lesser sac
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a complete account of the lesser sac (omental bursa) drawn from Gray's Anatomy for Students, Fischer's Mastery of Surgery, the Color Atlas of Human Anatomy, and Pye's Surgical Handicraft.
Lesser Sac (Omental Bursa)
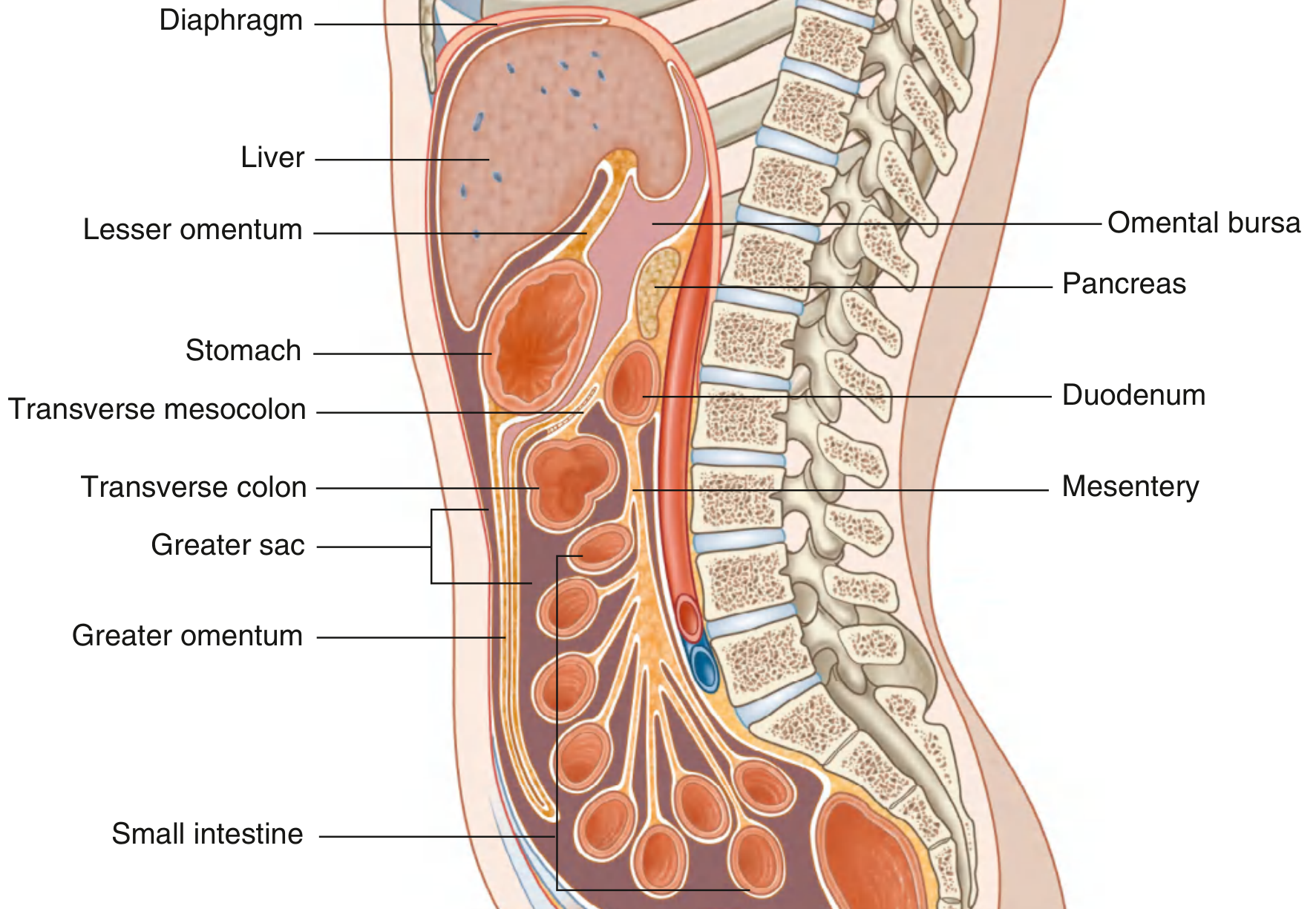
The lesser sac is a smaller, nearly completely enclosed subdivision of the peritoneal cavity that lies posterior to the stomach and lesser omentum. It communicates with the greater sac through a single natural opening - the omental (epiploic) foramen (of Winslow).
Boundaries
| Wall | Structures |
|---|---|
| Superior | Liver (caudate lobe) and diaphragm |
| Anterior | Stomach and lesser omentum |
| Posterior | Parietal peritoneum covering the pancreas, aorta, left kidney, left adrenal gland |
| Inferior | Transverse mesocolon |
| Left | Splenic ligaments (gastrosplenic and splenorenal ligaments) |
| Right | Opens into greater sac via the omental foramen |
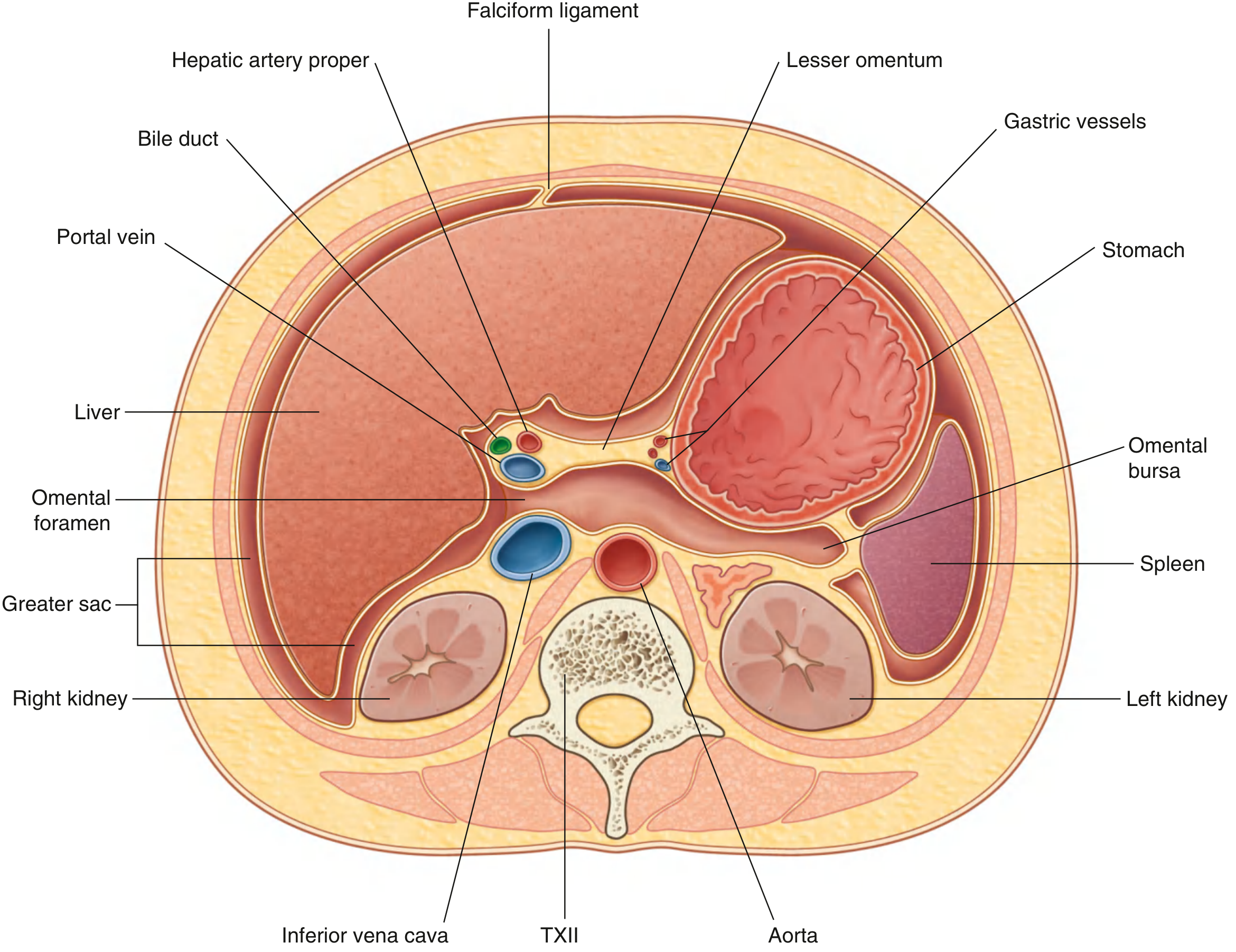
Omental (Epiploic) Foramen
The only natural entrance to the lesser sac. Its boundaries are:
- Anteriorly: Hepatoduodenal ligament (containing the portal vein, hepatic artery proper, and bile duct)
- Posteriorly: Inferior vena cava (covered by peritoneum)
- Superiorly: Caudate lobe of the liver
- Inferiorly: First part of the duodenum
Internal Subdivisions
-
Vestibule - the first area entered after passing through the omental foramen; bounded anteriorly by the lesser omentum and posteriorly by parietal peritoneum. The papillary process of the caudate lobe projects into it. The gastropancreatic fold (containing the left gastric artery) divides the vestibule from the main cavity.
-
Superior recess - extends upward between the esophagus and inferior vena cava toward the gastric fundus.
-
Splenic (left) recess - extends left between the splenic ligaments and the stomach.
-
Inferior recess - extends downward between the greater curvature of the stomach and the transverse colon.
Surgical Significance
Pringle maneuver: A finger inserted through the omental foramen can compress the hepatoduodenal ligament between the thumb and index finger - occluding the hepatic artery and portal vein to achieve rapid inflow control of the liver.
Posterior gastric ulcer perforation: If a posterior gastric ulcer perforates, contents leak into the lesser sac rather than the general peritoneal cavity. This can cause a lesser sac abscess or collection with:
- Epigastric mass, ileus, persistent nasogastric aspirates, swinging pyrexia
- Symptoms: malaise, abdominal fullness, nausea, vomiting, fever
(Anterior perforations contaminate the subphrenic or subhepatic spaces directly.)
Acute pancreatitis: Pancreatic exudate and pseudocysts typically collect in the lesser sac because the pancreas forms its posterior wall.
Surgical access to the lesser sac is achieved by:
- Dividing the lesser omentum
- Dividing the gastrocolic ligament (entering below the greater curvature)
- Dividing the transverse mesocolon
Embryological Basis
The lesser sac forms during stomach rotation. As the stomach rotates 90° clockwise (when viewed from above), its originally left surface faces posteriorly - and the space created behind it expands into the omental bursa. The dorsal mesogastrium enlarges to form the greater omentum, and the splenic recess develops as the spleen grows within the dorsal mesentery.
Sources: Gray's Anatomy for Students, 4th ed., p. 363 | Fischer's Mastery of Surgery, 8th ed., p. 4493 | Color Atlas of Human Anatomy Vol. 2, p. 373 | Pye's Surgical Handicraft, 22nd ed.
This is a shared conversation. Sign in to Orris to start your own chat.