Fractures of upper limb notes with diagram
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full structured notes.
Fractures of the Upper Limb - Comprehensive Notes
Sources: Bailey & Love's Short Practice of Surgery 28th Ed, Schwartz's Principles of Surgery 11th Ed, Rosen's Emergency Medicine, Rockwood & Green's Fractures in Adults 10th Ed 2025, Miller's Review of Orthopaedics 9th Ed, Campbell's Operative Orthopaedics 15th Ed 2026
1. CLAVICLE FRACTURES
Anatomy & Epidemiology
- Most common fracture in children; 90% of obstetric fractures
- Fractures typically occur at the junction of middle and distal thirds
- Proximity to subclavian vessels and brachial plexus makes neurovascular assessment essential
Mechanisms
- Birth injury: direct pressure from symphysis pubis
- Older children/adults: fall on an outstretched hand (FOOSH), direct trauma to clavicle or acromion
Classification (by location)
| Zone | Location | Frequency |
|---|---|---|
| Group 1 | Middle third | ~80% |
| Group 2 | Distal third | ~15% |
| Group 3 | Medial (proximal) third | ~5% |
Diagnosis
- AP radiograph is standard; cephalic tilt views (35-40°) for better visualisation
- CT for medial clavicle/physeal injuries
- Ultrasound for obstetric fractures
Clinical Features
- Pain at clavicle and shoulder with movement
- Crepitus, oedema, visible deformity (drooping shoulder)
- Assess for: brachial plexus injury, subclavian vessel injury, pneumothorax
Treatment
Non-operative (standard):
- Sling and swath for 4-6 weeks
- Figure-of-8 splinting NOT recommended (risk of brachial plexus palsy)
- Newborns: no treatment usually needed
Operative indications:
- Absolute: open fractures, neurovascular compromise
- Relative: non-union, malunion, displacement >2 cm, floating shoulder (with scapular fracture), high-level athletes
- Options: plate fixation or intramedullary nailing
Complications
- Non-union (1-3%)
- Pneumothorax
- Neurovascular compromise
- Malunion
2. PROXIMAL HUMERUS FRACTURES
Anatomy
- 80-90% of humeral growth occurs at proximal physis
- Fractures typically occur at the surgical neck (anatomical neck fractures are rare due to thick bone)
- Axillary nerve and posterior circumflex humeral artery are at risk - always test before relocation
Neer Classification (4-part system)
The four parts are: (1) humeral head, (2) greater tuberosity, (3) lesser tuberosity, (4) humeral shaft. A fragment counts as a "part" if displaced >1 cm or angulated >45°.

| Classification | Description |
|---|---|
| One-part | Any fracture not meeting displacement criteria (no truly displaced part) |
| Two-part | Surgical neck, anatomical neck, greater or lesser tuberosity |
| Three-part | GT + surgical neck, or LT + surgical neck |
| Four-part | All four parts displaced; highest AVN risk |
| Fracture-dislocation | Fracture + GH joint dislocation (anterior or posterior) |
Treatment
- Minimally displaced (80%): Sling immobilisation + early pendulum exercises within 2 weeks
- Displaced fractures: ORIF with locking plate and screw fixation
- Elderly/osteoporotic/4-part/head-splitting: Hemiarthroplasty or reverse shoulder arthroplasty
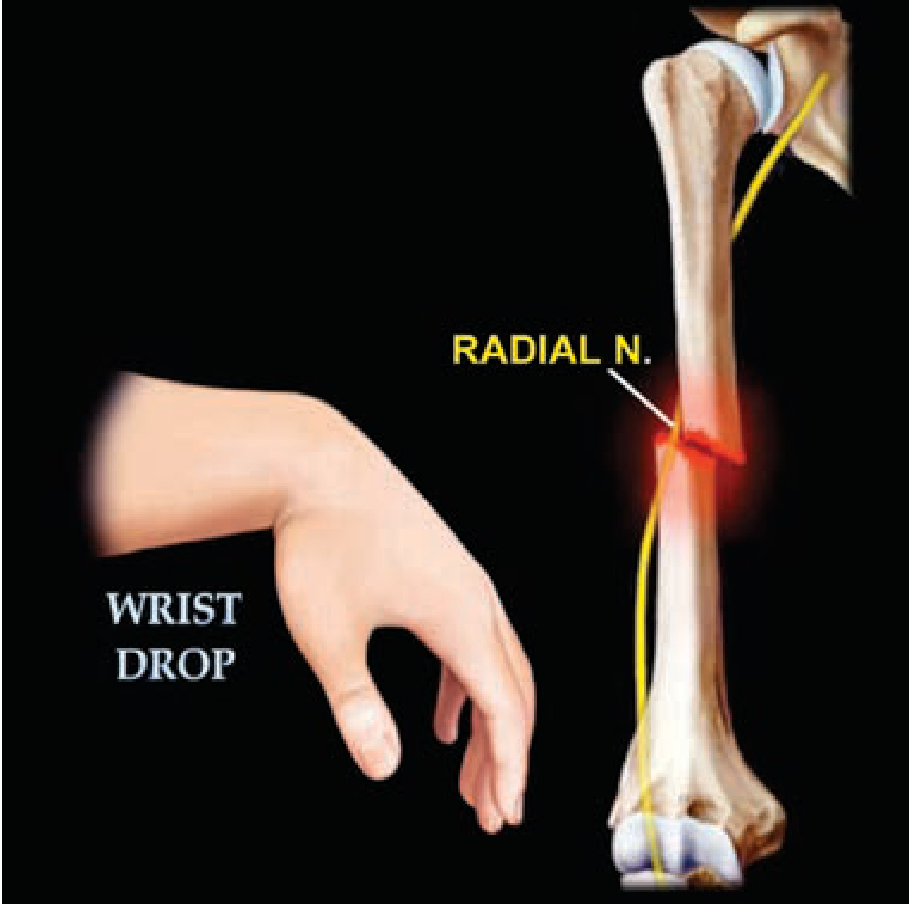
3. HUMERAL SHAFT FRACTURES
Key Points
- Most heal with non-operative management
- The radial nerve spirals in the spiral groove at the posterior humerus and is at high risk
Holstein-Lewis Fracture
- A spiral fracture of the distal one-third of the humeral shaft
- Classically associated with radial nerve neuropraxia causing wrist drop
Acceptable Alignment
- <20° anterior angulation
- <30° varus/valgus angulation
- <3 cm shortening
Treatment
- Conservative: Coaptation splint acutely → functional brace (plastic clamshell with Velcro)
- Operative: ORIF if open fracture, bilateral injuries, polytrauma, vascular injury, or failed closed reduction
- Radial nerve palsy: NOT a contraindication to conservative management; most neuropraxias recover within 3-4 months
- Exception: open fracture with radial nerve palsy → explore at time of irrigation/debridement
4. SUPRACONDYLAR FRACTURE OF THE HUMERUS
Epidemiology
- Most common elbow fracture in children
- Mechanism: fall on extended outstretched arm → distal fragment goes posterior/superior (extension type, ~97%)
Gartland Classification (Extension type)
| Type | Description |
|---|---|
| I | Undisplaced |
| II | Displaced but posterior cortex intact (hinge) |
| III | Completely displaced, no cortical contact |
Clinical Features
- Swelling, tenderness, reluctance to move
- CRITOE mnemonic for ossification centres (Capitellum, Radial head, Internal epicondyle, Trochlea, Olecranon, External epicondyle) - important to avoid mistaking for fracture lines on X-ray
Neurovascular Complications
- White pulseless hand: surgical emergency - urgent reduction required; if pulse does not return, vascular exploration needed
- Pink pulseless hand: more controversial; satisfactory perfusion - reduce and stabilise, take expectant approach; pulse often returns in 24-48 hours
- Nerve injury: most common is anterior interosseous nerve (AIN) - neuropraxia, typically resolves post-reduction
- Volkmann's ischaemic contracture: feared complication from excessive swelling and missed compartment syndrome; do NOT put elbow in deep flexion if very swollen
Treatment
- Type I: Collar and cuff or backslab, 3 weeks
- Type II: Closed reduction + above-elbow cast if periosteal hinge intact
- Type III: Closed reduction + percutaneous K-wires + above-elbow cast
- Malunion in cubitus varus (gunstock deformity) requires corrective osteotomy if symptomatic
5. FOREARM FRACTURES (Radius & Ulna)
Monteggia Fracture-Dislocation
- Fracture of the proximal ulna + dislocation of the radial head
- Check the radiocapitellar line on lateral X-ray: a line drawn along the radial shaft should pass through the centre of the capitellum - disruption indicates radial head dislocation
- Treatment: Closed reduction and casting; reduction of ulna fracture usually reduces the radial head
Galeazzi Fracture-Dislocation
- Fracture of the distal radius + disruption of the distal radioulnar joint (DRUJ)
- Sometimes called a "fracture of necessity" in adults (ORIF required)
- Treatment: Orthopedic consultation; ORIF of radius usually required in adults; cast in children
| Eponym | Fracture | Dislocation |
|---|---|---|
| Monteggia | Proximal ulna | Radial head (proximal RUJ) |
| Galeazzi | Distal radius | DRUJ (distal RUJ) |
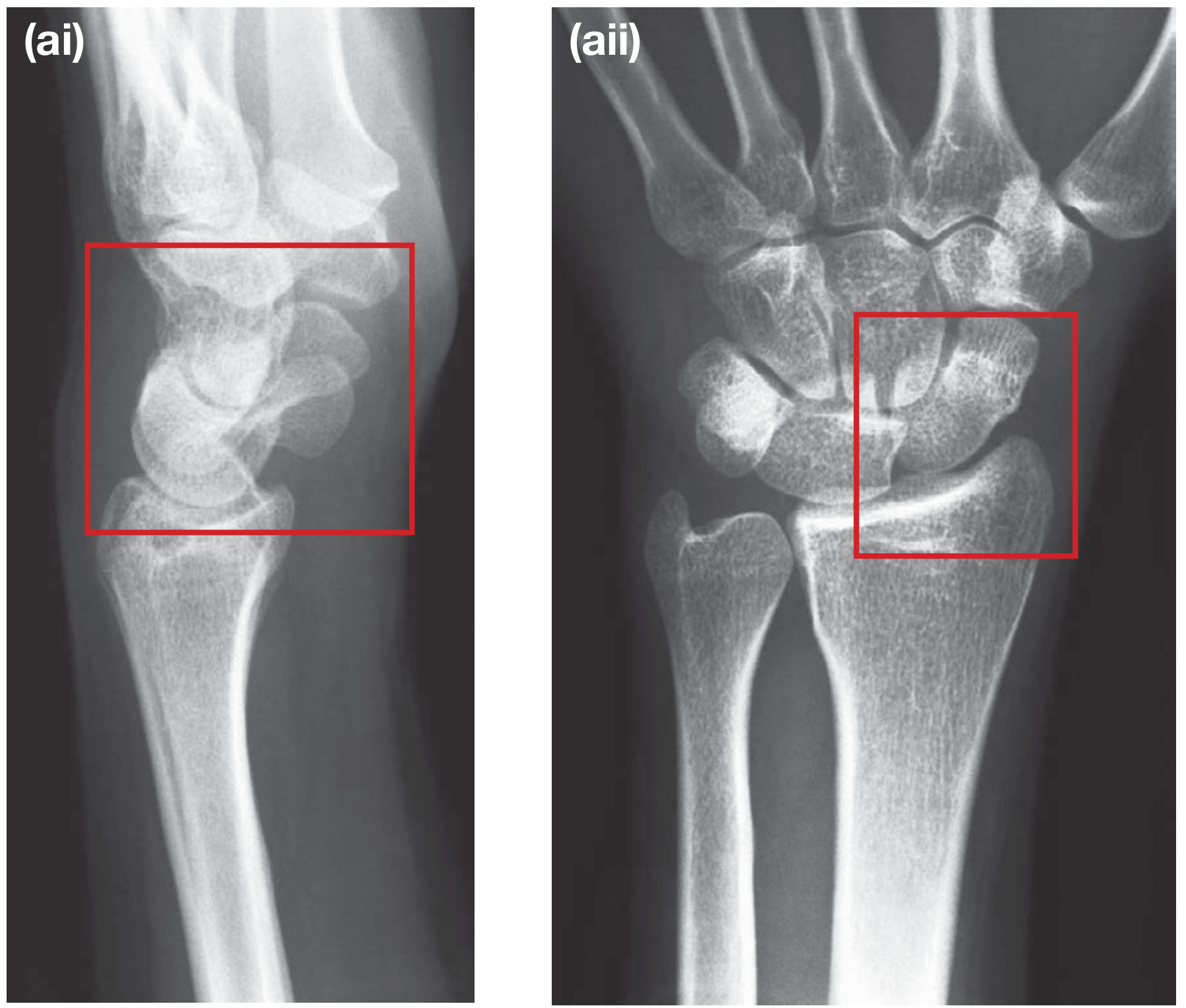
6. DISTAL RADIUS FRACTURES
Important Eponyms
| Eponym | Mechanism | Displacement | Key Feature |
|---|---|---|---|
| Colles' | FOOSH (extension) | Dorsal displacement + angulation | "Dinner fork deformity"; within 2 cm of articular surface |
| Smith's | Fall on flexed wrist (FOIF) | Volar displacement + angulation | "Garden spade deformity"; reverse Colles' |
| Barton's | Shear force | Intra-articular, dorsal subluxation | Dorsal rim fracture with radiocarpal subluxation |
| Reverse Barton's | Shear force | Intra-articular, volar subluxation | Volar rim fracture |
| Chauffeur's | Compression by scaphoid | Radial styloid isolated | Intra-articular, from hand-crank backfire |
Colles' Fracture - Classic Features
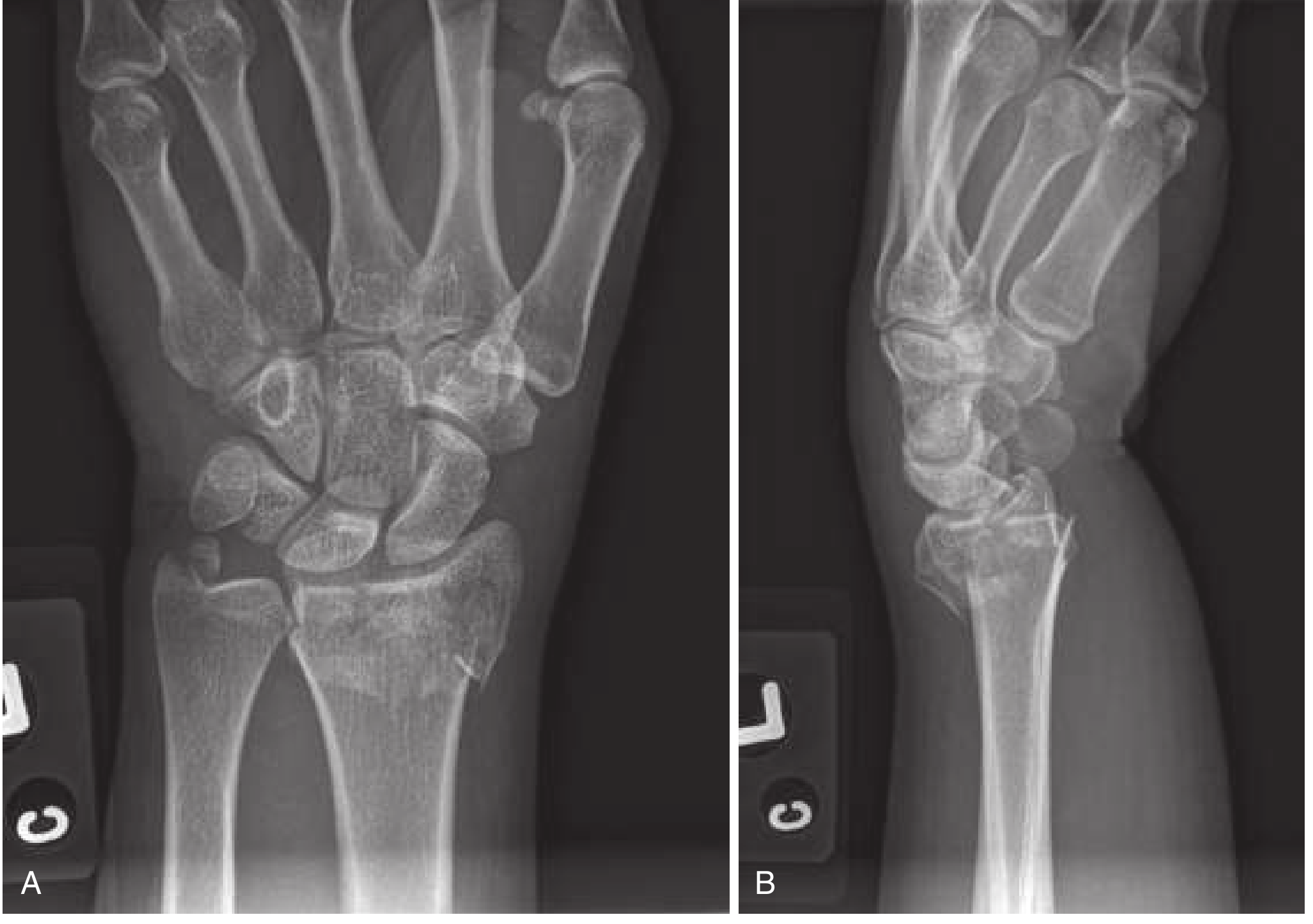
- Median nerve is most commonly injured (contusion, traction, or carpal tunnel syndrome)
- Indications for ED reduction: Neurovascular compromise, dorsal angulation >20°, significant deformity, skin tenting
- Reduction technique: Procedural sedation or hematoma block (5-10 mL 1% lidocaine into fracture haematoma via dorsal approach); finger traps useful
- Immobilisation: Double sugar-tong splint; avoid circumferential cast for 24 hours due to oedema
Scaphoid Fracture (special consideration at wrist)
- Blood supply enters distally and runs in retrograde fashion - waist fractures risk AVN of proximal pole
- May be radiographically occult initially
- Tender in anatomical snuffbox after FOOSH = treat as scaphoid fracture until excluded
- Investigate with: Repeat X-rays at 10-14 days, bone scan, MRI (most sensitive), or CT
- Undisplaced: Below-elbow cast (thumb immobilisation not routinely required)
- Displaced/unstable (>1 mm): ORIF with headless compression screw
- Complications: Non-union, AVN, malunion, carpal instability
7. HAND FRACTURES
Bennett's Fracture
- Intra-articular fracture at the base of the 1st metacarpal (thumb CMC joint)
- A small volar fragment remains attached to the trapezium by the volar oblique ligament; the remainder of the metacarpal is pulled proximally and radially by abductor pollicis longus
- Treatment: Closed reduction (often unstable) → percutaneous K-wire fixation or ORIF
Rolando's Fracture
- Comminuted intra-articular fracture of the 1st metacarpal base (Y or T pattern)
- More complex and worse prognosis than Bennett's
- Treatment: ORIF if fragments large enough; spanning external fixation for highly comminuted
Boxer's Fracture (5th Metacarpal Neck)
- FOOSH or punch mechanism
- Typical finding: volar angulation of the metacarpal head
- Acceptable angulation: up to 40° for 5th metacarpal (10° for 2nd/3rd)
- Treatment: Buddy strapping ± ulnar gutter splint; ORIF if >40° or rotational deformity
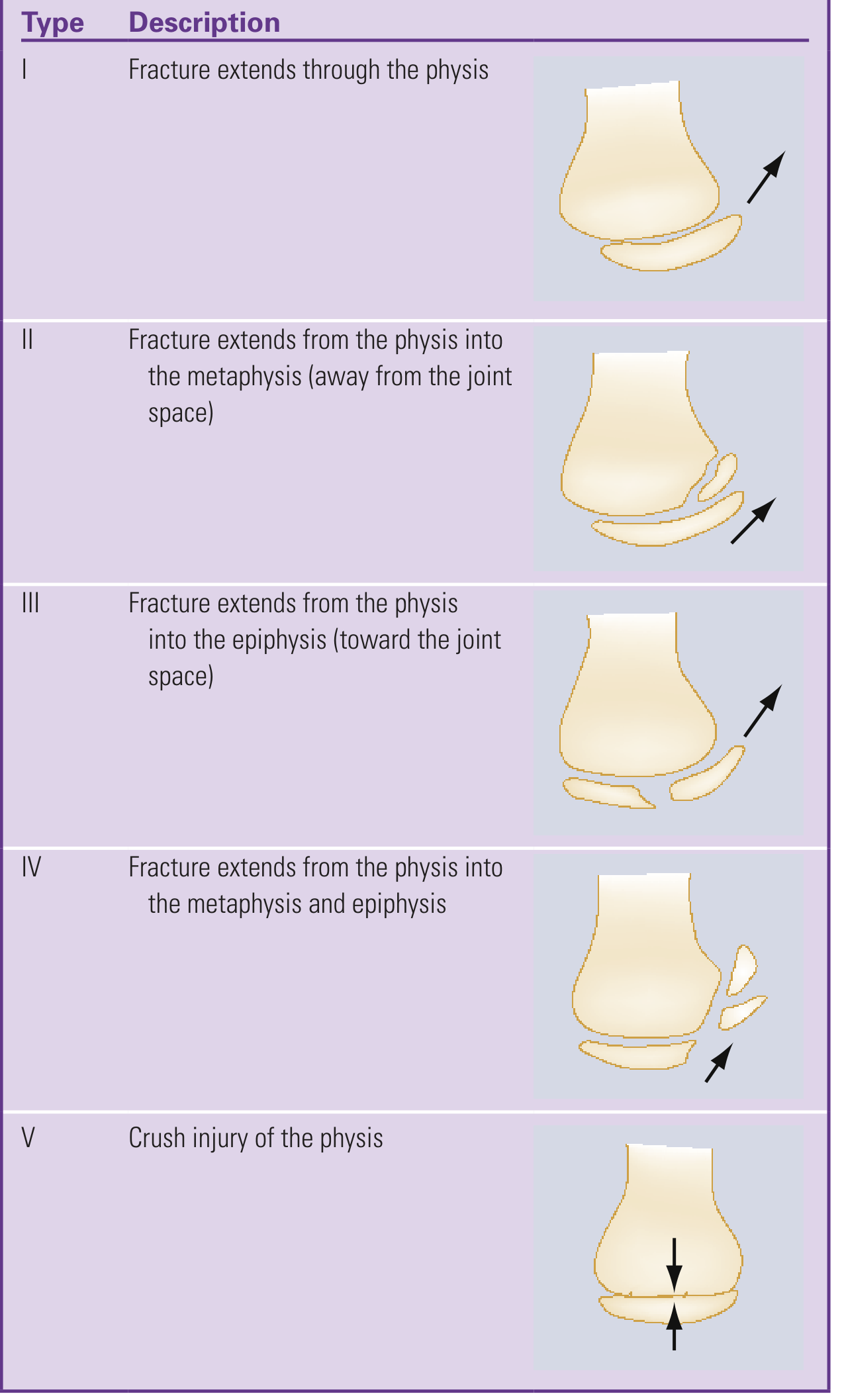
8. SALTER-HARRIS CLASSIFICATION (Physis Fractures in Children)
Relevant to many upper limb fractures in skeletally immature patients:
| Type | Description | Mnemonic | Prognosis |
|---|---|---|---|
| I | Through physis only | Straight through | Good |
| II | Physis + metaphysis | Above (metaphysis) | Good (most common) |
| III | Physis + epiphysis | Lower (epiphysis) | Fair |
| IV | Physis + metaphysis + epiphysis | Through all | Poor |
| V | Crush injury of physis | Everything (crush) | Very poor |
9. NEUROLOGICAL ASSESSMENT OF THE UPPER LIMB AFTER FRACTURE
| Nerve | Motor Test | Sensory Area | Vulnerable Fracture |
|---|---|---|---|
| Radial | Wrist extension | Thumb-index web space | Humeral shaft (Holstein-Lewis) |
| Median | Thumb opposition; wrist flexion + abduction | Thumb, index, middle fingers | Supracondylar, Colles' |
| Ulnar | Wrist flexion + adduction; finger abduction | Little finger | Medial epicondyle, distal humerus |
| AIN (branch of median) | Distal thumb/index flexion (OK sign) | None | Supracondylar |
| Axillary | Deltoid (shoulder abduction) | Regimental badge area | Surgical neck humerus, shoulder dislocation |
10. QUICK SUMMARY TABLE
| Fracture | Mechanism | Key Clinical Feature | Nerve at Risk | Treatment |
|---|---|---|---|---|
| Clavicle | FOOSH, direct blow | Drooping shoulder | Brachial plexus | Sling; ORIF if displaced >2 cm |
| Surgical neck humerus | Fall on shoulder | Elderly patient | Axillary nerve | Sling ± ORIF; arthroplasty if 4-part |
| Humeral shaft | Direct blow, twisting | Wrist drop | Radial nerve | Functional brace; ORIF if open/vascular |
| Supracondylar | FOOSH (extended elbow) | Elbow swelling, "S-shaped" limb | AIN, brachial artery | K-wires; urgent if vascular |
| Monteggia | Direct ulna blow | Radial head dislocation | PIN (post interosseous) | Closed reduction; reduce ulna = reduces head |
| Galeazzi | FOOSH | DRUJ tenderness | - | ORIF radius in adults |
| Colles' | FOOSH (extension) | Dinner fork deformity | Median nerve | Reduction + sugar-tong splint |
| Smith's | Fall on flexed wrist | Garden spade deformity | - | ORIF often needed |
| Scaphoid | FOOSH | Snuffbox tenderness; X-ray often normal | - | Cast; ORIF if displaced |
| Bennett's | Axial load on thumb | Thumb CMC instability | - | K-wire or ORIF |
Sources: Bailey & Love's Short Practice of Surgery 28th Ed • Schwartz's Principles of Surgery 11th Ed • Rosen's Emergency Medicine • Rockwood & Green's Fractures in Adults 10th Ed 2025 • Miller's Review of Orthopaedics 9th Ed • Campbell's Operative Orthopaedics 15th Ed 2026 • Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.