Hyperthyroidism pathophysiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Here it is:
Hyperthyroidism - Pathophysiology
Definition and Key Distinction
Hyperthyroidism refers specifically to excessive thyroid gland function, resulting in overproduction of thyroid hormones (T3 and T4). This should be distinguished from thyrotoxicosis, which is the broader state of thyroid hormone excess from any source (including exogenous intake or gland destruction). - Harrison's Principles of Internal Medicine 22E
Normal Thyroid Hormone Axis (Background)
To understand how hyperthyroidism arises, the normal axis must be clear:
- The hypothalamus releases TRH (thyrotropin-releasing hormone) → stimulates anterior pituitary thyrotrophs to secrete TSH
- TSH binds its receptor on follicular cells (via Gs protein → adenylyl cyclase → cAMP), stimulating every step of thyroid hormone synthesis: I⁻ uptake via Na/I symporter, oxidation by thyroid peroxidase (TPO), organification into monoiodotyrosine (MIT) and diiodotyrosine (DIT), coupling to form T3 and T4, and secretion via proteolysis of thyroglobulin
- Negative feedback: Free T3 (generated from T4 by 5'-deiodinase in pituitary thyrotrophs) down-regulates TRH receptors on thyrotrophs, suppressing further TSH release
-
99% of circulating thyroid hormones are protein-bound (to albumin, TBG); only free hormone is biologically active
Causes of Hyperthyroidism
| Category | Mechanism | TSH level |
|---|---|---|
| Graves' disease | TSH-receptor stimulating antibodies (TSI) | Low (feedback suppressed) |
| Toxic multinodular goiter | Autonomous nodule(s) secreting T3/T4 | Low |
| Toxic adenoma | Single autonomously functioning nodule | Low |
| TSH-secreting pituitary adenoma | Excess TSH drives thyroid | High |
| Activating TSH-R mutation | Constitutive receptor activation | Low |
| McCune-Albright syndrome | Activating Gα mutation | Low |
| Struma ovarii | Ectopic thyroid tissue in ovarian teratoma | Low |
| Iodine excess (Jod-Basedow) | Iodine load in susceptible gland | Low |
Harrison's Principles of Internal Medicine 22E, Costanzo Physiology 7th Edition
Graves' Disease - Primary Mechanism
Graves' disease accounts for 60-80% of thyrotoxicosis cases. It is an autoimmune disorder driven by:
1. Thyroid-Stimulating Immunoglobulins (TSI)
- IgG autoantibodies against the TSH receptor (TSH-R)
- TSI binds and activates the TSH receptor, mimicking TSH action - stimulating adenylyl cyclase → ↑cAMP → increased synthesis and secretion of T3/T4
- Present in ~90% of Graves' patients; almost never seen in other thyroid autoimmune diseases
- Simultaneously cause hypertrophy and hyperplasia of follicular cells (goiter)
- Because circulating T3/T4 are elevated, endogenous TSH is suppressed by negative feedback - TSH levels are low in Graves' disease even though the gland is maximally stimulated
2. TSH-R Blocking Antibodies
- A minority of patients also have blocking antibodies that compete at the TSH receptor
- Coexistence of stimulating and blocking antibodies can produce fluctuating states - explaining occasional intercurrent hypothyroid episodes in Graves' patients
Robbins & Kumar Basic Pathology, Robbins, Cotran & Kumar Pathologic Basis of Disease
Genetic susceptibility: Concordance in monozygotic twins is 20-40% (vs <5% in dizygotic). Key susceptibility genes include HLA-DR alleles, CTLA-4, CD25, CD40, PTPN22, FCRL3, CD226, and the TSHR gene itself. - Harrison's Principles of Internal Medicine 22E
Environmental triggers: Stress (neuroendocrine effects on immune system), smoking (major risk factor for ophthalmopathy), sudden iodine increase, postpartum period, immune reconstitution (e.g. after HAART or alemtuzumab).
Molecular Mechanism of Thyroid Hormone Action
In target tissues, T4 is converted to the active T3 by 5'-iodinase (5'-deiodinase). T3 then enters the nucleus, binds to nuclear thyroid hormone receptors, and the T3-receptor complex binds thyroid-response elements on DNA → gene transcription → new protein synthesis.
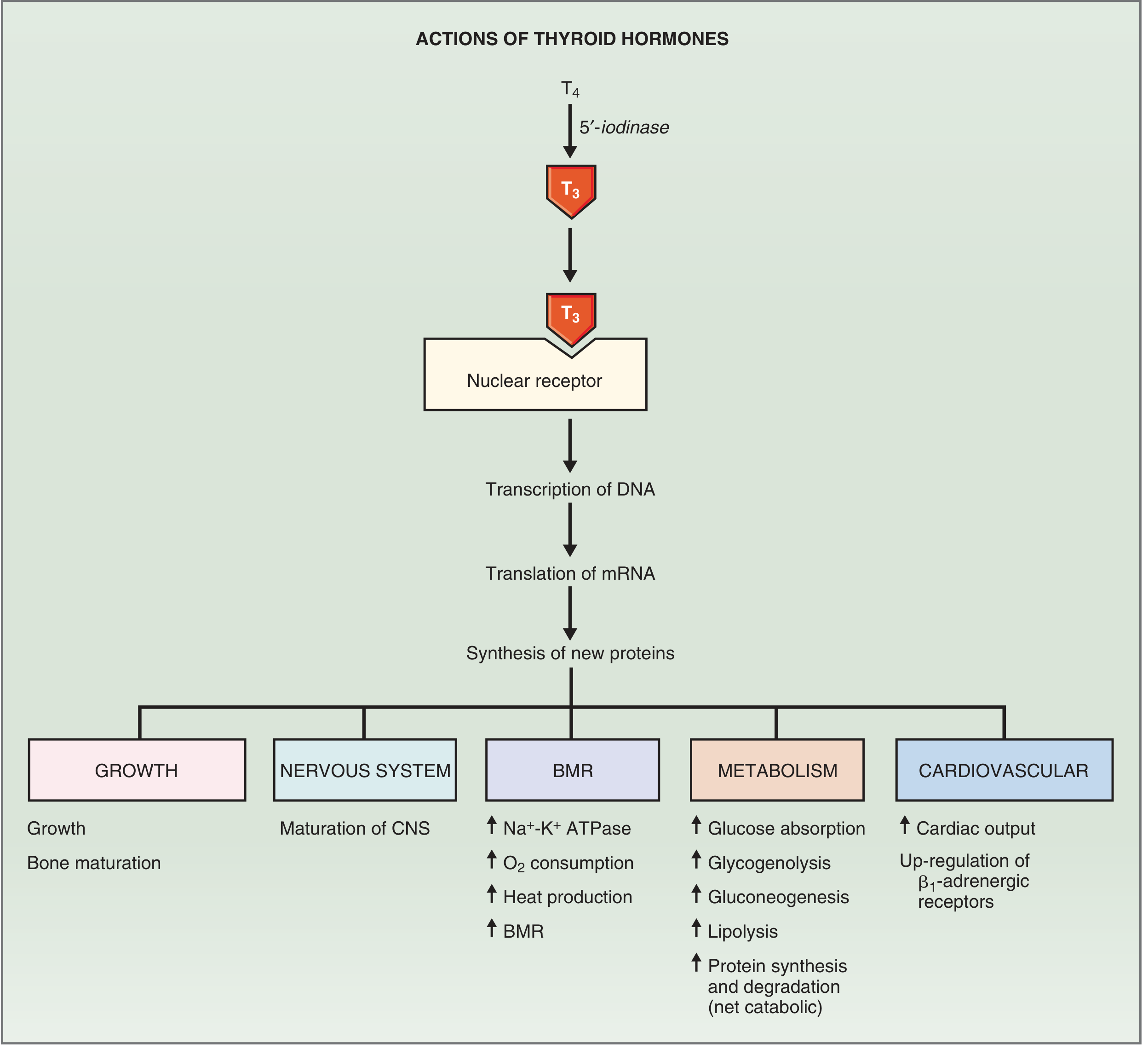
Key proteins induced by T3 include:
- Na⁺-K⁺ ATPase → increased O₂ consumption, BMR, heat production
- Myosin, β₁-adrenergic receptors, Ca²⁺ ATPase (cardiac) → increased heart rate and contractility
- Metabolic enzymes (liver, adipose) → altered carbohydrate, fat, protein metabolism
Organ-System Pathophysiology in Hyperthyroidism
| System | Mechanism | Clinical Features |
|---|---|---|
| Metabolic | ↑Na⁺-K⁺ ATPase → ↑BMR, ↑O₂ consumption | Weight loss despite increased appetite, heat intolerance, sweating |
| Cardiovascular | Up-regulation of β₁-adrenergic receptors → ↑HR and contractility; catecholamine sensitization | Palpitations, tachycardia, ↑cardiac output, AF, wide pulse pressure |
| Neuromuscular | Catecholamine excess interaction, increased protein catabolism | Tremor, muscle weakness, nervousness, anxiety |
| Bone/growth | Accelerated bone turnover | Osteoporosis with prolonged disease |
| Metabolic (catabolic) | ↑glycogenolysis, ↑gluconeogenesis, ↑lipolysis, net protein catabolism | Negative nitrogen balance, hyperglycemia tendency |
| GI | Increased gut motility | Diarrhea, increased frequency |
| Reproductive | Altered sex hormone-binding globulin | Menstrual irregularities in women |
Catecholamine sensitization is a key amplifier: thyroid hormones up-regulate β₁-adrenergic receptors, so even normal circulating catecholamine levels produce exaggerated responses. This is why β-blockers are effective adjunct therapy. - Katzung's Basic and Clinical Pharmacology, 16th Edition
Graves' Disease - Extrathyroidal Manifestations
Ophthalmopathy (Exophthalmos)
- TSH receptors are expressed not only in thyroid but also on orbital fibroblasts and fat cells
- Activated CD4+ T cells secrete cytokines (including PDGF and TGF-β) that stimulate fibroblast proliferation and synthesis of hydrophilic glycosaminoglycans (hyaluronic acid, chondroitin sulfate)
- This causes: (1) mononuclear cell infiltration of retro-orbital connective tissue, (2) edema and swelling of extraocular muscles, (3) GAG accumulation, (4) fatty infiltration (adipogenesis)
- Net result: increased retro-orbital volume → protrusion of the eyeball (exophthalmos), lid lag, impaired extraocular movement
Pretibial Dermopathy (Pretibial Myxedema)
- Deposition of glycosaminoglycans + lymphocytic infiltration in the dermis of the shins
- Presents as scaly thickening and induration of skin
Robbins, Cotran & Kumar Pathologic Basis of Disease, Robbins & Kumar Basic Pathology
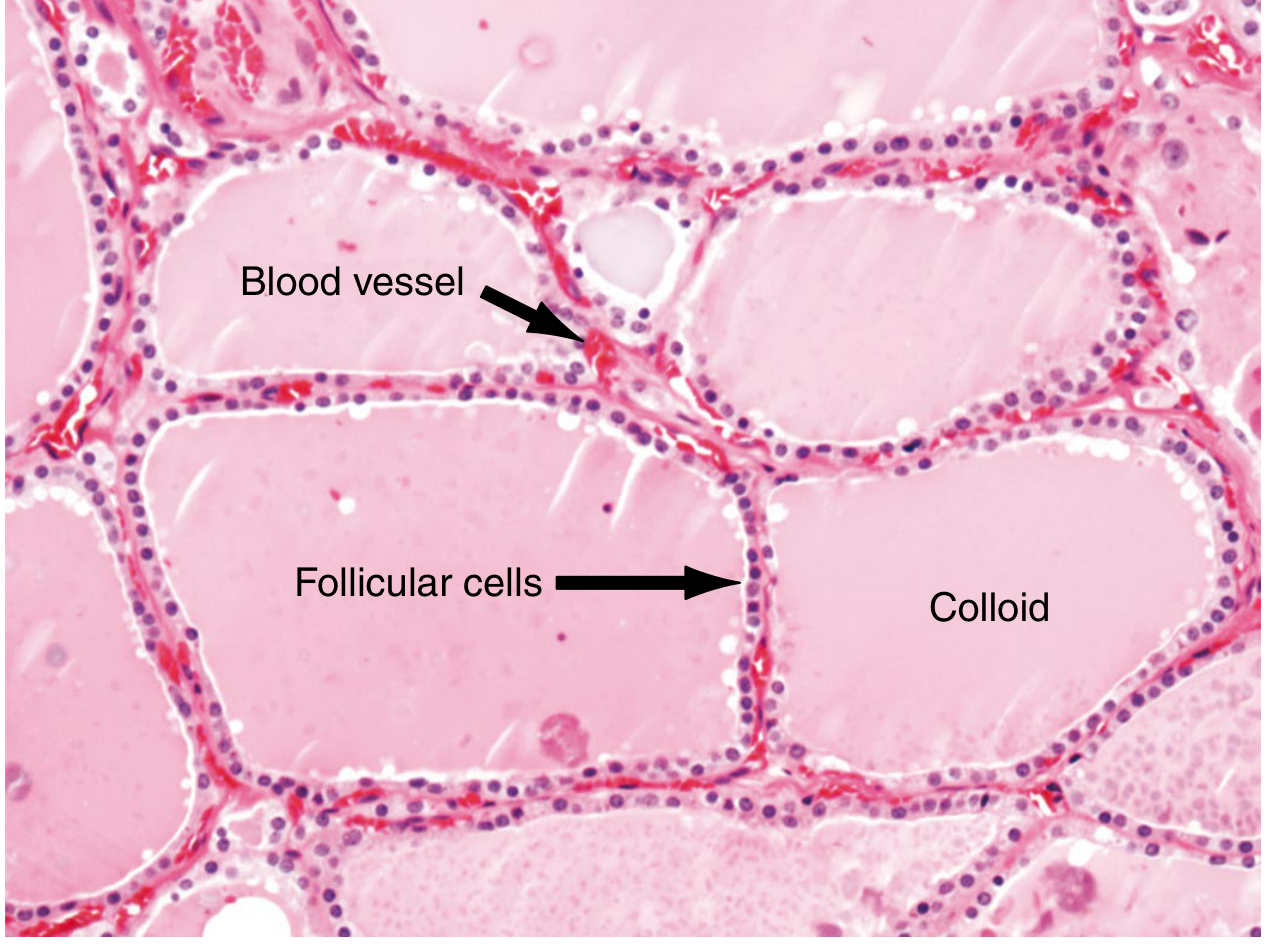
Gross and Histological Changes in Graves' Disease
- Diffuse symmetric goiter: gland can weigh >80g, soft and brown-red on cut section
- Histology: tall, crowded follicular epithelial cells forming small papillae projecting into follicular lumen (lacks fibrovascular cores - unlike papillary carcinoma)
- Colloid: pale with scalloped margins (indicates active resorption)
- Lymphoid infiltrates: T cells, B cells, plasma cells, often with germinal centers
- Increased thyroidal blood flow - audible bruit may be present
TSH Levels as a Diagnostic Key
| Cause | TSH level | Reasoning |
|---|---|---|
| Graves', toxic goiter, toxic adenoma, factitious | Low/suppressed | High T3/T4 → negative feedback suppresses pituitary TSH |
| TSH-secreting pituitary adenoma | High | Primary pituitary overproduction |
| Primary thyroid failure (e.g., Hashimoto's) | High | Loss of negative feedback on pituitary |
Costanzo Physiology 7th Edition
Sources: Costanzo Physiology 7th Edition | Robbins & Kumar Basic Pathology | Robbins, Cotran & Kumar Pathologic Basis of Disease | Harrison's Principles of Internal Medicine 22E | Katzung's Basic and Clinical Pharmacology 16th Edition | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.