Organ autopsy technique
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough account of organ autopsy technique, drawn from two authoritative forensic medicine textbooks.
Organ Autopsy Technique
1. The Four Classical Techniques for Organ Removal
These are the standard methods, each differing in how organs are removed from the body:
| Technique | Method | Key Feature | Preferred When |
|---|---|---|---|
| Virchow's | Organs removed one by one | Cranium first, then spinal cord, thoracic, cervical, abdominal | Most widely used; best for detailed study of individual organs |
| Rokitansky's | In situ dissection + en bloc removal | Partial in-place examination | Infectious cases (HIV, Hepatitis B) - limits spread of infection |
| Letulle's | All cervical, thoracic, abdominal, pelvic organs removed en masse | All attachments and inter-organ connections preserved | Best for routine inspection; body available to undertaker within 30 minutes |
| Ghon's | Cervical, thoracic, abdominal organs + urogenital system removed as blocks; neuronal system as a separate block | Modified en bloc | When organ systems need to be studied as discrete blocks |
Virchow's - cannot study anatomico-pathological relationships (organs separated). Letulle's - preserves relationships but the organ mass is awkward to handle. Rokitansky's - organs cannot be studied in as much detail.
- The Essentials of Forensic Medicine and Toxicology, 36th ed.; PC Dikshit Textbook of Forensic Medicine and Toxicology
2. Instruments
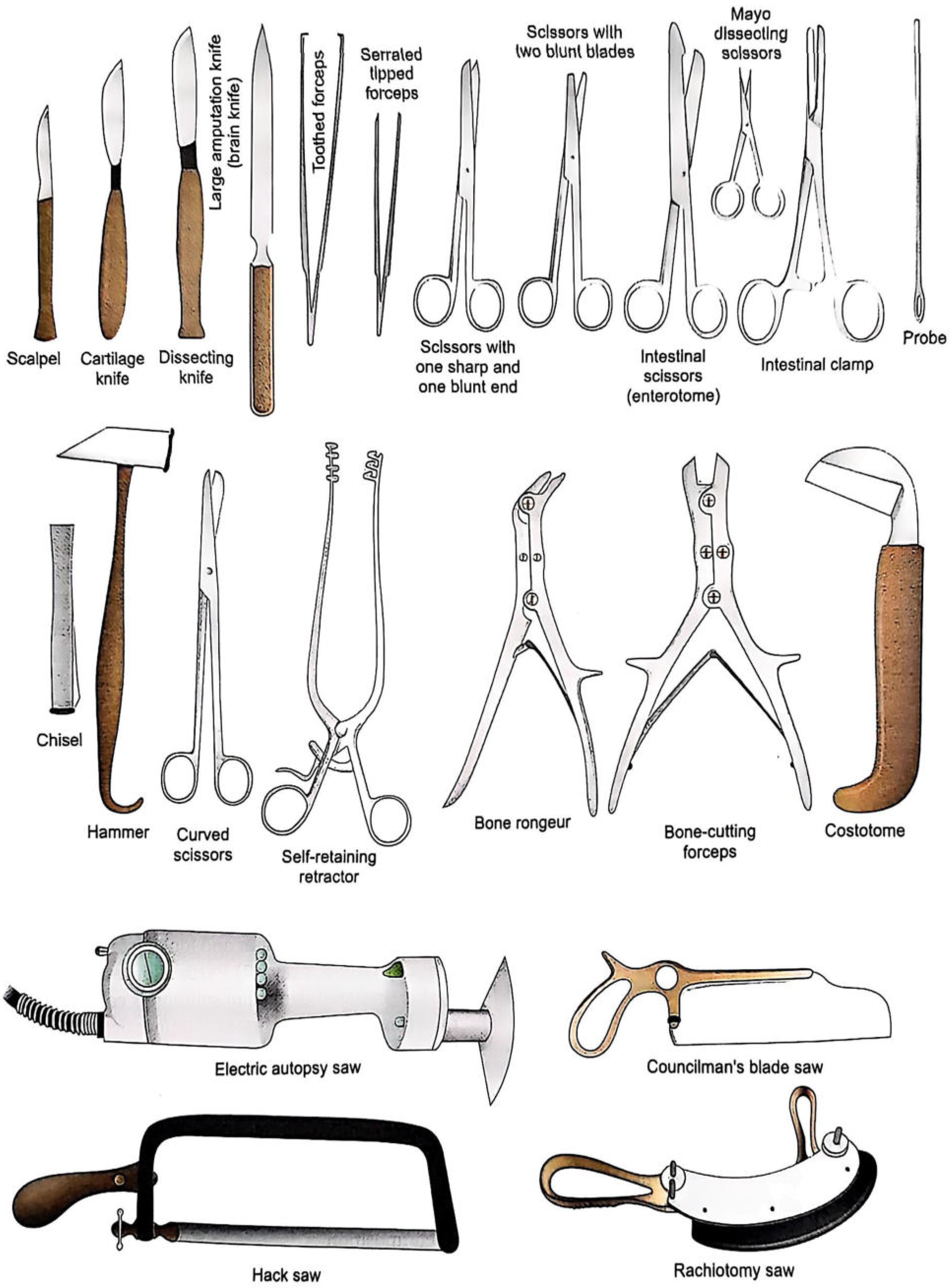
Fig: Standard autopsy instruments
Key instruments include: scalpel, cartilage knife, dissecting knife, large amputation (brain) knife, toothed/serrated forceps, intestinal scissors (enterotome), bone rongeur, costotome, chisel and hammer, electric autopsy saw, hacksaw, and rachiotomy saw.
3. Primary Skin (External) Incisions
Three types are used, selected based on the case:
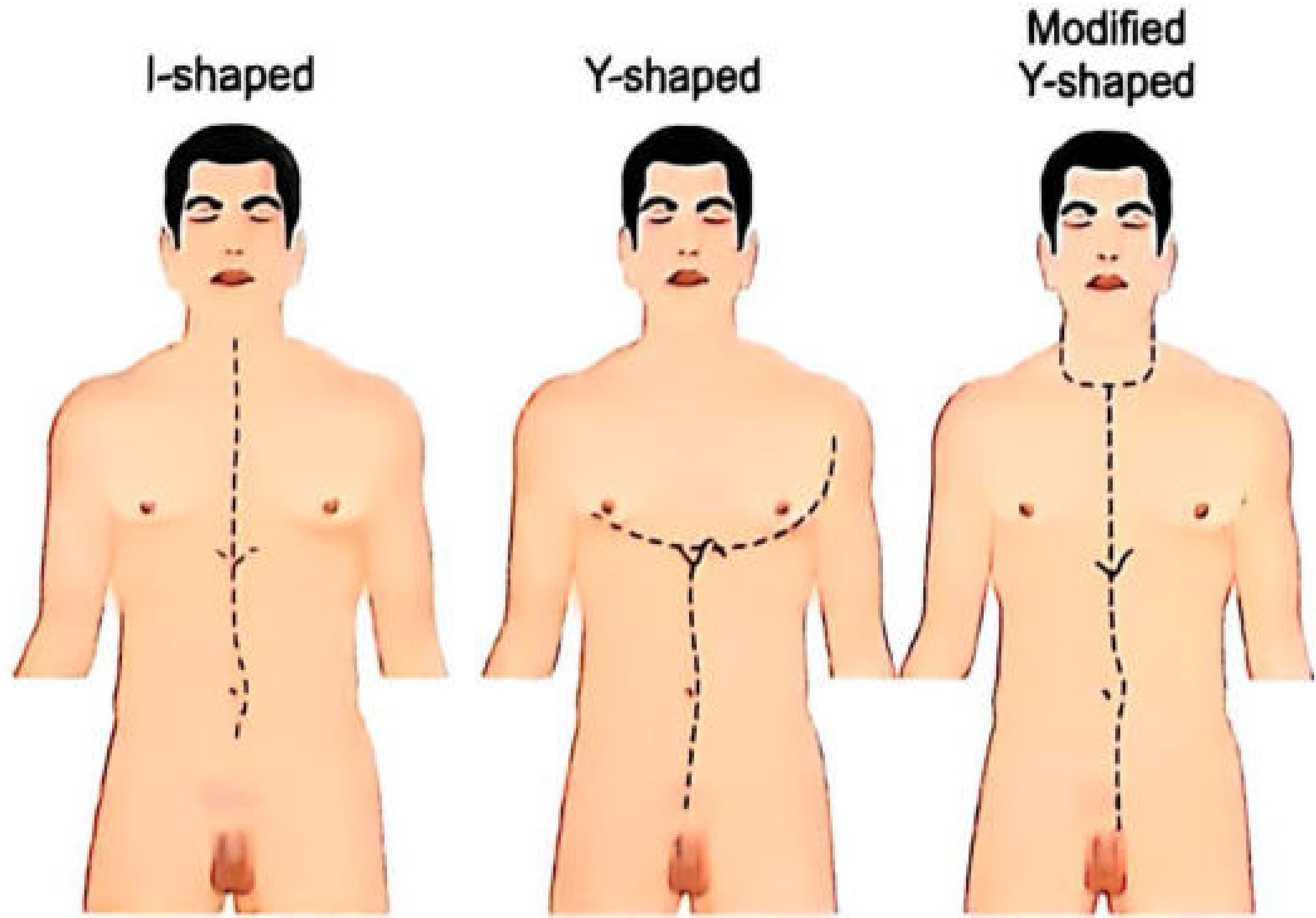
Fig: Primary skin incision types
-
"I" (T)-shaped Incision: Straight vertical incision from chin to symphysis pubis, passing left or right of the umbilicus. The umbilicus is avoided as dense fibrous tissue there makes re-suturing difficult.
-
"Y"-shaped Incision: Begins near the acromial process on each side, extends below the breast to the xiphoid process, then continues straight down to symphysis pubis.
-
Modified "Y"-shaped Incision: Midline from suprasternal notch to symphysis pubis, with bilateral extensions from the suprasternal notch over the clavicle, then up and behind the ear. Best for examining neck organs.
Note: Incisions must be adapted to the case - e.g., stab wounds may require the standard incision line to be altered to avoid disturbing the wound track.
4. Opening the Body Cavities
Abdomen
- The pathologist stands on the right side of the body (if right-handed).
- Recti muscles divided ~5 cm above symphysis pubis.
- A small cut is made in the fascia, fingers inserted in a V-shape to protect underlying structures, then peritoneum cut upward to xiphoid.
- Before disturbing anything: note blood, pus, or fluid (measure quantity), perforation of organs, adhesions, fat in mesentery/omentum, and height of diaphragm.
Neck Dissection
- A block (12-20 cm) placed under shoulders to extend the neck.
- Dissection carried immediately deep to skin through platysma.
- In asphyxial deaths (hanging, strangulation): open the skull first and remove the brain to drain blood from the neck, enabling dissection in a relatively bloodless field and preventing artifactual haemorrhages.
- Sternomastoid muscle freed from clavicular and sternal attachments and reflected on each side.
- Omohyoid, sternothyroid, thyrohyoid muscles exposed and reflected.
- Thyroid gland and carotid sheaths freed by blunt dissection.
- Larynx, trachea, pharynx, and esophagus mobilized and pulled away from prevertebral tissue.
Mouth/Tongue Removal
- Knife inserted under the chin through the floor of the mouth.
- Cut along sides of mandible to its angle - at the angle, blade is turned inward to avoid the carotid artery.
- Tongue pushed down under the mandibular arch; soft palate cut to include uvula, tonsils, tongue, and neck organs.
- Dissection carried distally through prevertebral muscles on the anterior cervical spine surface.
- Great vessels (carotids) divided in the neck.
Pneumothorax Detection (before opening chest)
Four methods:
- Dissect a pocket between chest wall and skin, fill with water, then puncture the wall under water - bubbling = pneumothorax.
- 16-gauge needle attached to water-filled 50 mL syringe (without plunger) introduced into intercostal space - bubbling confirms air.
- Remove intercostal muscle to expose parietal pleura - if pneumothorax is present, visceral pleura will not be visible immediately beneath it.
- Chest X-ray.
Chest (Thoracic Cavity)
- Chest muscles dissected away, knife directed inward toward ribs, carried to midaxillary line.
- Ribs, sternum, and spine examined for fractures.
- Chest opened by cutting costal cartilage with a cartilage knife, beginning at the upper border of the 2nd cartilage, close to costochondral junctions, knife inclined ~30° to vertical.
- In elderly (calcified cartilages): rib shears or handsaw used.
- Sternoclavicular joints disarticulated by inserting knife vertically into the semicircular joint and rotating.
- Diaphragm divided at its rib and sternal attachments up to the spine.
- In situ inspection before full organ removal includes:
- Lumen of main pulmonary vessels
- Right atrium and ventricle for air embolism
- State of lung distension or collapse
- Pleural cavities for blood, fluid, or adhesions
5. General Principles of Evisceration and Documentation
- The pathologist should use the technique with which they are most comfortable.
- All organs must be weighed and a brief description recorded. "Unremarkable" is acceptable for pancreas, adrenals, and spleen with no positive findings. "Normal" should not be used.
- Samples from all major organs should be saved; microscopic slides made when indicated (often not needed in forensic trauma cases).
- Samples for toxicological analysis should be noted separately.
- Articles removed from the body (clothing, jewelry, bullets) must be labelled, documented in the report, and handed to police in a sealed cover.
- Pacemakers must be removed before cremation (mercury batteries explode when burnt).
6. Special Considerations
- In suspected cranial injury: do not open the skull until blood has been drained by opening the heart first, to avoid artefactual findings.
- For air embolism suspicion: neck dissection must be modified to avoid injuring large neck veins before examination.
- For infectious deaths: Rokitansky's technique is preferred to contain spread.
Sources: The Essentials of Forensic Medicine and Toxicology, 36th edition (2026); PC Dikshit Textbook of Forensic Medicine and Toxicology
Provide diagram of each organ
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Generating Image
Generating Image
Generating Image
Generating Image
Provide general diagrams than
Generating Image
Generating Image
Generating Image
Generating Image
This is a shared conversation. Sign in to Orris to start your own chat.