Differential diagnosis of atrophy of small muscles of hand
Differential Diagnosis of Atrophy of Small Muscles of the Hand
Patterns of Wasting and Their Significance
| Pattern | Primary Cause |
|---|---|
| Thenar wasting | Median nerve palsy (C8) |
| Hypothenar wasting | Ulnar nerve palsy (T1) |
| Intrinsic (all) wasting | Ulnar nerve palsy (T1) |
| Global intrinsic + both eminences | T1 root / brachial plexus / anterior horn cell |
- Bailey and Love's Short Practice of Surgery, Table 35.6
1. Peripheral Nerve Lesions (Most Common)
A. Ulnar Nerve Palsy
- Site of compression: Cubital tunnel (elbow) most common, or Guyon's canal (wrist)
- Muscles wasted: Hypothenar eminence, all interossei, medial two lumbricals, adductor pollicis
- Signs: Claw hand (ring & little fingers - "ulnar claw"), guttering on dorsum of hand, Froment's sign
- Causes: Elbow fracture/dislocation, prolonged compression, cubital tunnel syndrome, trauma
B. Median Nerve Palsy
- Site: Carpal tunnel (wrist) most common; also at elbow (anterior interosseous nerve, pronator teres syndrome)
- Muscles wasted: Thenar eminence (LOAF - lateral two lumbricals, opponens pollicis, abductor pollicis brevis, flexor pollicis brevis)
- Signs: Simian (ape) hand deformity, loss of thumb opposition, Tinel's and Phalen's signs in carpal tunnel syndrome
- Causes: Carpal tunnel syndrome (repetitive strain, pregnancy, hypothyroidism, acromegaly, rheumatoid arthritis), wrist fractures
C. Combined Median + Ulnar Nerve Lesion
- Affects all intrinsic muscles
- Causes: High wrist lacerations, combined entrapment, leprosy
2. Nerve Root / Spinal Cord Lesions
A. C8-T1 Nerve Root Compression
- Cause: Cervical spondylosis (C7-T1), disc prolapse, post-laminectomy
- All intrinsic muscles affected
- Associated sensory loss in C8-T1 dermatomal distribution (medial forearm, ring & little fingers)
B. T1 Root Lesion
- Classic cause of global wasting of all small muscles of the hand
- Due to: cervical rib, Pancoast tumor, apical lung carcinoma (Pancoast tumor invades the T1 root - a key surgical cause)
- Pancoast (superior sulcus) tumor - characterized by wasting of all intrinsics + Horner's syndrome (ptosis, miosis, anhidrosis) + shoulder/arm pain
C. Cervical Rib / Thoracic Outlet Syndrome
- Compresses lower brachial plexus (C8-T1 = lower trunk)
- Wasting predominantly in thenar eminence (median nerve territory more affected than ulnar in neurogenic TOS)
- Associated: subclavian artery compression, Adson's test positive
D. Brachial Plexus (Lower Trunk - Klumpke's Palsy)
- Lesion of C8-T1 lower trunk
- Wasting of all intrinsic muscles of hand + sensory loss over medial forearm + Horner's syndrome (if T1 root avulsion)
- Causes: Traction injury, birth trauma (Klumpke's), apical tumors
3. Anterior Horn Cell Disease
A. Amyotrophic Lateral Sclerosis (ALS) / Motor Neuron Disease
- Intrinsic hand wasting often an early presenting feature ("wasting of one hand")
- Characteristic combination of: LMN signs (wasting, fasciculations) + UMN signs (hyperreflexia, upgoing plantar)
- Fasciculations visible over the dorsum of the hand and tongue
- Progressive, bilateral - GOLDMAN-CECIL MEDICINE
B. Spinal Muscular Atrophy (SMA)
- Hereditary degeneration of anterior horn cells
- Distal wasting in SMA type III (Kugelberg-Welander)
C. Poliomyelitis
- Acute or post-polio syndrome
- Asymmetric, non-progressive after initial illness
- Residual wasting from anterior horn cell destruction
4. Spinal Cord Lesions
A. Syringomyelia
- Cavity in the central cord (typically cervical)
- Destroys anterior horn cells at the level of the cavity
- Presents with: cape distribution dissociated sensory loss (loss of pain and temperature but preserved touch/proprioception) + lower motor neuron wasting of hand muscles at the level of the lesion + upper motor neuron signs below
- Associated with Chiari malformation, trauma, tumors
B. Intramedullary Cervical Cord Tumor
- Ependymoma, astrocytoma
- Wasting + sensory disturbance at the level of the lesion
C. Cervical Myelopathy
- Chronic cervical spondylosis compressing the cord
- Wasting at the level of compression + spastic paraparesis below
5. Peripheral Neuropathies
A. Charcot-Marie-Tooth Disease (Hereditary Motor and Sensory Neuropathy)
- Genetic peripheral neuropathy
- Characteristically begins distally - "inverted champagne bottle" legs
- Hand intrinsics affected later in the course
- Autosomal dominant, most commonly PMP22 duplication
B. Leprosy
- Most common cause of peripheral neuropathy worldwide
- Ulnar and median nerve thickening + wasting
- Look for thickened nerves, trophic skin changes, anesthetic patches
C. Diabetic Peripheral Neuropathy
- Usually length-dependent, stocking-glove pattern
- Intrinsic hand wasting occurs in severe or diabetic amyotrophy
D. Vasculitic Neuropathy
- Mononeuritis multiplex → can affect ulnar/median nerves
6. Myopathic Causes
| Condition | Key Feature |
|---|---|
| Distal muscular dystrophies (Welander, Miyoshi) | Distal > proximal wasting |
| Myotonic dystrophy (DM1) | Thenar/hypothenar wasting + grip myotonia + ptosis + cataracts |
| Inclusion body myositis (IBM) | Finger flexor + quadriceps weakness; age >50 |
7. Disuse and Local Causes
- Disuse atrophy: Prolonged immobilization in a cast, complex regional pain syndrome (CRPS)
- Rheumatoid arthritis: Wasting from disuse, nerve entrapment, and joint destruction; compound palmar ganglion can compress the median nerve - S Das A Manual on Clinical Surgery
- Tuberculosis of wrist: Wasting of thenar and hypothenar muscles - S Das A Manual on Clinical Surgery
- Ischemia: Volkmann's ischemic contracture (post-compartment syndrome)
Quick Localization Summary
| Level | Key Features to Look For |
|---|---|
| Muscle | No sensory loss, may have myotonia, CK elevated |
| Peripheral nerve | Specific nerve territory sensory loss, Tinel's sign, nerve thickening in leprosy |
| Nerve root (C8-T1) | Dermatomal sensory loss, neck pain, radiological spondylosis |
| Brachial plexus | Horner's syndrome, subclavian bruit, trauma history |
| Anterior horn cell | Fasciculations, UMN signs (ALS), no sensory loss |
| Spinal cord | Dissociated sensory loss (syringomyelia), UMN signs below |
"CLEAN"
- C - Cervical rib / Cord (syringomyelia)
- L - Leprosy
- E - Entrapment neuropathy (combined median + ulnar)
- A - Amyotrophic lateral sclerosis / Apical lung tumor (Pancoast)
- N - Neuropathy (peripheral) / Nerve root (C8-T1)
Make a diagnostic flowchart: peripheral nerve vs. spinal vs. motor neuron disease
A clean, professional medical diagnostic flowchart titled "Differential Diagnosis of Small Muscle Hand Atrophy: Peripheral Nerve vs. Spinal Cord vs. Motor Neuron Disease". The flowchart starts at the top with a box: "Small Muscle Wasting of Hand" with an arrow pointing down to: "Are UMN signs present? (hyperreflexia, spasticity, upgoing plantar, clonus)" Two branches: - YES branch (right): leads to "UMN + LMN MIXED PATTERN" box, then arrow down to "Motor Neuron Disease (ALS)" with features listed: fasciculations, wasting, hyperreflexia, no sensory loss, tongue fasciculations - NO branch (left/center): "Pure LMN Pattern" leads to next question Next diamond: "Is there SENSORY LOSS?" YES branch → "Sensory Loss Present" → diamond: "What pattern of sensory loss?" - "Dermatomal (C8-T1) + neck pain" → "NERVE ROOT LESION" box: C8-T1 radiculopathy, cervical spondylosis, disc prolapse, Pancoast tumor - "Cape/dissociated (pain+temp lost, touch preserved)" → "SPINAL CORD - Syringomyelia" box: central cord cavity, associated Chiari, UMN signs below level - "Peripheral nerve territory (ulnar/median)" → "PERIPHERAL NERVE" box: Ulnar nerve palsy, Median nerve palsy, Carpal tunnel, Cubital tunnel, Leprosy - "Stocking-glove / length-dependent" → "PERIPHERAL NEUROPATHY" box: CMT, Diabetic, Vasculitic NO branch → "No Sensory Loss" → diamond: "Fasciculations present?" - YES → "ANTERIOR HORN CELL" box: Motor Neuron Disease/ALS, Poliomyelitis, SMA, progressive muscular atrophy - NO → diamond: "Myotonia / CK elevated?" - YES → "MYOPATHY" box: Myotonic dystrophy, Distal muscular dystrophy, IBM - NO → "DISUSE / LOCAL" box: Immobilization, CRPS, RA, Ischemia Color coding: peripheral nerve boxes in blue, spinal cord in green, motor neuron disease in red/orange, myopathy in purple. Clean white background, clear arrows, medical professional style, all text clearly readable.
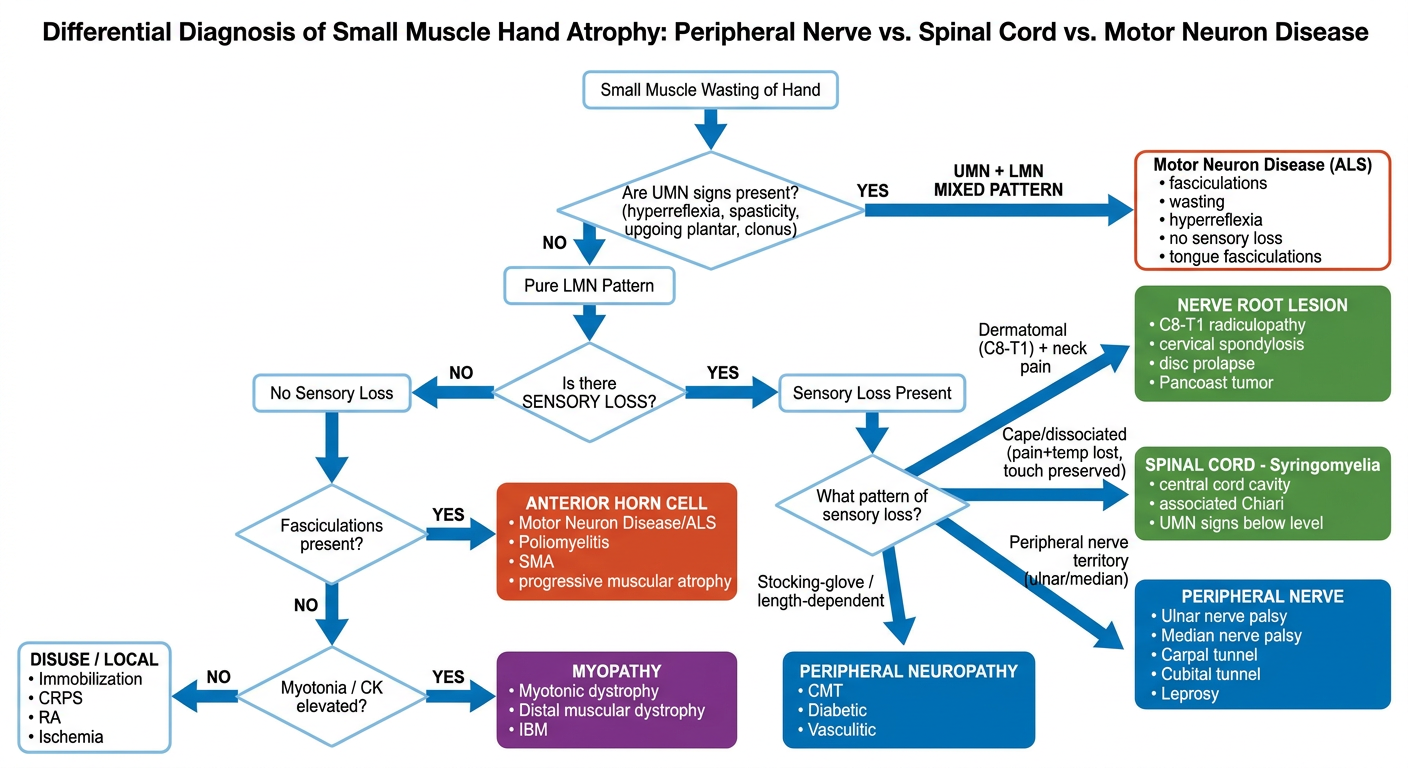
- Yes → Mixed UMN + LMN = Motor Neuron Disease (ALS) - the only condition that combines both upper and lower motor neuron signs with no sensory loss
- Yes → Narrow by pattern:
- Dermatomal (C8-T1) + neck pain → Nerve Root Lesion (cervical spondylosis, disc, Pancoast tumor)
- Cape/dissociated loss (pain & temp gone, touch preserved) → Syringomyelia (central cord cavity)
- Peripheral nerve territory (ulnar/median distribution) → Peripheral Nerve Palsy (cubital tunnel, carpal tunnel, leprosy)
- Stocking-glove / length-dependent → Peripheral Neuropathy (CMT, diabetic, vasculitic)
- No sensory loss → Proceed to Step 3
- Yes → Anterior Horn Cell disease (ALS/polio/SMA)
- No → Check for myotonia/elevated CK → Myopathy (myotonic dystrophy, IBM) or Disuse/Local cause (CRPS, RA, immobilization)
Pulmonary function test
Create a reference guide PDF on PFT interpretation