
fb05bb3a-eaae-482a-9630-984b2ab33847.jpeg
Tell me about this what is this it's etiology treatment prevention evrything
analyse_media
Reading File
Finding Sources
Searching PubMed
onychomycosis treatment antifungal
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information to give a thorough answer. Here it is:
Onychomycosis (Fungal Nail Infection / Tinea Unguium)
The image shows the classic features of Distal Subungual Onychomycosis (DLSO) - the most common type of fungal nail infection - with:
- Yellow-brown discoloration starting at the distal/lateral nail edge
- Onycholysis (nail plate separating from the nail bed)
- Subungual hyperkeratosis (chalky debris under the nail)
- Multiple fingers affected
This textbook image from Andrews' Diseases of the Skin shows the same condition for comparison:

Definition
Onychomycosis is fungal infection of the nail plate caused by dermatophytes, non-dermatophyte molds, or yeasts. It represents up to 30% of all superficial fungal infections and accounts for approximately 50% of all causes of nail dystrophy (onychodystrophy). The term "tinea unguium" strictly refers to dermatophyte nail infection only.
- Andrews' Diseases of the Skin, p. 351
Epidemiology
-
Affects up to 14% of the general population
-
More common in older individuals and increasing in children/adolescents
-
More common in men than women
-
Up to 40% of toenail onychomycosis patients have concurrent tinea pedis
-
Fitzpatrick's Dermatology, p. 2967
Etiology (Causative Organisms)
| Type | Most Common Pathogens |
|---|---|
| Distal-lateral subungual | Trichophyton rubrum (most common), T. interdigitale |
| Proximal subungual | T. rubrum, T. megninii |
| White superficial | T. interdigitale, Aspergillus, Scopulariopsis, Fusarium |
| Candida type | Candida albicans (usually in immunocompromised) |
| Non-dermatophyte molds | Aspergillus, Fusarium, Acremonium, Scopulariopsis brevicaulis |
In the United States (and South Asia), T. rubrum causes the vast majority of tinea pedis and onychomycosis. Infection typically begins as tinea pedis and extends to the nail bed, where eradication is far more difficult.
- Andrews' Diseases of the Skin, p. 351
Risk Factors
- Advanced age
- Male sex
- Nail trauma
- Immunosuppression (HIV/AIDS, diabetes mellitus, organ transplant)
- Peripheral vascular disease
- Wearing tight shoes / occlusive footwear
- Use of communal locker rooms, pools, showers
- Family members with onychomycosis (contagious)
HIV patients with CD4 < 400 cells/µL are at particularly high risk - PSO (proximal subungual type) can be a marker for HIV infection.
- Fitzpatrick's Dermatology, p. 2967
Clinical Types
1. Distal Lateral Subungual Onychomycosis (DLSO) - Most Common
- Invasion starts at the distal edge or lateral corner of the nail
- Whitish-to-brownish-yellow opacification at the distal nail edge
- Spreads proximally as a streak
- Leads to subungual hyperkeratosis, nail thickening, and eventual onycholysis
- This is what is shown in the uploaded image
2. White Superficial Onychomycosis (WSO)
- Direct invasion of the dorsal nail plate surface
- White, sharply bordered chalky patches on toenail surfaces
- Caused by T. interdigitale and non-dermatophyte molds
3. Proximal Subungual Onychomycosis (PSO)
- Fungus enters via the proximal nail fold
- White-to-beige opacity seen on the proximal nail plate
- Spreads distally; can destroy the entire nail
- Marker for HIV infection - screen all PSO patients
4. Candida Onychomycosis
- Massive nail destruction and hyperkeratosis
- Seen in chronic mucocutaneous candidiasis, other immunodeficiency states, and infants
5. Total Dystrophic Onychomycosis
-
End-stage disease; entire nail plate destroyed
-
Can result from progression of any of the above types
-
Fitzpatrick's Dermatology, p. 2967-2968; Andrews' Diseases of the Skin, p. 349-351
Diagnosis
A clinical diagnosis alone is not enough - up to 50% of dystrophic nails are not fungal. Confirmation is mandatory before starting systemic antifungals.
| Test | Sensitivity | Notes |
|---|---|---|
| KOH microscopy | Moderate | Rapid, in-office; identifies hyphae |
| Fungal culture | 30-70% | Gold standard for species ID; takes weeks |
| KOH + culture combined | 80-85% | Best of both |
| PAS histopathology | 41-93% | Most sensitive single test; results in 24 hours |
| PCR | Emerging | Highly sensitive and specific |
Samples should include subungual debris and nail clippings from the diseased area. A drilling technique may yield higher results than curettage.
- Andrews' Diseases of the Skin, p. 351
Differential Diagnosis
-
Nail psoriasis - pitting, oil-drop discoloration, salmon patches; skin/joint involvement
-
Lichen planus - rough nails, pterygium formation; oral/skin lesions
-
Eczema / contact dermatitis - affects adjacent nail fold
-
Traumatic onycholysis - history of injury
-
Yellow nail syndrome - all 20 nails, associated with lymphedema/pleural effusion
-
Norwegian (hyperkeratotic) scabies - generalized hyperkeratosis
-
Melanoma - must always rule out in pigmented nail changes
-
Andrews' Diseases of the Skin, p. 351
Treatment
Topical Therapy (mild/distal disease, contraindication to systemic)
| Agent | Cure Rate | Duration |
|---|---|---|
| Ciclopirox nail lacquer (8%) | ~70-77% in children; lower in adults | 48 weeks |
| Efinaconazole 10% solution | 15-17% complete; 55% mycologic | 48 weeks |
| Amorolfine nail lacquer | Moderate | 6-12 months |
Topical agents have lower side effects but significantly lower cure rates than oral therapy.
Systemic (Oral) Therapy - First Line for Most Cases
Terbinafine (drug of choice for dermatophytes):
- Adults: 250 mg/day for 6 weeks (fingernails) or 12 weeks (toenails)
- Children >40 kg: 250 mg/day; 20-40 kg: 125 mg/day; <20 kg: 62.5 mg/day
- Mycologic cure ~70% (toenails), ~80% (fingernails)
Itraconazole (pulse dosing):
- 200 mg twice daily for 1 week per month
- 2 months for fingernails; 3-4 months for toenails
- Good for Candida and non-dermatophyte molds too
Fluconazole:
- 150-300 mg once weekly for 6-12 months
- Comparable efficacy; convenient once-weekly dosing
Note: Griseofulvin is no longer standard therapy - prolonged course, low cure rates, high recurrence.
- Andrews' Diseases of the Skin, p. 351-352; Fitzpatrick's Dermatology, p. 2968-2969
Combination & Mechanical Approaches
- Combination topical + oral can improve clearance rates
- Nail trimming and debridement help deliver medication to the site
- Nd:YAG laser therapy: 50-60% cure rate after multiple sessions
- Surgical or chemical nail avulsion (40% urea) for refractory cases - a recent systematic review (Mycoses, 2025) confirmed 40% urea as an effective adjuvant to antifungals
For Candida Onychomycosis
- Itraconazole 400 mg/day pulse (1 week/month) for 4-12 weeks, OR
- Fluconazole 50 mg/day or 300 mg/week for similar duration
- Topical + systemic combination improves outcomes
Prevention and Recurrence
Recurrence rates are high (especially for toenails - up to 20-25% do not respond). Strategies to prevent recurrence and new infection:
- Keep feet clean and dry - dry between toes thoroughly after washing
- Wear breathable footwear - avoid tight, occlusive shoes
- Use antifungal powder or spray in shoes and socks
- Avoid walking barefoot in communal areas (pools, gym locker rooms, showers)
- Treat concomitant tinea pedis - it's a major reservoir for nail reinfection (30% of cases co-exist)
- Don't share nail clippers, files, or footwear
- Change socks daily; use moisture-wicking materials
- Topical antifungal lacquers after cure can be used as maintenance
- Manage systemic risk factors - optimal diabetes control, improve peripheral circulation
- Treat household contacts if infected
- Fitzpatrick's Dermatology, p. 2968-2969; Andrews' Diseases of the Skin, p. 351
When to Urgently Seek Care
- Diabetic patients or those with peripheral neuropathy: onychomycosis significantly increases risk of bacterial cellulitis - treat promptly
- Any suspicion of PSO (proximal white opacity under the nail): screen for HIV
- Spreading redness, warmth, swelling, or pus around the nail - possible secondary bacterial infection
Important Note
This is a clinical impression only. The nail changes in this image - particularly involving fingernails (rather than toenails) - can also be caused by psoriasis, which has nearly identical appearance. A KOH prep or PAS-stained nail clipping is needed to confirm the fungal etiology before starting systemic antifungals. Please see a dermatologist for proper testing and diagnosis.
Why there is hydrophobia after rabies
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have everything needed for a thorough, textbook-grounded explanation. Here it is:
Why Hydrophobia Occurs in Rabies
First, Understand the Virus's Path to the Brain
Before hydrophobia can be explained, you need to understand how the virus gets to the brainstem:
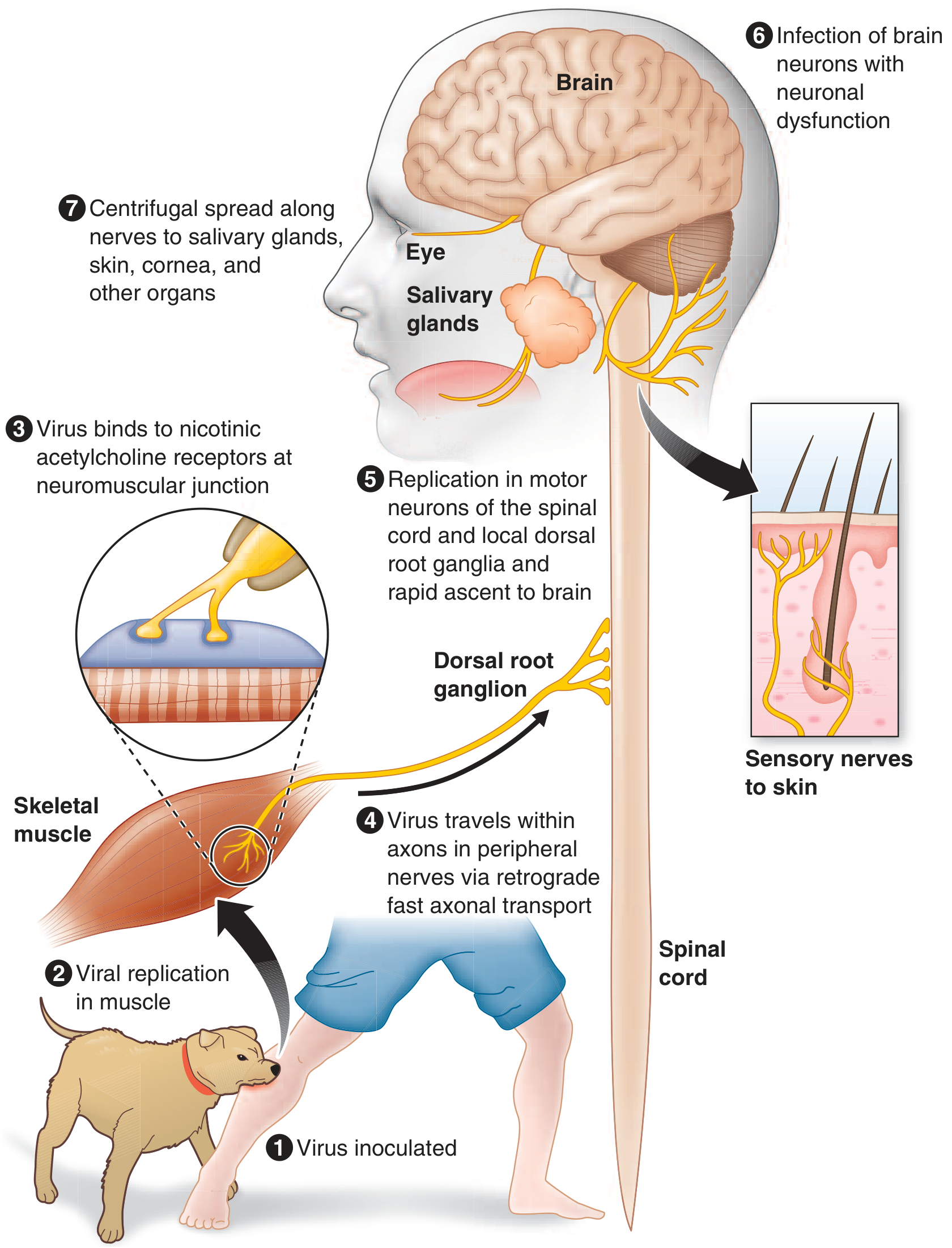
- The virus is inoculated via a bite into muscle/skin
- It replicates briefly in muscle, then binds to nicotinic acetylcholine receptors at the neuromuscular junction
- It enters peripheral nerve axons and travels centripetally (toward the CNS) via retrograde fast axonal transport at up to ~250 mm/day
- It replicates in spinal cord motor neurons and dorsal root ganglia, then ascends rapidly to the brain
- Once in the CNS it spreads widely via axonal connections - the brainstem and limbic system are particularly heavily infected
- After CNS infection is established, it spreads centrifugally back out to salivary glands, skin, cornea - this is why saliva is infectious
- Harrison's Principles of Internal Medicine 22e, p. 1695
The Core Mechanism of Hydrophobia
Hydrophobia is the result of early, prominent brainstem infection - specifically dysfunction of brainstem neurons that normally regulate swallowing and breathing.
Step-by-step breakdown:
1. Virus infects the brainstem - especially near the nucleus ambiguus
The nucleus ambiguus (in the medulla) controls the pharyngeal and laryngeal muscles used in swallowing. Nearby brainstem interneurons normally inhibit inspiratory neurons during swallowing - this is the protective reflex that prevents you from aspirating food or liquid into your airway.
When the rabies virus infects these brainstem neurons, it destroys the inhibitory control over inspiratory neurons. The result: swallowing can no longer suppress the inspiratory reflex properly.
2. Attempting to swallow water triggers violent spasms
When the patient tries to drink, the signal to swallow reaches a brainstem that has lost its normal inhibitory circuitry. This causes an exaggerated, involuntary, extremely painful spasm of:
- The diaphragm
- The pharyngeal muscles (throat)
- The laryngeal muscles (voice box)
- Accessory respiratory muscles
This lasts 1-5 minutes and is agonizing.
"Hydrophobia: involuntary, painful contraction of the diaphragm and accessory respiratory, laryngeal, and pharyngeal muscles in response to swallowing liquids... These symptoms are probably due to dysfunction of infected brainstem neurons that normally inhibit inspiratory neurons near the nucleus ambiguus, resulting in exaggerated defense reflexes that protect the respiratory tract."
- Harrison's Principles of Internal Medicine 22e
3. Classical conditioning creates the "phobia" component
After experiencing this terrifying spasm once or twice with water, the patient's brain forms a conditioned fear association. Now even:
- Seeing water
- Hearing water (splashing, running taps)
- Smelling it
- Or just being offered a drink
...all trigger anticipatory panic, spasm, and terror - even before the water touches the mouth. This is why it is literally called a "phobia" - the patient becomes genuinely terrified of water.
- Bradley and Daroff's Neurology in Clinical Practice, p. 1675
Aerophobia - The Same Mechanism
Closely related to hydrophobia is aerophobia - fear of drafts of air. A puff of air on the face triggers the same violent pharyngeal/laryngeal spasm. This is because the same dysfunctional brainstem defense reflex is activated by any stimulus to the respiratory tract area - not just liquid.
"Up to 80% of patients may exhibit hydrophobia or aerophobia, spasms of pharyngeal and nuchal muscles lasting from 1 to 5 minutes, triggered by swallow attempts or tactile, auditory, visual, and olfactory stimuli."
- Bradley and Daroff's Neurology in Clinical Practice
Why the Virus "Wants" This to Happen (Evolutionary Perspective)
This is actually advantageous for the virus. The same centrifugal spread that eventually causes the patient to develop hydrophobia also seeds the salivary glands with virus. The hydrophobia and pharyngeal spasms cause the patient to hypersalivate and be unable to swallow - meaning their mouth accumulates large quantities of virus-laden saliva. Combined with the behavioral changes (aggression, agitation) caused by limbic system infection, the virus maximizes its chance of being transmitted via a bite to a new host.
The Hypersalivation + Pharyngeal Dysfunction = "Foaming at the Mouth"
The combination of:
- Hypersalivation (from autonomic dysfunction - the virus infects the salivary glands and their autonomic supply)
- Pharyngeal paralysis/spasm (patient cannot swallow)
...produces the classic "foaming at the mouth" appearance, which is simply saliva that cannot be swallowed accumulating and frothing at the lips.
- Harrison's Principles of Internal Medicine 22e, p. 1695
Clinical Note - Hydrophobia as a Diagnostic Sign
In many developing countries, offering the patient a glass of water is used as a diagnostic test for rabies. The characteristic gagging, spasm, and terror on seeing water is so specific that it strongly confirms the diagnosis.
"The findings of hydrophobia with resultant gagging and hypersalivation are so characteristic of rabies infection that in many developing countries, water is offered to the patient as a diagnostic test."
- Rosen's Emergency Medicine
Summary Table
| Feature | Mechanism |
|---|---|
| Hydrophobia | Brainstem infection → loss of inhibitory control over inspiratory neurons near nucleus ambiguus → exaggerated airway-protective spasm on swallowing |
| Aerophobia | Same mechanism triggered by air draft instead of liquid |
| Foaming at the mouth | Hypersalivation + inability to swallow due to pharyngeal spasm |
| Fear of water (conditioned) | Classical conditioning after repeated painful spasm episodes |
| Hypersalivation | Virus infects salivary glands + autonomic dysfunction |
The bottom line: hydrophobia in rabies is not a psychological quirk - it is a direct, mechanistic consequence of the virus selectively destroying brainstem neurons that normally suppress the airway-protective reflex during swallowing. The "phobia" part is a learned conditioned response layered on top of this very real, very painful spasm.
This is a shared conversation. Sign in to Orris to start your own chat.