Neck of femur changleys procedure
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching PubMed
Charnley total hip arthroplasty femoral neck fracture
Now I have enough information to provide a comprehensive answer. Let me compile the key content from the Schwartz's Surgery textbook, which covers the Charnley procedure (low friction arthroplasty) and hip arthroplasty for femoral neck fractures.
Charnley's Procedure for Neck of Femur (Hip Arthroplasty)
Background
Sir John Charnley revolutionized hip surgery, and the history of hip arthroplasty is divided into "Pre-Charnley" and "Post-Charnley" eras.
Before Charnley's contributions:
- Interpositional arthroplasty was used — tissue layers, plastic, or metal placed between worn articular surfaces. This frequently failed due to fracture of interposed material or component loosening.
- Austin-Moore prosthesis was introduced as an early stemmed component — replaced the femoral head and neck with a metal component secured into the femoral shaft via a diaphyseal stem. It was used for hemiarthroplasty for many years and served as a step toward total hip arthroplasty.
Charnley's Contribution — Low Friction Arthroplasty
Charnley's guiding principle was establishing a low-friction articulation — which remains the foundational goal of all modern hip arthroplasty. His key innovations:
- Small femoral head to minimize frictional torque
- High-density polyethylene acetabular cup (replacing earlier Teflon cups)
- Cemented fixation of both the femoral stem and acetabular component
- Medialisation of the acetabular component to reduce lever arm forces
This became known as the Charnley Low Friction Arthroplasty (LFA) — the prototype of modern total hip arthroplasty.
Types of Hip Arthroplasty for Femoral Neck Fractures
| Type | Description |
|---|---|
| Total Hip Arthroplasty (THA) | Replacement of both femoral head/neck and acetabulum |
| Hemiarthroplasty | Replacement of femoral head and neck with stemmed femoral component only; acetabulum not addressed |
For femoral neck fractures specifically:
- Hemiarthroplasty is the most common surgical option for displaced intracapsular fractures (subcapital fractures) in elderly patients
- The Austin-Moore and Thompson prostheses are classic unipolar hemiarthroplasty designs
- Bipolar hemiarthroplasty allows movement at both the prosthesis-head and prosthesis-acetabulum interfaces
Surgical Approaches
| Approach | Key Features |
|---|---|
| Anterior (Smith-Petersen) | Internervous/intermuscular; plane between femoral nerve and superior gluteal nerve; supine positioning; good for fluoroscopy use |
| Posterior (Kocher-Langenbach) | Muscle-splitting; no internervous plane; short external rotators released; best exposure for complex/revision cases |
| Lateral (Hardinge, 1982) | Anterior third of gluteus medius and minimus released from greater trochanter; risk of Trendelenburg gait |
| Anterolateral (Watson-Jones) | Intermuscular plane between gluteus medius and tensor fasciae lata |
Component Fixation
- Cemented fixation: Bone cement (PMMA) used to fix both the femoral stem and acetabular component. Standard in elderly patients with femoral neck fractures. Provides immediate stability.
- Cementless/press-fit fixation: Relies on osseointegration; more common in younger, active patients with good bone stock.
- Hybrid: Cemented femoral stem + cementless acetabular cup (most common combination for THA).
Bearing Surfaces
| Combination | Notes |
|---|---|
| Metal-on-polyethylene | Most common; cobalt-chrome or ceramic head on polyethylene liner |
| Ceramic-on-ceramic | Lowest friction of all; risk of fracture and squeaking |
| Metal-on-metal (MOM) | Largely abandoned — metal ion deposition, pseudotumors, early failure |
Alignment Principles (Charnley's Legacy)
Successful THA restores:
- Combined version of femoral and acetabular components
- Appropriate acetabular abduction (~40–45°)
- Medialization of the acetabular component to restore the centre of rotation
- Appropriate femoral offset and limb length
As Schwartz's notes: "staying true to Sir John Charnley's principles: establishing a low friction articulation."
Indications for THA vs. Hemiarthroplasty in Femoral Neck Fractures
| Factor | Favours Hemiarthroplasty | Favours THA |
|---|---|---|
| Activity level | Low | High |
| Pre-existing acetabular arthritis | No | Yes |
| Age | Very elderly (>80) | Younger elderly (65–80) |
| Cognitive function | Impaired (dementia) | Intact |
| Medical comorbidities | Multiple | Fewer |
Complications
- Dislocation — especially with posterior approach (posterior soft tissue repair reduces risk)
- Periprosthetic fracture — risk higher with anterior approach
- Aseptic loosening — most common long-term failure mode
- Periprosthetic joint infection
- Leg length discrepancy
- Heterotopic ossification — higher risk with lateral (Hardinge) approach
- Trendelenburg gait — abductor weakness, especially lateral approach
Sources: Schwartz's Principles of Surgery, 11th Ed.; Rockwood & Green's Fractures in Adults, 10th Ed.
Extracapsular neck of femur vs intra capsular neck of femur
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Now I have comprehensive content from multiple textbooks. Here is the full comparison:
Intracapsular vs. Extracapsular Neck of Femur Fractures
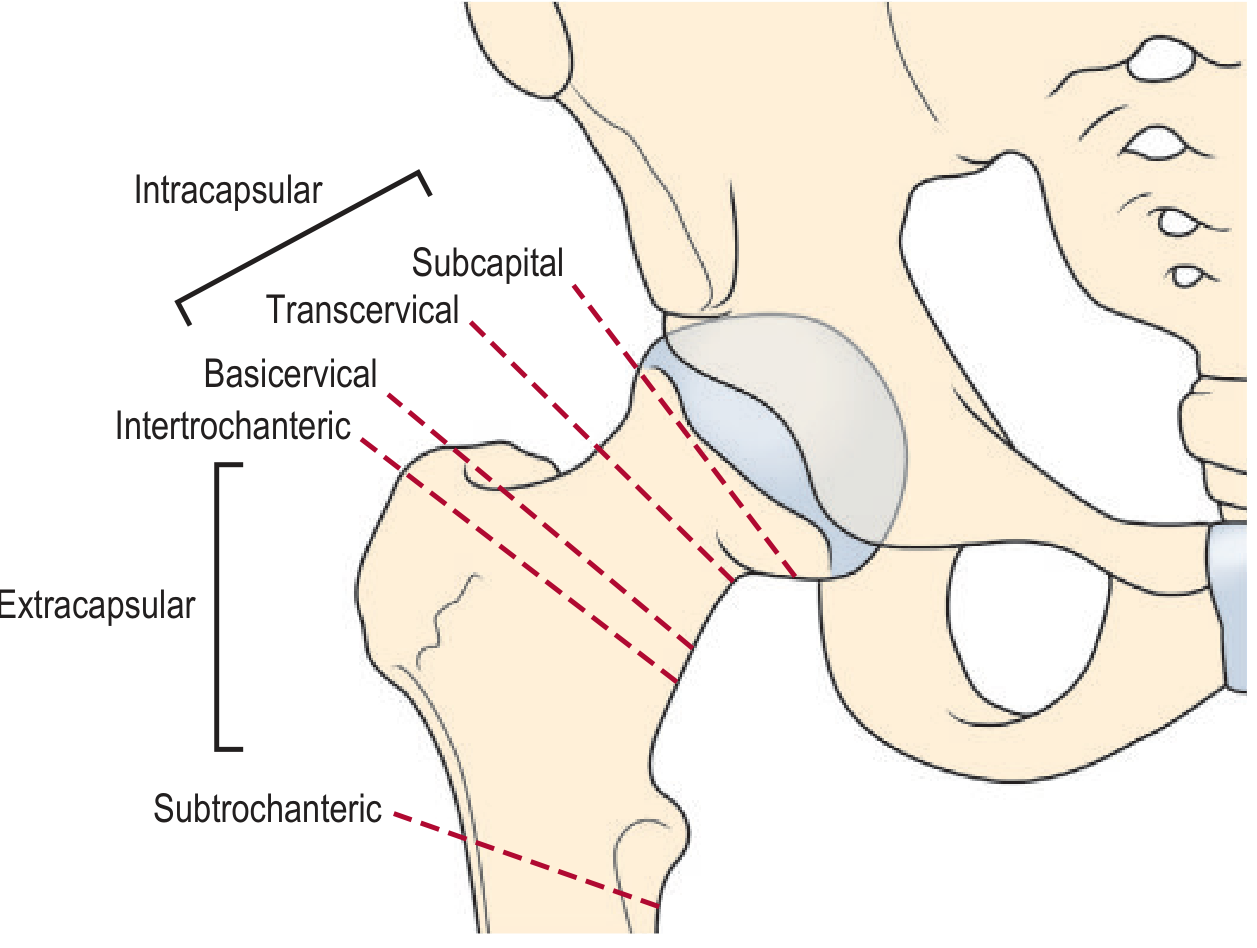
Anatomical Division
| Feature | Intracapsular | Extracapsular |
|---|---|---|
| Location | Within the hip joint capsule | Outside the hip joint capsule |
| Fracture sites | Subcapital, transcervical | Basicervical*, intertrochanteric, subtrochanteric |
| Relation to blood supply | Retinacular vessels run along the femoral neck inside the capsule — at high risk | Rich extracapsular arterial anastomosis — blood supply preserved |
*Basicervical fractures occupy a borderline zone — older classification systems called them extracapsular, but more recent systems consider them intracapsular (Rockwood & Green, 10th Ed.)
Blood Supply — Key Distinction
The blood supply to the femoral head comes from three sources (Rosen's Emergency Medicine):
- Ascending cervical (retinacular) arteries — branches of the medial circumflex femoral artery, run along the femoral neck within the capsule (most important, most vulnerable)
- Intramedullary (nutrient) arteries
- Foveal artery — within the ligamentum teres (minor contribution)
- Intracapsular fractures: Retinacular vessels are torn or kinked → high risk of avascular necrosis (AVN) of the femoral head (15–35% of displaced fractures)
- Extracapsular fractures: Fracture is distal to the capsular attachment → blood supply largely intact → AVN risk is very low
- Additionally, in intracapsular fractures, haemarthrosis raises intracapsular pressure, causing a tamponade effect further compromising femoral head perfusion.
Clinical Presentation
Both types present similarly, and cannot be reliably distinguished on clinical grounds alone (Rockwood & Green):
- Shortened, externally rotated leg
- Painful hip movements
- History of low-energy fall in elderly
Differences to note:
- Intracapsular: haemarthrosis may cause groin pain radiating to the knee; leg may appear less deformed in undisplaced fractures
- Extracapsular: typically more deformity and more obvious shortening due to pull of hip muscles
Classification Systems
Intracapsular — Garden Classification (1961)
Classified on the AP radiograph by the alignment of trabecular lines in the femoral head vs. acetabulum:
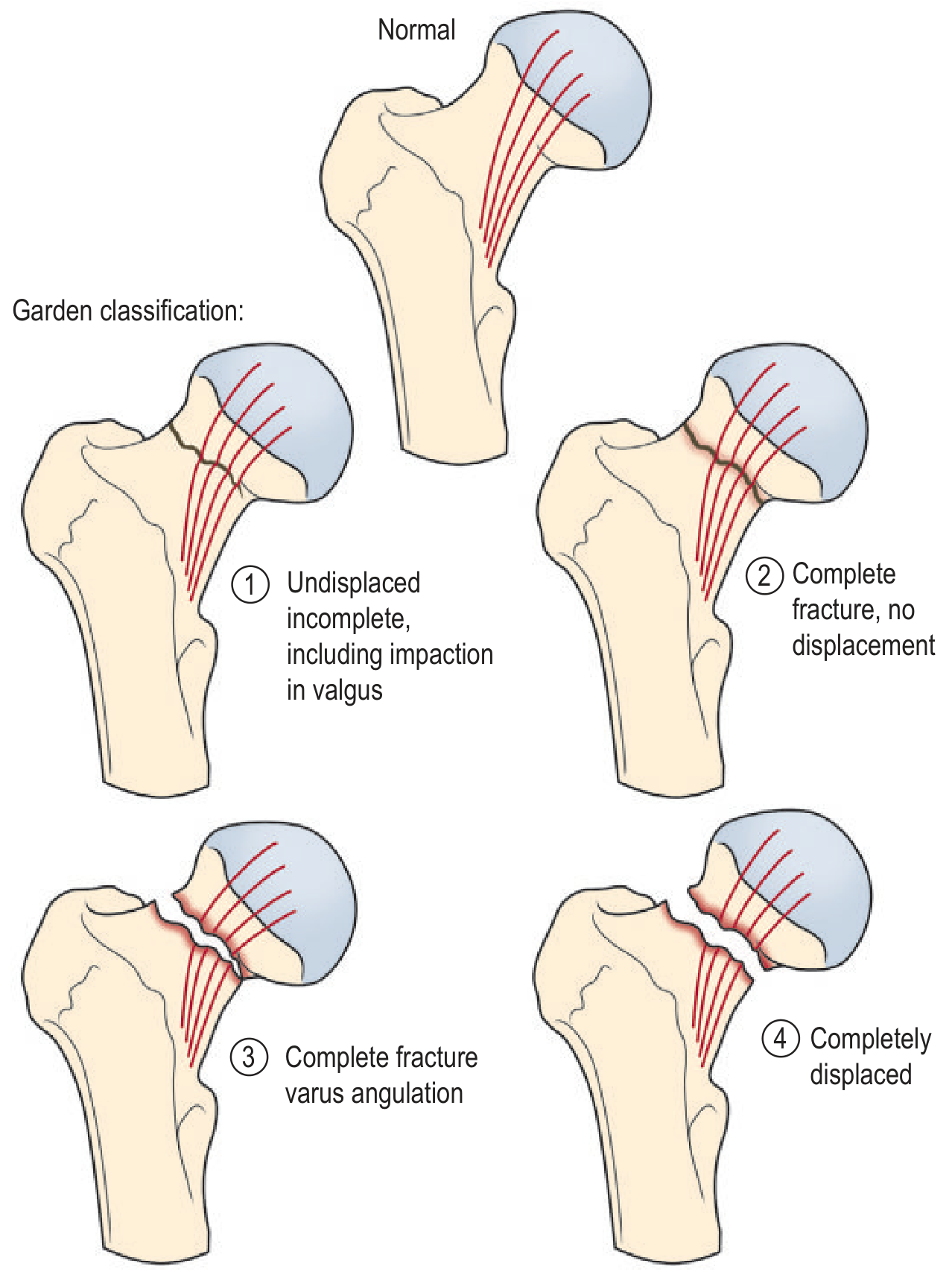
| Grade | Description |
|---|---|
| I | Incomplete/valgus-impacted; trabecular lines in head angled relative to acetabulum |
| II | Complete, undisplaced; trabecular lines collinear |
| III | Complete, partially displaced; varus angulation of trabecular lines |
| IV | Completely displaced |
Practical simplification: Clinically and prognostically, Garden I/II = undisplaced and Garden III/IV = displaced — the four-type system has poor inter-observer reliability (only 22% agreement across all grades).
Intracapsular — Pauwels Classification
Based on the angle of the fracture plane to horizontal:
- Type I: ≤30° (transverse) — most stable
- Type II: 30–50°
- Type III: >50° (vertical) — most unstable, highest risk of non-union and AVN
More relevant in younger patients with high-energy vertical fractures. Poor reliability in elderly patients where most fractures are near-transverse.
Extracapsular — Evans/Jensen Classification (Intertrochanteric)
Classified as stable vs. unstable based on integrity of the posteromedial cortex (lesser trochanter):
- Stable: Intact posteromedial cortex
- Unstable: Comminuted posteromedial cortex, reversed obliquity, or lateral wall fracture
Management
| Intracapsular | Extracapsular | |
|---|---|---|
| Goal | Restore blood supply / replace femoral head if AVN risk high | Internal fixation — bone heals reliably |
| Undisplaced (Garden I/II) | Internal fixation with cannulated screws or dynamic hip screw | Internal fixation |
| Displaced (Garden III/IV) — elderly | Hemiarthroplasty (Austin-Moore / cemented Thompson prosthesis) or Total Hip Arthroplasty in active, cognitively intact patients | Dynamic Hip Screw (DHS) or Intramedullary nail (cephalomedullary nail) for unstable patterns |
| Displaced — young (<60 yrs) | Urgent reduction and internal fixation (attempt head preservation) | Internal fixation |
| Non-ambulatory patient | Conservative management may be considered | Conservative may be acceptable |
Why fixation fails for displaced intracapsular fractures: Avascular femoral head cannot heal reliably → high rates of non-union and AVN with screws → arthroplasty preferred in elderly.
Why intertrochanteric fractures do NOT need arthroplasty routinely: Extracapsular location preserves blood supply → bone heals → internal fixation works.
Complications Summary
| Complication | Intracapsular | Extracapsular |
|---|---|---|
| Avascular necrosis | ✅ Major risk (15–35%) | ✗ Rare |
| Non-union | ✅ Common in displaced | Less common |
| Shortening/malunion | Present | Present |
| Implant failure/cut-out | If fixed | If fixed (especially unstable patterns) |
| Periprosthetic fracture | If arthroplasty used | — |
| DVT/PE | Both types | Both types |
| Mortality (1-year) | ~20–30% in elderly | ~20–30% in elderly |
Sources: Rockwood & Green's Fractures in Adults, 10th Ed. | Grainger & Allison's Diagnostic Radiology | Rosen's Emergency Medicine | Pfenninger & Fowler's Procedures for Primary Care, 3rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.