New admission under Dr Ravikumar sir (Emergency ot booked for today) Brundha N 27/F MH01107338 Insurance 512 C/o pain and swelling in her left ankle since 1 day Patient gives a/h/o skid and fall from 2 wheeler on 15/07/2026 at around 9:30 am near Ramaiah degree college following which she sustained injury to her right ankle and started c/o pain sudden in onset,non progressive,associated with swelling around the ankle,aggravated on movements and relieved on immobilisation and taking medications No H/o head injury/LOC/ENT bleed No known comorbs Diagnosis-Right ankle bimalleolar fracture Plan-Right lateral malleolus ORIF + plating and medial malleolus cc screw fixation I’m scrubbing in for this , everything I need to know
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have everything needed. Here is your full surgical scrub guide for this case.
Surgical Scrub Guide
Right Ankle Bimalleolar Fracture - ORIF
Brundha N | 27/F | MH01107338 | Dr. Ravikumar | Emergency OT - 16/07/2026
PATIENT SNAPSHOT
| Injury | Skid and fall from 2-wheeler, 15/07/2026, ~09:30 hrs |
| Diagnosis | Right ankle bimalleolar fracture |
| Plan | Right lateral malleolus ORIF + plating; Medial malleolus CC screw fixation |
| Time from injury | ~30 hours - within acceptable early ORIF window |
| Comorbidities | Nil |
| Anaesthesia | Spinal/GA (discuss with anaesthetist) |
WHY ORIF IS INDICATED
Bimalleolar fractures disrupt both medial and lateral stabilizing structures of the ankle. Displacement reduces tibiotalar contact area and alters joint kinematics. Closed reduction cannot be reliably maintained as swelling subsides. Key data points to know:
- ~10% nonunion with closed treatment
- 20% have intraarticular injuries to talus/tibia that are missed without surgical exploration
- Randomized prospective long-term studies confirm superior outcomes with ORIF over nonoperative treatment for bimalleolar fractures
Campbell's Operative Orthopaedics 15th Ed 2026, p. 3322
TIMING NOTE
ORIF is ideally done within the first 12 hours OR delayed 2-3 weeks to allow swelling resolution. This patient is ~30 hours out - she falls in a borderline zone. If there is no significant blistering or skin compromise, proceeding tonight is appropriate, and equivalent outcomes have been demonstrated with immediate vs delayed ORIF in Weber B fractures.
DANIS-WEBER CLASSIFICATION (know before you scrub)

- Type A - fibula fracture at or below the plafond (infrasyndesmotic) - internal rotation + adduction mechanism
- Type B - oblique fibula fracture at level of syndesmosis (transsyndesmotic) - external rotation mechanism - most common, likely what Brundha has
- Type C - fibula fracture above the syndesmosis (suprasyndesmotic) - syndesmosis always disrupted
Bimalleolar fractures are most commonly Weber B (supination-external rotation type IV), consistent with a twisting mechanism during a fall.
SETUP & POSITIONING
- Position: Supine, ipsilateral hip bumped to internally rotate the limb OR lateral decubitus depending on surgeon preference
- Tourniquet: Upper thigh pneumatic tourniquet (inflate ~250-300 mmHg or 100 mmHg above systolic)
- C-arm: Standard ankle views - AP, mortise (15-20° internal rotation), lateral
- Limb prep: Knee to toes, free-draped
- Table: Radiolucent
IMPLANTS TO HAVE READY
Lateral Malleolus (Fibula)
- 1/3 semitubular plate, 3.5 mm (standard lateral plating) - most common construct
- 3.5 mm cortical screws (multiple lengths - have 30 mm to 55 mm range)
- 3.5 mm lag screws (if oblique fracture - interfragmentary compression before plating)
- Optional: Posterior antiglide plate if posterolateral approach chosen
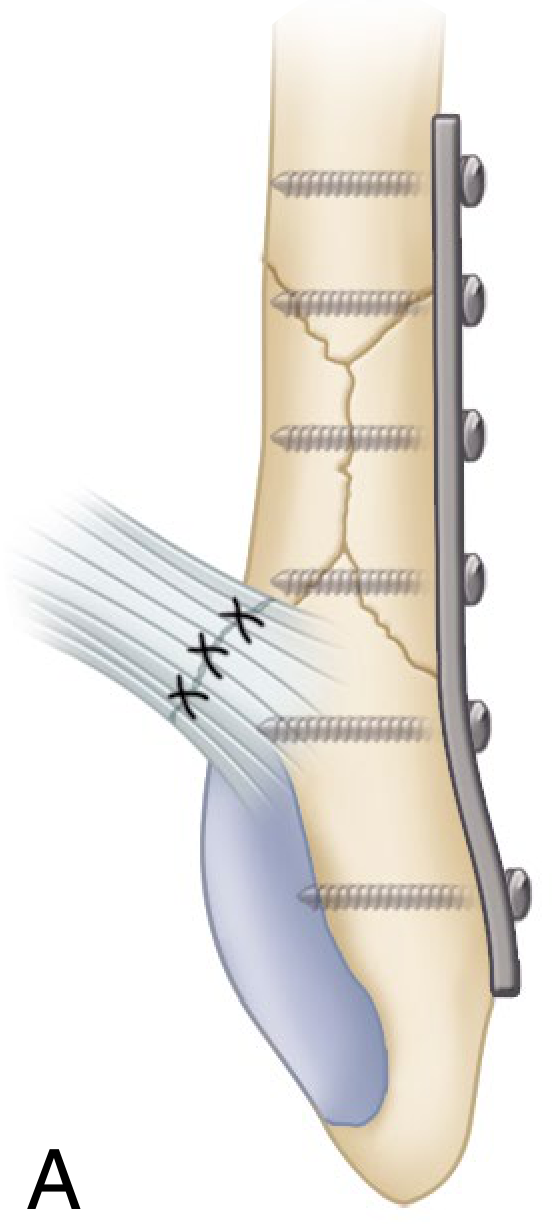
Standard fixation: one-third semitubular 3.5 mm plate and screws (A above), or lag screws for simple oblique fractures in young patients with good bone stock.
Medial Malleolus (CC Screw)
- Two 4.0 mm cannulated cancellous (CC) screws - standard fixation, oriented perpendicular to fracture line
- Guidewires x2 (for CC screws)
- Alternative: 3.5 mm bicortical lag screws or tension band wiring if fragment is small
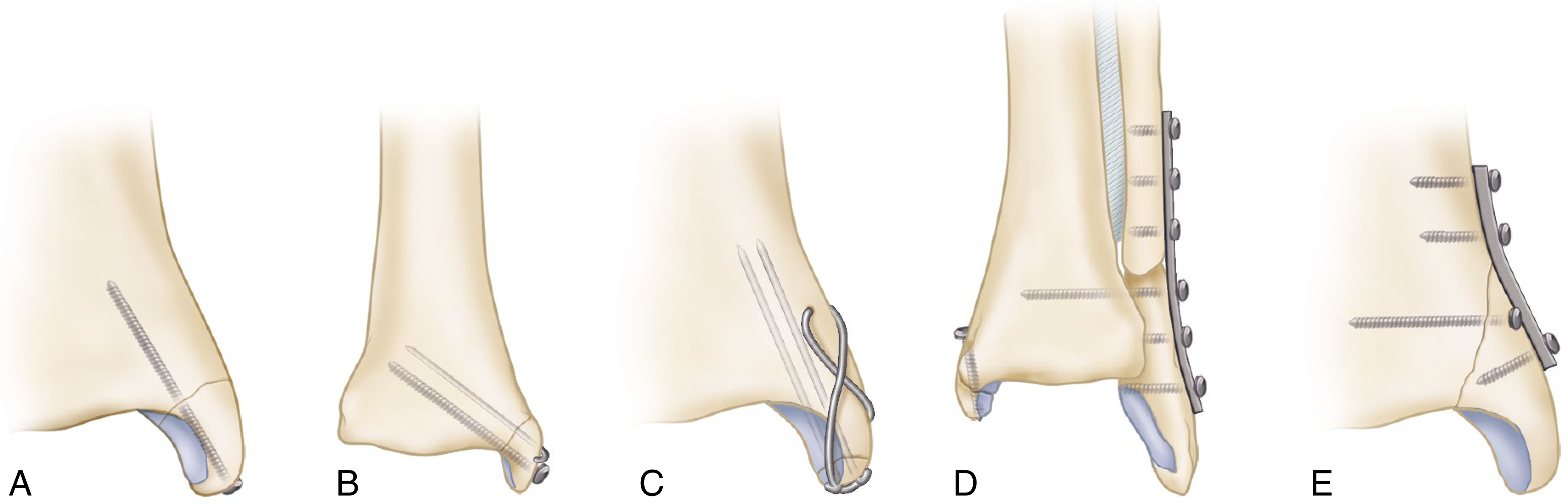
A = single lag screw (large fragment) | B = two lag screws | C = tension band wiring | D/E = plate fixation
Syndesmosis (Have Available - assess intraoperatively)
- One or two 3.5 mm or 4.5 mm cortical syndesmotic screws (quadricortical or tricortical)
- Usually placed 2-4 cm above the plafond, through distal plate hole if possible
- Assess with Cotton test + external rotation stress under fluoro after lateral fixation
SURGICAL SEQUENCE (Campbell's Technique 59.1)
Step 1 - Lateral Malleolus First (standard order)
Fix lateral before medial UNLESS the lateral is comminuted, in which case fix medial first to avoid over-reduction of the coronal plane.
-
Incision: Lateral longitudinal incision over distal fibula
- Protect the superficial peroneal nerve - identify and retract
- Alternatively: posterolateral incision for antiglide plating (avoids palpable implant over lateral surface)
- Expose fibula extraperiosteally
-
Fracture reduction:
- Reduce fracture and hold with reduction clamp / K-wires provisionally
- If oblique fracture with good bone stock - place one or two 3.5 mm lag screws anterior to posterior (1 cm apart, at least 1 cm from fracture line) for interfragmentary compression first
-
Plate application:
- Apply 1/3 semitubular plate to lateral surface of fibula
- Proximal screws: bicortical fixation (3.5 mm cortical)
- Distal screws: bicortical where possible
- Confirm length, rotation and alignment on fluoroscopy (AP + mortise + lateral)
-
Intraoperative syndesmosis assessment (Cotton test + external rotation stress):
- Hook the fibula and pull laterally while stabilizing the tibia
- >3-4 mm displacement = syndesmotic fixation needed
- If stable: proceed to medial side
- If unstable: place syndesmotic screw through distal plate hole, 2-4 cm above plafond, parallel to joint (NOT in dorsiflexion)
Step 2 - Medial Malleolus (CC Screw Fixation - Technique 59.2)
-
Incision: Medial longitudinal incision directly over medial malleolus, curving slightly anteriorly
- Protect the saphenous nerve and vein anteriorly
- Identify fracture, clear hematoma and any soft tissue interposition (periosteum can block reduction - clean the fracture site)
-
Reduction:
- Direct reduction with periosteal elevator
- Hold with two K-wires bent to stay out of the way (as per AO technique, Fig 59.6)
-
Guidewire placement (for cannulated screws):
- Drill 3.2 mm guide hole perpendicular to fracture line
- Measure depth
- Two parallel guidewires
-
Screw insertion:
- Insert two 4.0 mm CC screws without tapping
- Screws oriented perpendicular to fracture - lag effect for compression
- Remove K-wires after screws tightened
- If fragment tends to rotate: add a smaller screw or K-wire
-
Confirm on fluoroscopy: Mortise view - assess medial clear space (normal ≤4 mm), tibiotalar congruence, screw position (should not enter joint)
FLUOROSCOPIC CHECKPOINTS
| View | What to check |
|---|---|
| Mortise (15-20° IR) | Medial clear space ≤4 mm; symmetric joint space; talar shift |
| AP | Fibular length restored; distal tip of fibula at level of talar dome |
| Lateral | No anterior talar translation; no posterior malleolus displacement |
NERVES AT RISK - KNOW BEFORE YOU CUT
| Nerve | Location | Risk |
|---|---|---|
| Superficial peroneal nerve | Lateral approach, crosses fibula ~10 cm above tip | Lateral incision - identify and protect |
| Sural nerve | Posterior to lateral malleolus | Posterolateral approach |
| Saphenous nerve + GSV | Anterior to medial malleolus | Medial incision |
| Deep peroneal nerve | Anterior compartment | Minimal risk with standard approach |
SYNDESMOTIC FIXATION - QUICK REFERENCE
Indications (confirmed need):
- Fibula fracture above the distal tibiofibular joint (Weber C)
- Cotton test positive (>3-4 mm displacement)
- External rotation stress test positive on fluoro after lateral fixation
- Syndesmotic disruption extending >5 cm proximal to plafond
Technique:
- 1-2 cortical screws (3.5 or 4.5 mm), placed 2-4 cm above plafond
- Through both fibular cortices + 1 or 2 tibial cortices
- Ankle in neutral/slight dorsiflexion during placement (prevents over-compression)
- Reduce syndesmosis with pointed reduction forceps before drilling
- Confirm fibular position in incisura on axial fluoro/CT if uncertain
For Weber B bimalleolar (likely this patient): syndesmosis disruption is possible but not universal. The Cotton test and external rotation stress after fibular fixation will decide.
INSTRUMENTS NEEDED
- Standard trauma set
- Small fragment set (3.5 mm screws, 1/3 tubular plates)
- Cannulated screw set (4.0 mm CC for medial malleolus)
- Large pointed reduction forceps x2
- Bone hook
- K-wires (1.6 mm and 2.0 mm)
- Drill bits: 3.2 mm (for CC guidewire / screw prep), 2.5 mm
- Depth gauge, tap (if non-cannulated)
- C-arm
- Small Hohmann retractors x2
POSTOPERATIVE PLAN (standard)
- Below-knee backslab initially (wait for swelling to settle)
- Non-weight bearing x 6 weeks
- Convert to boot at 6 weeks if union progressing
- Partial WB at 6-8 weeks, full WB at 10-12 weeks
- Physiotherapy for ROM and strengthening
POTENTIAL INTRAOPERATIVE ISSUES
| Situation | What to do |
|---|---|
| Comminuted lateral malleolus | Fix medial malleolus first; use bridge plating / fibula nail for lateral |
| Small medial malleolar fragment | Use K-wire + single screw, or tension band wiring |
| Positive Cotton test after lateral fixation | Add syndesmotic screw before closing |
| Cannot achieve medial clear space | Check for soft tissue interposition (periosteum, deltoid) in fracture gap |
| Fracture blisters / skin compromise noticed on table | Consider staged procedure or wound VAC |
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 (Chapter 59, pp. 3322-3328); Rockwood & Green's Fractures in Adults 10th Ed 2025
Good luck in there - you've got this.
This is a shared conversation. Sign in to Orris to start your own chat.