My diognosis is absence of nitabisha fibrinoid layer Give me the features
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Here is a complete answer based on Creasy & Resnik's Maternal-Fetal Medicine:
Absence of Nitabuch's Fibrinoid Layer = Placenta Accreta Spectrum (PAS)
What is Nitabuch's Layer?
Nitabuch's fibrinoid layer is a band of fibrinoid material that forms the normal boundary between trophoblastic tissue and the maternal decidua basalis at the placental floor. In normal implantation, anchoring villi encroach on - but do NOT penetrate through - this membrane. It acts as a physiologic barrier that limits trophoblastic invasion.
Normal vs. Absent Nitabuch Layer (Histology)
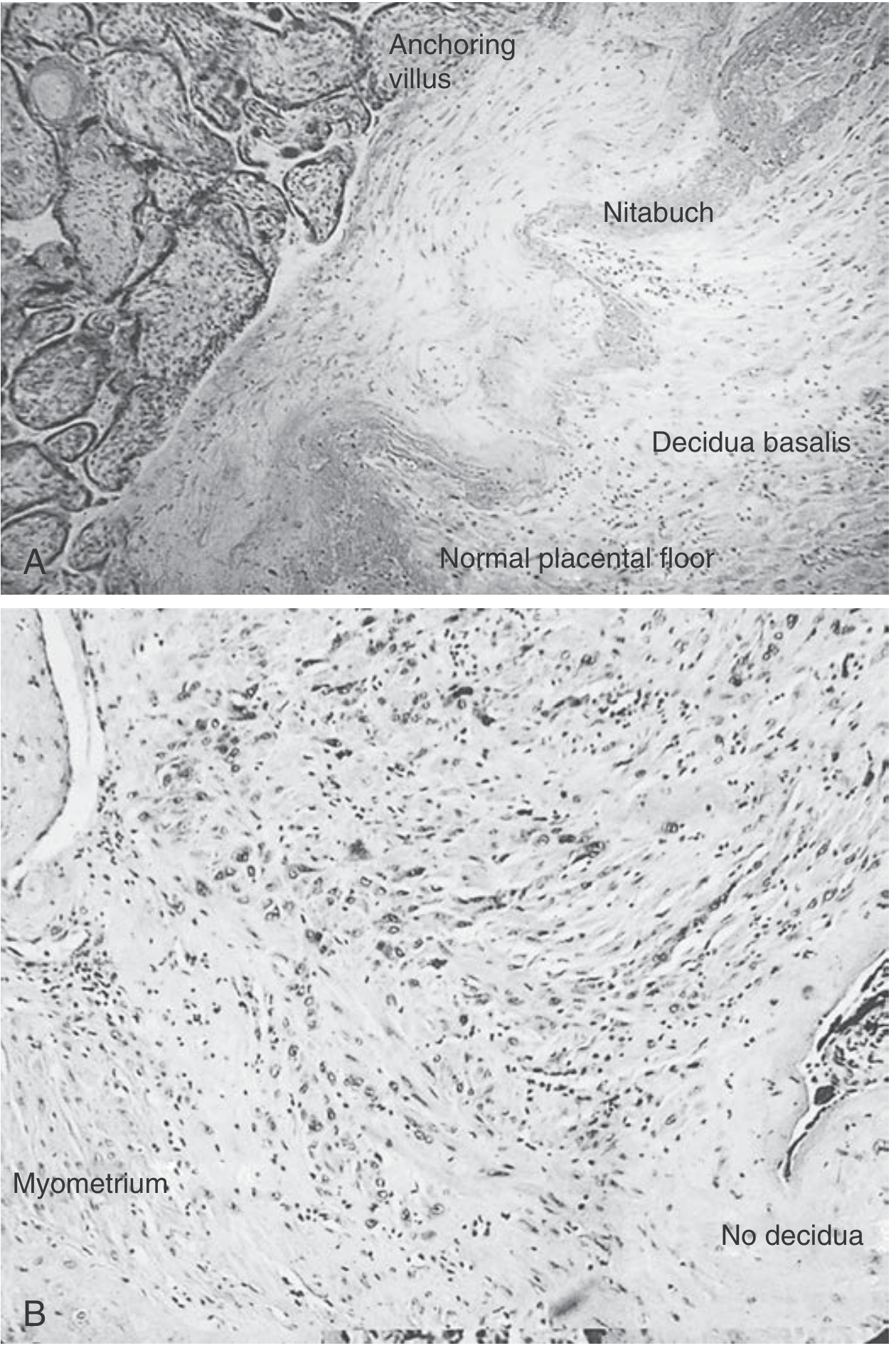
(A) Normal - Anchoring villi, Nitabuch membrane, and decidua basalis are all present at the placental floor.
(B) Placenta Accreta - No decidua, no Nitabuch layer; trophoblasts invade directly into myometrium.
Features of Absence of Nitabuch's Fibrinoid Layer
The absence of this layer defines the Placenta Accreta Spectrum (PAS), with three grades based on depth of invasion:
| Grade | Term | Feature |
|---|---|---|
| 1 | Placenta Accreta | Trophoblast attaches to myometrium with NO intervening decidua; invasion just beyond Nitabuch boundary |
| 2 | Placenta Increta | Invasion extends INTO the myometrium |
| 3 | Placenta Percreta | Invasion BEYOND uterine serosa (may involve bladder or other pelvic organs) |
Key Clinical & Pathological Features
Histology:
- No Nitabuch fibrinoid membrane visible
- No decidua basalis between villi and myometrium ("no decidua" sign)
- Trophoblasts in direct contact with or invading myometrial muscle fibers
Risk factors (why the layer is absent):
- Prior cesarean section - most common cause (risk >60% with previa + 3 or more cesareans)
- Placenta previa
- Other uterine surgeries: endometrial ablation, myomectomy, uterine curettage
- Pelvic radiation
- IVF, advanced maternal age, smoking, increased parity
Ultrasound features:
- Loss of normal hypoechoic boundary between placenta and bladder (represents absent myometrial/decidual layer)
- Intraplacental sonolucent spaces adjacent to uterine wall
- Turbulent flow and increased vascularity at the placenta-uterus interface on Doppler
- Obliteration of the well-delineated bladder wall
- Sensitivity ~55-90% depending on operator expertise
MRI features:
- Useful for posterior placenta or assessing deep myometrial/bladder involvement
- High accuracy for confirming diagnosis
- Gadolinium may improve detection but carries fetal risk
Clinical consequences:
- Failure of placenta to separate normally after delivery
- Massive intraoperative hemorrhage
- Most common indication for emergency peripartum hysterectomy
- High maternal morbidity
Management:
- Preferred treatment: planned cesarean delivery + hysterectomy (peripartum)
- Multidisciplinary team approach
- Pre-delivery diagnosis markedly reduces morbidity
- Planned delivery at 34-35 weeks after corticosteroid administration
- Conservative management (leaving placenta in situ) is possible in selected cases
Source: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Chapter 43 - Placenta Accreta Spectrum, p. 1021
This is a shared conversation. Sign in to Orris to start your own chat.