Apla syndrome
Reading File
Finding Sources
Searching PubMed
"antiphospholipid syndrome" management
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a detailed overview of Antiphospholipid Syndrome (APS / aPL Syndrome), synthesized from multiple authoritative textbooks.
Antiphospholipid Syndrome (APS)
Definition
Antiphospholipid syndrome (APS) is a systemic autoimmune thrombophilia characterized by recurrent venous and/or arterial thrombosis, pregnancy morbidity (recurrent fetal loss, fetal growth retardation), and persistently positive antiphospholipid (aPL) antibodies. The antibodies target plasma proteins bound to anionic phospholipids, the primary cofactor being β₂-glycoprotein I (β₂GPI).
- Goldman-Cecil Medicine, p. 795
- Brenner and Rector's The Kidney, p. 1464
Historical Background
| Year | Milestone |
|---|---|
| 1906 | Wassermann described aPL based on syphilis reactivity (VDRL test origin) |
| 1941 | Pangborn identified cardiolipin from bovine heart |
| 1963 | Lupus anticoagulant (LA) shown to cause thrombosis, not bleeding |
| 1972 | Feinstein & Rappaport coined the term "lupus anticoagulant" |
| 1983 | ELISA for anticardiolipin antibodies (aCL) developed by Harris et al. |
| 1990 | β₂GPI recognized as a phospholipid-binding protein |
| 1999 | Preliminary Sapporo classification criteria published |
| 2006 | Revised Sapporo (Sydney) classification criteria |
- Tietz Textbook of Laboratory Medicine, 7th Ed., p. (block 40)
Classification
-
Primary APS: No associated autoimmune disease (30-55% of all APS patients)
-
Secondary APS: Associated with SLE (aPL antibodies found in 25-75% of SLE patients) or other connective tissue diseases
-
Catastrophic APS (CAPS): Rare, life-threatening form with multiple simultaneous vascular occlusions ("thrombotic storm"); often fatal
-
Brenner and Rector's The Kidney, p. 1464
-
Goldman-Cecil Medicine, p. 795
Antibody Profile (Diagnostic Criteria Tests)
Three types of aPL antibodies are recognized in classification criteria:
- Lupus anticoagulant (LA) - phospholipid-based clotting test (paradoxically prolongs aPTT in vitro, but is prothrombotic in vivo)
- Anticardiolipin antibodies (aCL) - IgG and/or IgM isotype
- Anti-β₂GPI antibodies - IgG and/or IgM isotype
Important notes:
-
IgG isotype is more strongly associated with thrombosis than IgM
-
LA is the strongest risk factor for thrombosis (6x higher risk of future thrombosis)
-
aCL and anti-β₂GPI IgG are more correlated with thrombosis than IgM counterparts
-
aPL antibodies found in up to 2% of normal individuals and in infections (HIV, HCV), but these are not usually associated with clinical APS
-
"Seronegative APS": clinically suspected APS, negative for all three criteria antibodies - highlights need for additional biomarkers
-
aPL may cause a false-positive VDRL test
-
Tietz Textbook of Laboratory Medicine, 7th Ed.
-
Brenner and Rector's The Kidney, p. 1464
Classification Criteria (Revised Sapporo / Sydney 2006)
A patient is classified as APS if at least one clinical criterion AND at least one laboratory criterion are present:
Clinical Criteria
- Vascular thrombosis: One or more clinical episodes of arterial, venous, or small vessel thrombosis in any tissue/organ
- Pregnancy morbidity:
- One or more unexplained fetal deaths at or beyond 10 weeks' gestation
- One or more premature births before 34 weeks due to eclampsia, severe preeclampsia, or placental insufficiency
- Three or more unexplained consecutive spontaneous abortions before 10 weeks
Laboratory Criteria
- Positive for LA, aCL (IgG/IgM, medium or high titer), or anti-β₂GPI (IgG/IgM)
- Documented on 2 or more occasions at least 12 weeks apart, and within 5 years of clinical manifestations
Pathogenesis
The exact mechanism remains unclear but is multifactorial:
- "Two-hit" hypothesis: aPL antibodies alone may be insufficient; a "second hit" (pregnancy, oral contraceptives, nephrotic syndrome, SLE, hyperlipidemia, infection) may be required to trigger thrombosis
- Procoagulant mechanisms of aPL antibodies:
- Activation of endothelial cells, monocytes, and platelets
- Interference with multiple coagulation factors: prothrombin, protein C, annexin V, factors VII and XII, tissue factor
- Impaired fibrinolysis (inhibition of tissue plasminogen activator)
- Inhibition of mTORC intracellular pathway
- Complement activation (especially relevant in obstetric APS)
- Net result: endothelial damage and intravascular coagulation
- Genetic associations: HLA-DRB1 loci in SLE-associated APS
- Brenner and Rector's The Kidney, p. 1464
Clinical Features
Thrombotic Manifestations
In a landmark series of 1000 APS patients:
| Feature | Frequency |
|---|---|
| Deep vein thrombosis | 32% |
| Thrombocytopenia | 22% |
| Livedo reticularis | 20% |
| Stroke | 13% |
| Pulmonary embolism | 9% |
| Fetal loss | 9% |
Arterial Thrombosis
- Cerebrovascular events are the most common arterial complication: stroke, TIA, multi-infarct dementia, retinal artery occlusion
- Peripheral and intra-abdominal vascular occlusion (less common)
Cardiac
- Libman-Sacks endocarditis (nonbacterial valve vegetations) in ~1/3 of patients
- Pulmonary hypertension
Obstetric
- Recurrent spontaneous pregnancy loss
- Fetal growth retardation
- Placental thrombosis (mechanism)
- Preeclampsia, HELLP syndrome
Hematologic
- Thrombocytopenia (common)
- Prolonged aPTT (laboratory finding, paradoxical)
- Hemolytic anemia (less common)
Renal (APL Nephropathy)
Occurs in up to 25% of primary APS patients and is a distinct entity:
- Thrombosis from glomerular capillaries to main renal artery and vein
- Arterial/arteriolar lesions: intimal mucoid thickening, subendothelial fibrosis, medial hyperplasia
- Glomerular: capillary thrombosis, mesangiolysis, GBM duplication (resembles TTP/HUS)
- Interstitial fibrosis and cortical atrophy from ischemia
- Found in ~40% of aPL-positive biopsied patients vs. only 4% without aPL antibodies
- Clinical features: proteinuria (sometimes nephrotic), active urinary sediment, hypertension, progressive renal dysfunction, renal infarction, renal vein thrombosis
- Important: biopsies may be misclassified as FSGS, membranous nephropathy, or MPGN
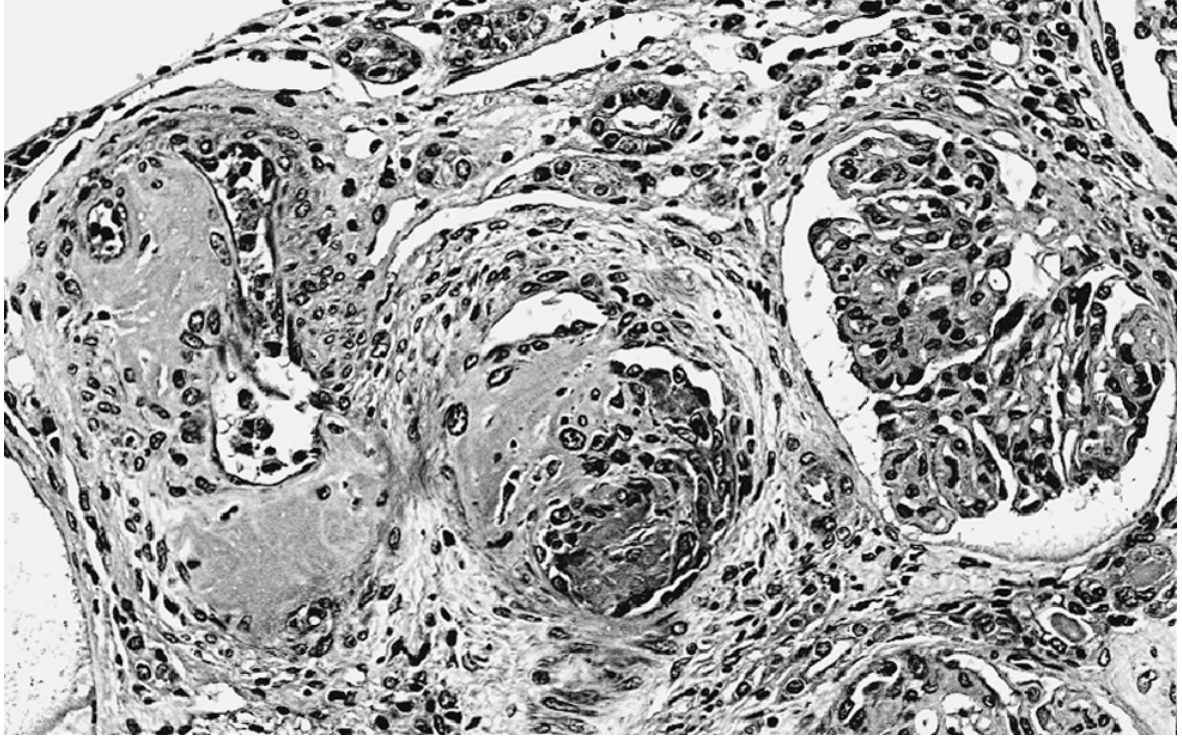
- Brenner and Rector's The Kidney, pp. 1464-1466
Laboratory Findings
- Prolonged aPTT (due to LA activity)
- Thrombocytopenia
- False-positive VDRL
- Positive aCL, anti-β₂GPI, or LA (must be confirmed on a second occasion ≥12 weeks apart)
Treatment
Acute Thrombosis
- Managed similarly to thrombosis from other causes
- LMWH preferred when LA is present (avoids aPTT monitoring difficulties, since baseline aPTT is already prolonged)
Long-Term Anticoagulation
- Warfarin is the standard of care; target INR 2.0-3.0 for most patients
- Prolonged or indefinite therapy is generally required
- Direct oral anticoagulants (DOACs) are NOT as effective as warfarin in APS - this is a critical distinction from most other thrombophilias
- For first-episode VTE with positive aPL: indefinite anticoagulation is usually recommended (though evidence is limited)
Obstetric APS
- No established treatment has been shown to definitively prevent recurrent fetal loss
- Low-dose aspirin + heparin (LMWH or UFH) is commonly used in pregnancy
Catastrophic APS (CAPS)
-
High-dose glucocorticoids
-
Therapeutic anticoagulation
-
Plasmapheresis and/or IVIG in refractory cases
-
Goldman-Cecil Medicine, pp. 795-796
Prognosis
-
Lupus anticoagulant carries the worst prognosis among aPL tests:
- 6-fold higher risk of future thrombosis
- 2-4 fold increased risk of recurrent thrombosis
- 12% increased 10-year mortality
-
SLE patients with IgG aCL have higher incidence of thrombosis and thrombocytopenia
-
In one multicenter European study of 1000 SLE patients, thrombosis occurred in 7% over 5 years
-
Goldman-Cecil Medicine, p. 795
Recent Evidence (2025)
A 2025 systematic review (Murvai et al., BMC Pregnancy Childbirth, PMID 40128683) provides a comprehensive update on APS in pregnancy, further exploring obstetric outcomes and management strategies - worth consulting for the latest evidence on pregnancy-related APS.
Sources: Brenner and Rector's The Kidney (2-Vol Set) | Goldman-Cecil Medicine | Tietz Textbook of Laboratory Medicine, 7th Ed. | Creasy & Resnik's Maternal-Fetal Medicine | Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.