Gonococccal urethritis microbiology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Neisseria gonorrhoeae" AND urethritis
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive material. Let me compile the full answer.
Gonococcal Urethritis - Microbiology
The Organism
Neisseria gonorrhoeae (the gonococcus) is a Gram-negative, kidney-shaped (reniform) diplococcus - paired cocci with flattened adjacent surfaces. It is an obligate human pathogen; humans are the only natural reservoir.
Key microbiological properties:
- Gram-negative cell wall (outer membrane + thin peptidoglycan + cytoplasmic membrane)
- Aerobic, oxidase-positive, catalase-positive
- Fastidious growth: requires enriched media, optimal temperature 35-37°C, 5% CO2 atmosphere
- Ferments glucose only (not maltose, lactose, or sucrose) - this distinguishes it from N. meningitidis (ferments glucose and maltose) and other Neisseriae
- Antigenically heterogeneous and capable of rapid surface-structure variation
Antigenic Structure and Virulence Factors
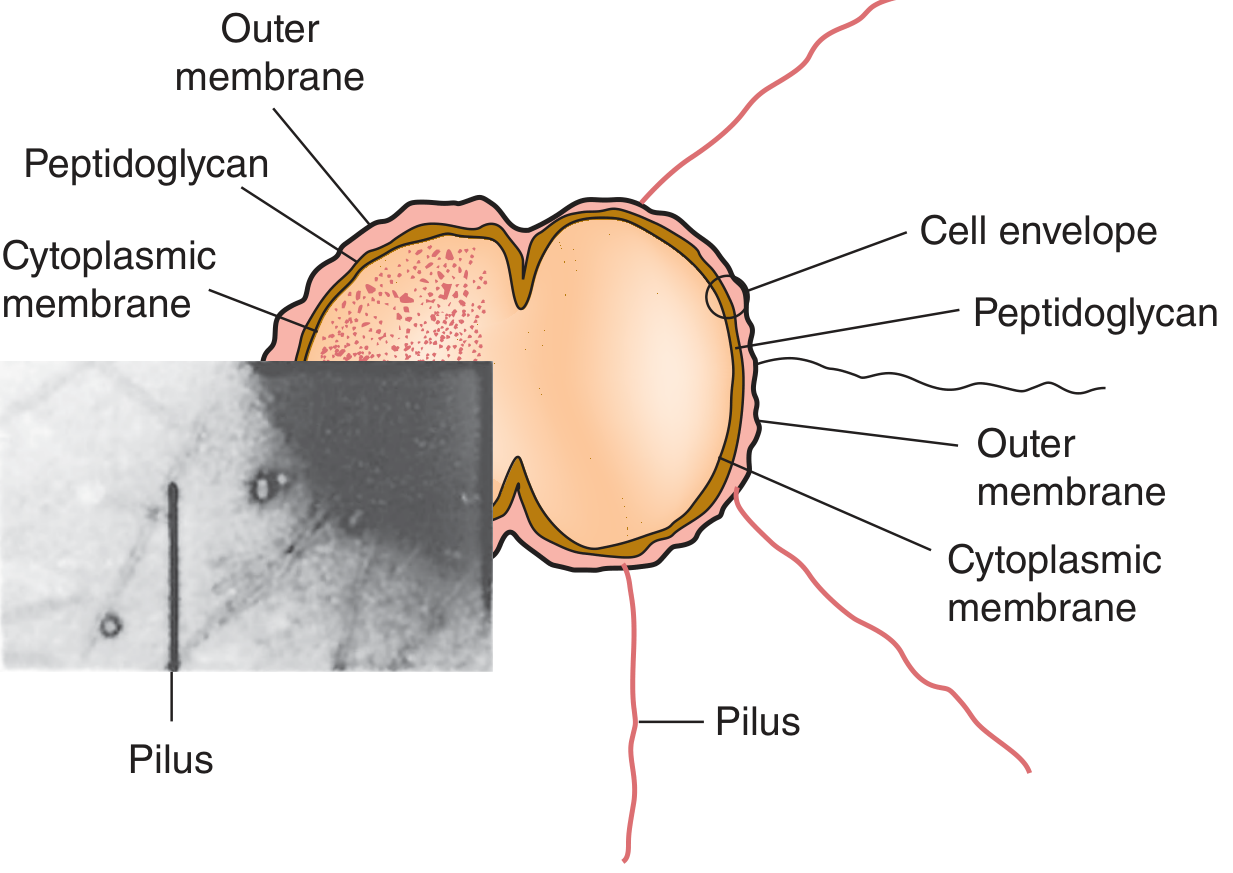
N. gonorrhoeae cell envelope showing the three-layered wall and surface pili (Jawetz Medical Microbiology, 28e)
1. Pili (Fimbriae)
- Hairlike appendages extending up to several micrometers from the surface
- Composed of stacked pilin proteins (MW 17-21 kDa)
- Functions: mediate attachment to host epithelial cells; confer resistance to phagocytosis
- The carboxyl-terminal region is highly variable antigenically - a single strain can express many antigenically distinct pilin forms, enabling immune evasion
- Piliated organisms produce small colonies on primary culture; on non-selective subculture, larger colonies of non-piliated organisms also appear
2. Por (Porin) Proteins
- Span the outer membrane; form pores for nutrient entry
- Prevent phagosome-lysosome fusion inside neutrophils (intracellular survival)
- Variable resistance to complement-mediated killing depends on Por binding to C3b and C4b
- Each strain expresses one of two Por types (PorB1a or PorB1b); antigenically diverse across strains
3. Opa Proteins (Opacity Proteins)
- Outer membrane proteins (MW 20-28 kDa) involved in adhesion to host cell receptors (heparin-related compounds, CD66/CEA-related cell adhesion molecules)
- Promote colony aggregation and epithelial cell invasion
- Each strain carries 11-12 opa genes; zero, one, two, or occasionally three types expressed simultaneously
- Associated with opaque colony morphology on primary culture
4. Rmp (Reduction-Modifiable Protein)
- Elicits antibodies that block bactericidal activity of antibodies directed against Por and LOS
- Contributes to immune evasion
5. Lipooligosaccharide (LOS)
- Gonococcal analogue of LPS (lacks the O-antigen polysaccharide side chain)
- Major mediator of local inflammation and tissue damage
- Antigenically variable; mimic host cell surface sugars
6. IgA Protease
- Cleaves secretory IgA1, the predominant mucosal antibody - neutralizes the host's first-line mucosal defense
7. Transferrin, Lactoferrin & Hemoglobin Receptors
- Outer membrane receptors that scavenge iron from host proteins - iron is essential for gonococcal survival and virulence
Pathogenesis of Urethritis
- Attachment - Pili and Opa proteins mediate adherence to non-ciliated columnar epithelium of the anterior urethra (ciliated cells are not the primary target)
- Invasion - Gonococci are taken up by epithelial cells via endocytosis; Por proteins inhibit phagolysosome fusion, promoting intracellular survival
- Submucosal spread - Organisms traverse epithelial cells and enter the subepithelial space, triggering intense PMN (neutrophil) infiltration
- Inflammation - LOS drives the brisk neutrophilic response; the pus formed consists largely of PMNs containing intracellular diplococci - the hallmark of gonococcal infection
- Incubation period: 3-14 days (most men symptomatic within 2-7 days)
Epidemiology
- Second most commonly reported communicable disease in the US (>555,000 cases/year reported; true incidence estimated at least twice that, ~78 million new cases worldwide annually)
- Highest rates in: ages 15-24, southeastern US, men who have sex with men (MSM)
- Disseminated gonococcal infection (DGI) risk is elevated in patients with terminal complement deficiencies (C5-C9)
- No protective immunity develops after infection due to antigenic variation - reinfection is common
Laboratory Diagnosis
Gram Stain
- Urethral smear showing PMNs with intracellular Gram-negative diplococci - diagnostic in symptomatic men (sensitivity ~95%, specificity ~99% in this group)
- Low sensitivity in women and in asymptomatic men; a negative Gram stain does not exclude infection
Culture
- Specimen immediately plated onto modified Thayer-Martin (MTM) medium (chocolate agar supplemented with vancomycin, colistin, nystatin, and trimethoprim to suppress normal flora)
- Incubated at 37°C in 5% CO2 for 48 hours
- Colonies identified by: Gram stain morphology + positive oxidase test + acid production from glucose only
- Confirmatory tests: chromogenic enzyme substrate tests, coagglutination, MALDI-TOF MS
- Culture is preferred over NAATs for: cases of suspected treatment failure, antimicrobial resistance monitoring, sexual assault in prepubescent children, and extragenital/rectal/oropharyngeal sites
Nucleic Acid Amplification Tests (NAATs)
- Now the preferred diagnostic method in most laboratories for genitourinary specimens
- Higher sensitivity than culture; can use first-void urine or urethral swabs
- Not FDA-cleared for rectal, oropharyngeal, or conjunctival specimens (culture required at these sites)
- Not suitable as test-of-cure (nucleic acid persists up to 3 weeks post-treatment)
Serology
- Not useful clinically due to: gonococcal antigenic heterogeneity, delayed antibody development, and high background seropositivity in sexually active populations
Biochemical Differentiation of Neisseriae
| Organism | Glucose | Maltose | Lactose | Sucrose | Growth on MTM |
|---|---|---|---|---|---|
| N. gonorrhoeae | + | - | - | - | + |
| N. meningitidis | + | + | - | - | + |
| N. lactamica | + | + | + | - | + |
| M. catarrhalis | - | - | - | - | - |
Antimicrobial Resistance (a key microbiological concern)
- Gonococci have developed resistance to: penicillin, tetracycline, fluoroquinolones (ciprofloxacin), and emerging resistance to cephalosporins and azithromycin
- Mechanisms include: plasmid-mediated beta-lactamase production, chromosomal mutations altering penicillin-binding proteins, efflux pumps (mtr locus)
- The CDC's Gonococcal Isolate Surveillance Project (GISP) has tracked resistance patterns since 1986
- Current first-line treatment: ceftriaxone 500 mg IM (single dose) - the dual therapy with azithromycin has been removed from the most recent CDC guidelines due to azithromycin resistance concerns
Key Distinguishing Points
- Only Neisseria that ferments glucose alone
- Requires enriched selective media (MTM) and CO2 for culture
- Antigenic variation (pili, Opa, Por, LOS) = no protective immunity, recurrent infection common
- Intracellular diplococci within PMNs on Gram stain = pathognomonic finding in symptomatic male urethritis
Sources: Jawetz Melnick & Adelberg's Medical Microbiology, 28e | Murray's Medical Microbiology, 9e | Campbell-Walsh-Wein Urology | Bailey & Love's Surgery, 28e
This is a shared conversation. Sign in to Orris to start your own chat.