bursectomy
Key Points to Remember
- Pes anserine bursitis and knee OA very commonly coexist - treat both, not just one
- Steroid injection and physical therapy are equally effective at 8 weeks - the choice depends on patient preference and compliance
- Do NOT inject directly into the conjoined tendon - risk of rupture
- Nocturnal medial knee pain in an obese diabetic patient with known OA = think pes anserine bursitis first
- In diabetics: warn that corticosteroid injection may cause a transient blood glucose rise for 24-72 hours
- If the bursa feels warm, fluctuant, and the patient is febrile - aspirate and culture before giving any steroid
Sources: Roberts & Hedges' Clinical Procedures in Emergency Medicine; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Gouda et al. 2023 (PMID 37810418) - RCT comparing corticosteroid, PRP, ESWT; Babaei-Ghazani et al. 2024 (PMID 37752656) - RCT comparing prolotherapy, O2-O3, corticosteroid; Comparison PT vs steroid injection - PMC4968491
Generate image of exercise for above physiotherapy
Generating Image
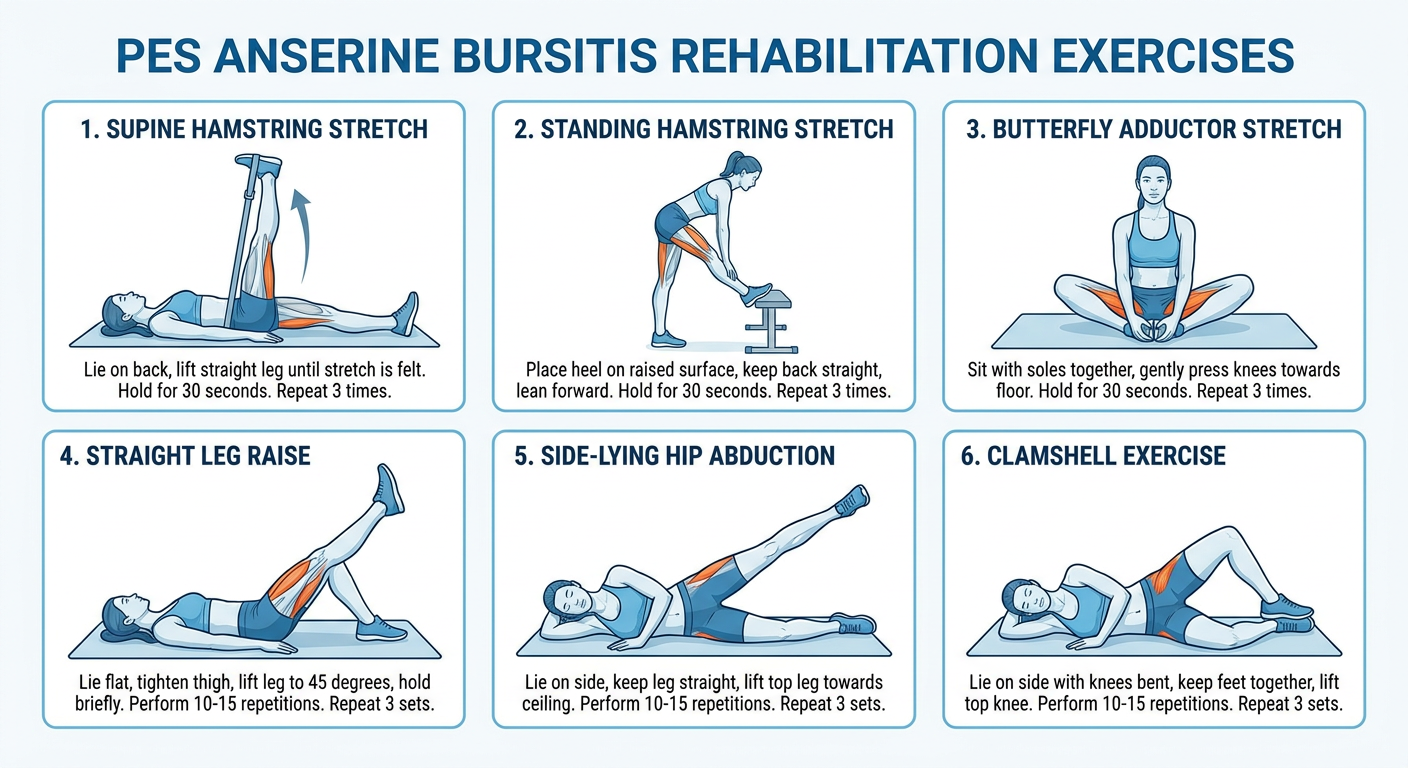
Here is a physiotherapy exercise poster covering the 6 key exercises for pes anserine bursitis rehabilitation:
| # | Exercise | Target | Sets x Reps |
|---|---|---|---|
| 1 | Supine Hamstring Stretch | Hamstrings (semitendinosus component) | Hold 30s x 3 |
| 2 | Standing Hamstring Stretch | Hamstrings | Hold 30s x 3 |
| 3 | Butterfly Adductor Stretch | Gracilis / hip adductors | Hold 30s x 3 |
| 4 | Straight Leg Raise | Quadriceps strengthening | 3 sets x 15 reps |
| 5 | Side-lying Hip Abduction | Hip abductors (reduces medial knee valgus load) | 3 sets x 15 reps |
| 6 | Clamshell Exercise | Gluteus medius / hip external rotators | 3 sets x 15 reps |
Progression guide:
- Week 1-2: Stretching only (exercises 1-3) - pain is still acute
- Week 2-3: Add straight leg raises (exercise 4)
- Week 3-6: Add hip abduction and clamshell (exercises 5-6) with resistance band as tolerated
- Ongoing: All 6 exercises daily as maintenance, especially if co-existing OA
This is a shared conversation. Sign in to Orris to start your own chat.