Shigellosis
Reading File
Finding Sources
Searching PubMed
"shigellosis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Shigellosis
The Pathogen
Shigella spp. are gram-negative, nonmotile, facultatively anaerobic bacilli belonging to the family Enterobacteriaceae - closely related genetically to E. coli. There are four species, distinguished by their O-antigen:
| Species | Serotypes | Notable Features |
|---|---|---|
| S. dysenteriae | 15 | Most severe disease; serotype 1 produces Shiga toxin |
| S. flexneri | 15-19 | Dominant in low/middle-income countries; 66% of global isolates |
| S. sonnei | 1 | Dominant in high-income countries; mildest disease |
| S. boydii | 19 | Relatively uncommon; mostly South Asia |
- Medical Microbiology 9e, p. 1961-2004
Epidemiology
Shigella is a human-restricted pathogen - humans are the only reservoir.
-
Transmission: predominantly fecal-oral, via person-to-person contact, fomites, contaminated food/water, and increasingly as an STI (especially in MSM)
-
Extremely low infective dose: as few as 10 organisms for S. dysenteriae; 50-180 for other species - the lowest of any enteric pathogen
-
~80-165 million cases/year worldwide; ~150,000 deaths globally (GBD 2019), ~95,000 in children under 5
-
Second most common cause of diarrheal death worldwide, after rotavirus; most common bacterial cause
-
Accounts for 64% of dysentery cases attributable fraction
-
In the US: ~500,000 cases/year; S. sonnei causes ~75-80% of US cases
-
High-risk groups: children <5, elderly, residents of care homes/institutions, daycare attendees, MSM, travelers, immunocompromised patients
-
Goldman-Cecil Medicine, p. 2069-2075
Pathogenesis
The virulence mechanism is primarily invasion of colonic epithelium:
- Shigella is acid-resistant, allowing survival through the stomach at a very low inoculum
- Organisms are taken up by M (microfold) cells in the colonic epithelium (and ileal Peyer patches)
- After proliferating within M cells, bacteria escape into the lamina propria, where they are phagocytosed by macrophages and induce apoptosis
- The resultant inflammatory response damages surface epithelium, allowing Shigella in the lumen and lamina propria to access the basolateral surface of colonic epithelial cells - entry is far more efficient from the basolateral than the apical side
- All Shigella spp. carry virulence plasmids encoding a Type III secretion system that injects bacterial proteins directly into the host cytoplasm
- S. dysenteriae serotype 1 additionally produces Shiga toxin (Stx), which inhibits eukaryotic protein synthesis, causing host cell death and endothelial damage (mechanism for HUS)
- Robbins Pathologic Basis of Disease, p. 2916-2918
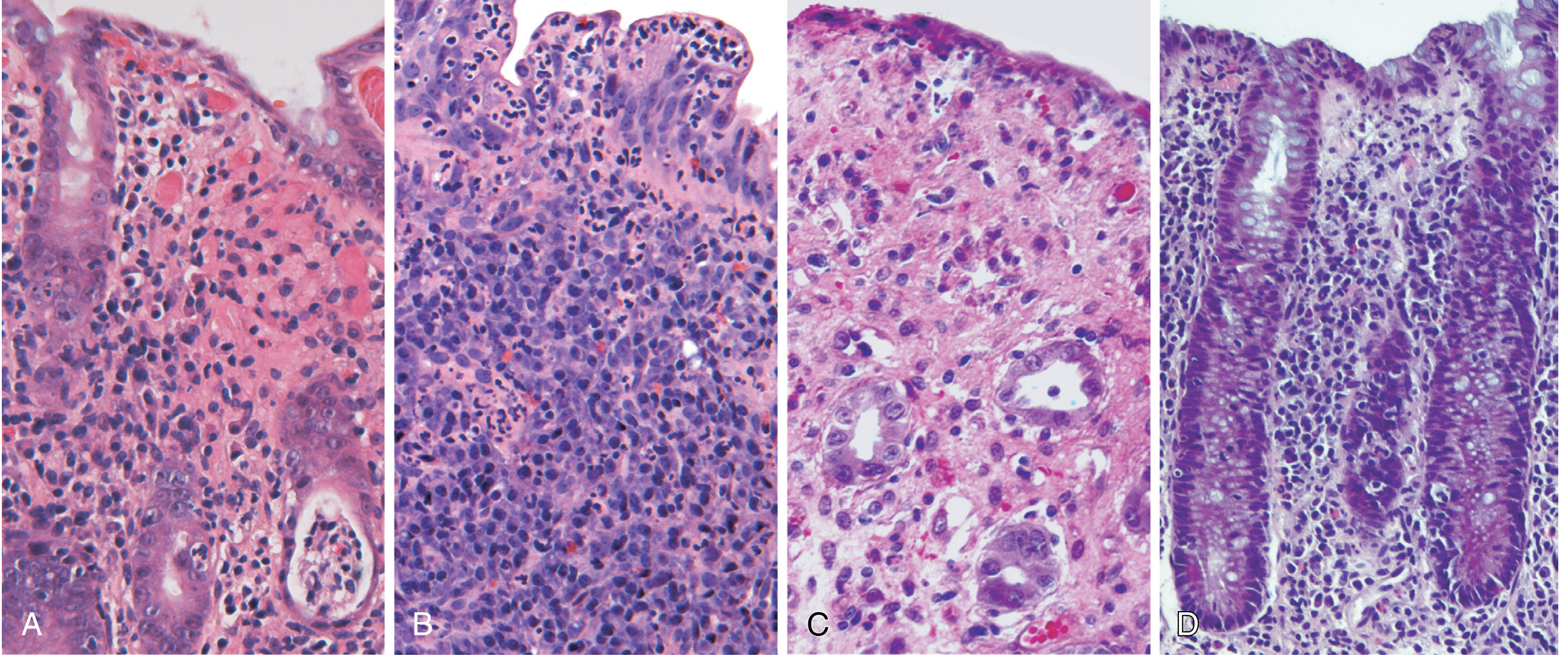
Morphology / Histopathology
- Most prominent in the left colon; ileum may also be involved (due to M-cell tropism over Peyer patches)
- Macroscopically: hemorrhagic, ulcerated mucosa; pseudomembranes may be present
- Histologically: early cases resemble acute self-limited colitis (e.g., Campylobacter colitis)
- Later: aphthous ulcers form over lymphoid follicles due to M-cell tropism
- Intraepithelial neutrophils are prominent (cryptitis/crypt abscesses)
The image below shows bacterial enterocolitis histology (panel A - Campylobacter is shown as an example of acute self-limited colitis):
Clinical Features
Incubation period: 24-48 hours (range 12 hours to 7 days)
The clinical course classically has two phases:
Phase 1 - Watery diarrhea (hours to 1-2 days):
- Crampy abdominal pain, fever, nausea/vomiting
- High-volume, non-bloody diarrhea
Phase 2 - Dysentery (in a subset):
- Low-volume, grossly bloody diarrhea with mucus
- Tenesmus (painful urge to defecate)
- Fever, headache, myalgias
- Severe dehydration and circulatory collapse if untreated
Species differences:
- S. sonnei: high-volume watery diarrhea, fewer systemic signs - typically milder
- S. flexneri, S. dysenteriae, S. boydii: more likely to cause frank dysentery with severe systemic symptoms
Neurologic manifestations (especially in children <2): seizures, lethargy, coma - may occur even without severe dehydration (Ekiri syndrome in its most lethal form)
- Rosen's Emergency Medicine, p. 1162-1165
Complications
| Complication | Associated Species / Notes |
|---|---|
| Hemolytic Uremic Syndrome (HUS) | S. dysenteriae type 1 (Shiga toxin); microangiopathic hemolytic anemia, thrombocytopenia, AKI |
| Reactive Arthritis | Post-infectious; especially after S. flexneri |
| Bacteremia/Sepsis | Rare, but more common in malnourished children and immunocompromised |
| Intestinal obstruction/toxic megacolon | Severe disease |
| Rectal prolapse | Children, due to straining |
| Hyponatremia | Especially in children, contributing to seizures |
| Protein-losing enteropathy | Chronic/recurrent infection |
Diagnosis
- Stool culture on selective media (e.g., MacConkey, XLD, Hektoen agar): >90% sensitivity in first 3 days; 75% after 1 week
- Multiplex PCR / NAATs (enteric panels): now considered the gold standard; detect Shigella directly and rapidly
- Stool microscopy: fecal leukocytes (WBCs in stool) are characteristic - useful screen
- Blood cultures: if bacteremia/sepsis is suspected
- Sigmoidoscopy: not routinely needed but shows friable, hyperemic, ulcerated mucosa
Treatment
1. Rehydration - the cornerstone of management
- Oral rehydration salts (ORS) for mild-moderate dehydration
- IV fluids for severe dehydration or inability to tolerate oral intake
2. Antibiotics - shorten clinical course, reduce fecal shedding, and are recommended for:
- All moderate-to-severe or dysenteric disease
- Immunocompromised patients
- Malnourished children
- Elderly patients
- Public health indications (food handlers, healthcare workers)
- Asymptomatic/recovering patients generally do not require antibiotics unless public health concerns apply
Empirical antibiotic choices (guided by susceptibility testing):
| Drug | Notes |
|---|---|
| Fluoroquinolones (ciprofloxacin) | First-line for adults in most settings; 3-5 days |
| Azithromycin | Preferred in children; also for fluoroquinolone-resistant strains |
| Trimethoprim-sulfamethoxazole (TMP-SMX) | Empirical option but high resistance rates in many regions |
| Ceftriaxone (IV) | For severe/complicated disease, S. dysenteriae outbreaks, or resistant strains |
| Pivmecillinam | Used in some settings for multidrug-resistant strains |
Antimicrobial resistance is a major and growing problem. Treatment should always be guided by local resistance patterns and in vitro susceptibility testing. Multidrug-resistant (MDR) and extensively drug-resistant (XDR) Shigella - particularly S. sonnei and S. flexneri - are increasingly reported globally.
3. Antipyretics: paracetamol/acetaminophen for fever
4. Avoid antidiarrheal agents (e.g., loperamide): contraindicated in dysentery - they may prolong fever, worsen disease, and increase risk of toxic megacolon
- Rosen's Emergency Medicine, p. 1175-1178; Goldman-Cecil Medicine, p. 2100-2115
Prevention and Control
- Handwashing with soap is the single most effective preventive measure
- Safe water supply and sanitation
- Proper food handling; isolating infected food-handlers
- Infection control in institutional settings
- No licensed vaccine is currently available - though several are in clinical development (this remains a major global health gap)
Key Summary Points
- Shigellosis is the most common cause of bacillary dysentery worldwide
- Very low infective dose (as few as 10 organisms) makes it highly contagious
- Pathogenesis is through colonic epithelial invasion via M cells and Type III secretion
- Classic presentation: fever + watery diarrhea progressing to bloody diarrhea + tenesmus
- S. dysenteriae type 1 produces Shiga toxin and can cause HUS
- Diagnosis: stool culture or NAAT (multiplex PCR)
- Treatment: rehydration + antibiotics (fluoroquinolones or azithromycin; guided by susceptibility)
- Growing antimicrobial resistance is a major global threat
What is shifellosis
I think you mean Shigellosis — I just covered this in detail above! Here's a concise summary:
Shigellosis - Quick Overview
Shigellosis is an infectious diarrheal disease caused by bacteria of the genus Shigella. It is the most common cause of bacillary dysentery worldwide.
What causes it?
- Gram-negative bacteria: Shigella sonnei (mildest, common in developed countries), S. flexneri (developing countries), S. dysenteriae (most severe), S. boydii
- Spread by fecal-oral route - person to person, contaminated food/water, or sexually (MSM)
- Extremely contagious - as few as 10 organisms can cause infection
What are the symptoms?
- Fever + crampy abdominal pain
- Starts as watery diarrhea, progresses to bloody diarrhea with mucus
- Tenesmus (painful urge to pass stool)
- Nausea, vomiting, headache
Who gets it?
- Children under 5 are most vulnerable
- People in crowded/poor-sanitation settings, daycare centers, nursing homes
How is it treated?
- Rehydration (ORS or IV fluids) - most important
- Antibiotics (ciprofloxacin or azithromycin) for moderate-severe cases
- Avoid anti-diarrheal drugs like loperamide
Key danger
- S. dysenteriae type 1 produces Shiga toxin, which can cause Hemolytic Uremic Syndrome (HUS) - kidney failure, anemia, low platelets
For the full detailed breakdown (pathogenesis, histology, complications, resistance), scroll up to my previous response!
This is a shared conversation. Sign in to Orris to start your own chat.