Explain the hemorrhage in detail according to surgery book Definition, Etiology, pathogenesis in flow chart, classification, clinical features, diagnosis, treatment, complications
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have all the content needed. Let me compile the comprehensive, well-structured answer.
HEMORRHAGE - A Surgical Perspective
Sources: Schwartz's Principles of Surgery 11th Ed., Sabiston Textbook of Surgery, Forensic Medicine & Toxicology 36th Ed.
1. DEFINITION
Hemorrhage is the escape (effusion) of blood from the confines of the vascular system - arteries, veins, or capillaries - into surrounding tissues, body cavities, or to the exterior. The term is commonly applied to any clinically significant blood loss, and specifically to cerebral hemorrhage when blood collects within an organ.
In surgical practice, hemorrhage is the most common cause of shock in the surgical or trauma patient, and loss of approximately one-third of the circulating blood volume (roughly 1.5-2 L in an adult) causes irreversible hypovolemic shock and death if untreated.
2. ETIOLOGY
A. Traumatic
- Penetrating injuries (stab wounds, gunshot wounds)
- Blunt trauma with organ laceration (liver, spleen, kidney)
- Fractures (pelvic fractures - major cause of retroperitoneal hemorrhage; long bone fractures)
- Surgical/iatrogenic injury to major vessels
B. Spontaneous / Pathological
- Vessel wall disease: Atherosclerosis, aneurysm rupture, vasculitis, Marfan syndrome
- Coagulation disorders: Hemophilia A & B, von Willebrand disease, thrombocytopenia (ITP, DIC)
- Anticoagulant therapy: Warfarin, heparin, DOACs, aspirin, NSAIDs
- Infections: Erosion of vessel walls by septic processes (mycotic aneurysm, abscess)
- Neoplasms: Tumor invasion of vessels
- Peptic ulcer disease: Erosion into gastroduodenal/left gastric artery
- Esophageal varices: Portal hypertension
- Aortoenteric fistula
- Hemorrhagic diathesis / haemophilia - even minor injuries can be fatal
C. Factors That Worsen Hemorrhage
- Rise in blood pressure during recovery from shock
- Muscular movements loosening a blood clot
- Sepsis causing erosion of vessel walls
- Partial transection of an artery (retraction cannot occur, so bleeding is greater than with complete transection)
3. PATHOGENESIS - FLOW CHART
BLOOD LOSS FROM VASCULAR COMPARTMENT
|
v
DECREASED CIRCULATING BLOOD VOLUME
|
________|________
| |
v v
BARORECEPTOR CHEMORECEPTOR
ACTIVATION STIMULATION
(aortic arch, (hypoxia, acidosis,
carotid bodies) CO2 changes)
| |
|_________________|
|
v
SYMPATHETIC NERVOUS SYSTEM ACTIVATION
+ Hypothalamic-Pituitary-Adrenal Axis
|
_______|_______
| | |
v v v
Catecho- Renin- Vasopressin
lamines Angiotensin Release
Released Cascade
| | |
|_______|_______|
|
v
PERIPHERAL VASOCONSTRICTION
+ Increased Heart Rate & Contractility
+ Fluid Retention (oliguria)
+ Blood Flow Preferentially to Heart & Brain
|
v
[IF HEMORRHAGE CONTINUES / EXCEEDS COMPENSATION]
|
v
DECREASED TISSUE PERFUSION
/ | \ \
v v v v
Parenchymal Endothelial Cellular Metabolic
Cell Injury Activation/ Hypoxia Acidosis
Microvascular
Damage
| |
v v
Cellular Intracellular
Aggregation Fluid Loss +
↓ Coronary
Perfusion
\___________/
|
v
↓ VENOUS RETURN
|
v
FURTHER ↓ TISSUE PERFUSION
(VICIOUS CYCLE OF SHOCK)
|
v
IRREVERSIBLE SHOCK
(Multi-Organ Failure, Death)
The Vicious Cycle of Shock (from Schwartz's Surgery):
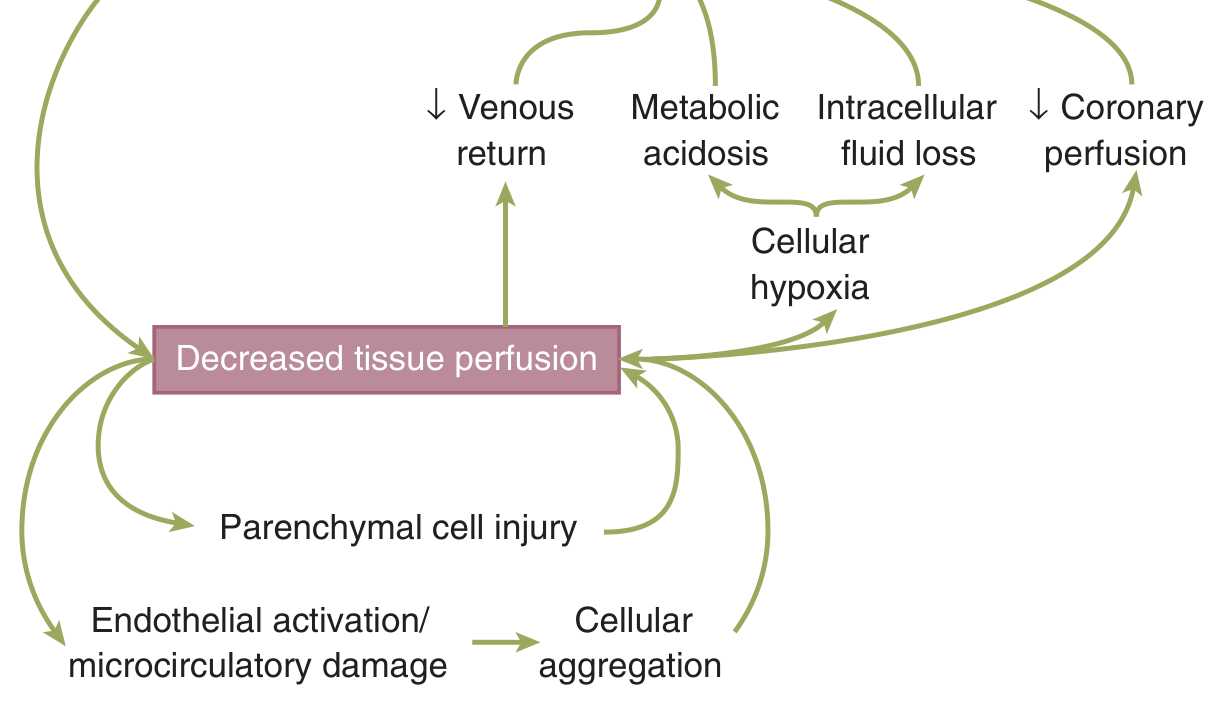
Regardless of etiology, decreased tissue perfusion creates a feed-forward loop that exacerbates cellular injury and tissue dysfunction. Schwartz's Principles of Surgery, Fig. 5-2.
Neuroendocrine Response in Detail:
- The goal is to maintain perfusion to heart and brain at the expense of other organs
- Initial stimulus: loss of circulating blood volume
- Magnitude: proportional to both the volume and rate of blood lost
- Afferent signals from baroreceptors, chemoreceptors, and pain receptors converge in the CNS
- Efferent response: expands plasma volume, maintains peripheral perfusion, restores homeostasis
4. CLASSIFICATION
A. By Timing (Clinical Classification - Bailey & Love / Surgical Tradition)
| Type | Timing | Mechanism |
|---|---|---|
| Primary | At the time of injury | Direct vascular disruption |
| Reactionary (Secondary) | Within 24 hours (usually a few hours post-injury) | Rise in BP during recovery from shock; muscular movement loosening clot |
| Secondary | 7-14 days after injury | Vessel wall erosion due to infection/sepsis |
B. By Source of Vessel
| Type | Description |
|---|---|
| Arterial | Bright red, spurting, pulsatile; does not clot easily due to pressure |
| Venous | Dark red, continuous oozing flow |
| Capillary | Oozing from raw surfaces; usually self-limiting |
C. By Location
| Type | Description |
|---|---|
| External | Blood visible outside the body |
| Internal | Blood in body cavities (hemothorax, hemoperitoneum, retroperitoneal) |
| Concealed | Blood within tissues (hematoma, intracranial hemorrhage) |
D. By Severity - ATLS Classification (Schwartz's Surgery, Table 5-5)
| Parameter | Class I | Class II | Class III | Class IV |
|---|---|---|---|---|
| Blood loss (mL) | < 750 | 750-1500 | 1500-2000 | > 2000 |
| Blood loss (%) | < 15% | 15-30% | 30-40% | > 40% |
| Heart rate (bpm) | < 100 | > 100 | > 120 | > 140 |
| Blood pressure | Normal | Orthostatic changes | Hypotension | Severe hypotension |
| CNS symptoms | Normal | Anxious | Confused | Obtunded |
Note: Young, healthy patients may maintain near-normal blood pressure until sudden cardiovascular collapse. Elderly patients on beta-blockers or anticoagulants tolerate much less. A systolic BP < 110 mmHg is now considered a clinically relevant threshold for hypoperfusion (Eastridge et al.).
5. CLINICAL FEATURES
Early/Compensated Stage (Class I-II, <30% blood loss)
- Tachycardia (most sensitive early sign)
- Cool, clammy extremities
- Pallor
- Mild anxiety or restlessness
- Orthostatic hypotension
- Mild tachypnea
Decompensated Stage (Class III-IV, >30% blood loss)
- Hypotension (SBP < 90-100 mmHg; now < 110 mmHg is considered significant)
- Marked tachycardia (HR > 110-120 bpm)
- Confusion, agitation, or obtundation
- Absent or weak peripheral pulses
- Oliguria / anuria
- Severe pallor, cold sweating
- Rapid, shallow breathing
Features by Location
- External hemorrhage: Visible bleeding from wounds, open fractures
- Hemothorax: Decreased breath sounds, dullness to percussion, dyspnea
- Hemoperitoneum: Abdominal distension, tenderness, guarding, rigidity
- Retroperitoneal: Flank bruising (Grey Turner sign), pelvic tenderness; often occult
- Intracranial: Headache, vomiting, altered GCS, focal neurology
- Cardiac tamponade: Beck's triad - hypotension + raised JVP + muffled heart sounds (even 300-400 mL blood in pericardial sac is fatal)
Key point: Substantial volumes of blood may be lost before classic manifestations of shock appear. "When a patient is significantly tachycardic or hypotensive, this represents both significant blood loss AND physiologic decompensation." - Schwartz's Surgery
6. DIAGNOSIS
Clinical Assessment
- History: mechanism of injury, anticoagulant use, bleeding disorders
- Vital signs: tachycardia, hypotension, tachypnea
- Physical exam: site of external bleeding, abdominal/thoracic signs, GCS
Laboratory Investigations
| Test | Significance |
|---|---|
| Hemoglobin / Hematocrit | Initial Hct may be normal (no time for equilibration); admission Hct correlates with 24-hr transfusion requirement |
| Serum Lactate | Indirect marker of tissue hypoperfusion; elevated in hemorrhagic shock; serial levels predict morbidity and mortality |
| Base Deficit (ABG) | Mild: -3 to -5; Moderate: -6 to -9; Severe: < -10 mmol/L - correlates with transfusion requirement and mortality |
| Coagulation profile | PT, aPTT, INR, fibrinogen - assess for coagulopathy |
| Blood type & crossmatch | Emergency transfusion preparation |
| Serum electrolytes, creatinine | Organ function |
Note: Lactate and base deficit both correlate with shock severity but interestingly do not firmly correlate with each other - evaluation of both is useful.
Imaging
| Modality | Use |
|---|---|
| FAST (Focused Assessment with Sonography in Trauma) | Rapid bedside detection of intraperitoneal/pericardial blood |
| Chest X-ray | Hemothorax, widened mediastinum |
| Pelvic X-ray | Pelvic fractures as a source of retroperitoneal hemorrhage |
| CT scan (abdomen/chest/head) | Hemodynamically stable patients; gold standard for identifying source and extent |
| Diagnostic Peritoneal Lavage (DPL) | Rapid identification of intraperitoneal blood when US unavailable |
| Angiography | Identification and embolization of arterial bleeding |
7. TREATMENT
Immediate Priorities (in order)
(a) Control the source of blood loss → (b) Volume resuscitation → (c) Secure the airway
Shock in a trauma or postoperative patient is assumed to be from hemorrhage until proven otherwise.
A. Hemorrhage Control
External Bleeding:
- Direct sustained pressure to wound
- Tourniquets for extremity bleeding not controlled by pressure (apply in pre-hospital setting)
- Wound packing with hemostatic agents (Combat gauze)
- Proximal vascular control
Intraoperative Major Vascular Injury (Sabiston):
- Direct compression + proximal vascular isolation and clamping
- For aortic injury: supraceliac aortic compression - retract stomach caudally, mobilize left lobe of liver, divide gastrohepatic ligament, compress aorta against vertebrae
- Hands-free aortic control: incise peritoneum, separate limbs of right diaphragmatic crus, apply aortic clamp
- Endovascular balloon occlusion of aorta (REBOA) - for patients with femoral arterial access
- Venous injury: compression + direct suture repair
Damage Control Surgery:
- For multiple bleeding sites, coagulopathy, hypothermia - abbreviated "damage control" laparotomy
- Pack and temporize, achieve hemostasis, close abdomen temporarily
- Return to ICU for resuscitation, then definitive repair
Angioembolization:
- For pelvic fracture hemorrhage, hepatic/splenic hemorrhage in stable patients
- Identifies arterial source and occludes with coils or gelfoam
B. Damage Control Resuscitation (Current Strategy - Schwartz's Surgery)
This strategy begins in the emergency department, continues into the OR and ICU:
1. Permissive Hypotension:
- Target SBP 80-90 mmHg in penetrating injuries
- Prevents renewed bleeding from recently clotted vessels
- For blunt injury with head injury: SBP ≥ 110 mmHg (hypotension worsens brain injury)
- Aggressive crystalloid resuscitation to normalize BP is counterproductive - increases bleeding and mortality
2. Balanced Blood Product Resuscitation:
- Resuscitate with blood products, NOT crystalloids
- Ratio: Packed Red Blood Cells : Fresh Frozen Plasma : Platelets = 1:1:1
- Early use of FFP to correct coagulopathy
- Massive transfusion protocol (MTP) activated for estimated blood loss > 10 units PRBCs/24h
- Cryoprecipitate for fibrinogen replacement (fibrinogen < 150 mg/dL)
- Recombinant Factor VIIa in refractory coagulopathic bleeding
3. Prevent / Treat the "Lethal Triad":
- Hypothermia - warm IV fluids, warm OR, warming blankets; aim temp > 35°C
- Acidosis - control with hemorrhage control + resuscitation; bicarbonate rarely indicated
- Coagulopathy - treat with FFP, platelets, cryo; avoid dilutional coagulopathy
4. Tranexamic Acid (TXA):
- Antifibrinolytic agent
- Give within 3 hours of injury (CRASH-2 trial) - reduces mortality
- 1 g IV over 10 min, then 1 g over 8 hours
5. Vasopressors:
- Only after adequate volume replacement
- Norepinephrine first-line for refractory vasodilatory shock
C. Surgical Procedures by Source
| Source | Procedure |
|---|---|
| Intra-abdominal | Emergency laparotomy, damage control |
| Intrathoracic | Tube thoracostomy (diagnostic + therapeutic); thoracotomy if > 1500 mL initial output or >200 mL/hr persistent |
| Pelvic fracture | External fixation + angioembolization; pelvic packing |
| GI hemorrhage | Endoscopic hemostasis, angioembolization, surgery |
| Intracranial | Neurosurgical evacuation |
8. COMPLICATIONS
Early Complications
| Complication | Mechanism |
|---|---|
| Hemorrhagic shock | Circulatory failure from volume loss |
| Cardiac tamponade | 300-400 mL blood in pericardium impairs cardiac filling and output |
| Cerebral anoxia / Death | Rapid BP fall → cerebral ischemia |
| Airway obstruction | Hemorrhage into trachea/bronchi acts as mechanical barrier → asphyxia |
| Coagulopathy (DIC) | Consumption of clotting factors, dilution from massive transfusion |
| Lethal Triad | Hypothermia + Acidosis + Coagulopathy - each worsens the others |
Late Complications
| Complication | Mechanism |
|---|---|
| Acute Respiratory Distress Syndrome (ARDS) | Inflammatory response from massive transfusion and hypoperfusion |
| Acute Kidney Injury (AKI) | Renal hypoperfusion, ATN |
| Multiple Organ Dysfunction Syndrome (MODS) | Prolonged hypoperfusion, reperfusion injury, inflammatory cascade |
| Acute Tubular Necrosis | Ischemic renal injury |
| Secondary infection / Sepsis | Immunosuppression from trauma + transfusions |
| Abdominal Compartment Syndrome | After damage control with massive fluid/blood resuscitation |
| Transfusion-Related Lung Injury (TRALI) | From massive blood product transfusion |
| Reperfusion Injury | After restoration of blood flow; reactive oxygen species cause cellular damage |
| Anemia | Chronic sequel requiring iron/transfusion support |
| Secondary Hemorrhage | Erosion of vessel wall by infection 7-14 days post injury |
Key Clinical Pearls (Surgical)
-
Tachycardia alone is unreliable - only 65% of hypotensive hemorrhagic shock patients had tachycardia in one study; it was present in only 59% of those needing > 5 units pRBC.
-
"Hypotension begins at 110 mmHg" - a SBP < 110 mmHg correlates with increasing mortality in trauma hemorrhage (Eastridge et al.).
-
Partial arterial transection bleeds MORE than complete transection - because retraction and spasm cannot occur.
-
The abdomen can hide enormous blood volumes - physical exam is unreliable; use FAST/CT/DPL.
-
Damage control resuscitation - permissive hypotension + 1:1:1 blood products + early surgical hemorrhage control is the current standard of care.
-
Time is survival - each 3-minute delay in the ED increases mortality by approximately 1% in patients needing emergency laparotomy for hemorrhage.
Sources: Schwartz's Principles of Surgery 11th Ed. (pp. 161-174), Sabiston Textbook of Surgery, Forensic Medicine & Toxicology 36th Ed. (pp. 9591-9650)
Explain the hemorrhoids in detail according to surgery book Definition, Etiology, pathogenesis in flow chart, classification, clinical features, diagnosis, treatment, complications
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the comprehensive content needed. Let me compile the full, detailed surgical answer on hemorrhoids.
HEMORRHOIDS - A Surgical Perspective
Sources: Schwartz's Principles of Surgery 11th Ed., Current Surgical Therapy 14th Ed., Sabiston Textbook of Surgery
1. DEFINITION
Hemorrhoids (also called "piles") are cushions of submucosal tissue containing venules, arterioles, and smooth muscle fibers located in the anal canal. They are a normal part of anorectal anatomy that functions as part of the continence mechanism, aiding in complete closure of the anal canal at rest.
Three primary hemorrhoidal cushions are found at constant positions:
- Right anterior
- Right posterior
- Left lateral
(At the 3, 7, and 11 o'clock positions in the lithotomy view)
Hemorrhoidal disease (symptomatic hemorrhoids) occurs when these normal vascular cushions become enlarged, engorged, prolapsed, or thrombosed, causing symptoms such as bleeding, prolapse, pain, and pruritus. Treatment is only indicated when they become symptomatic.
2. ANATOMY
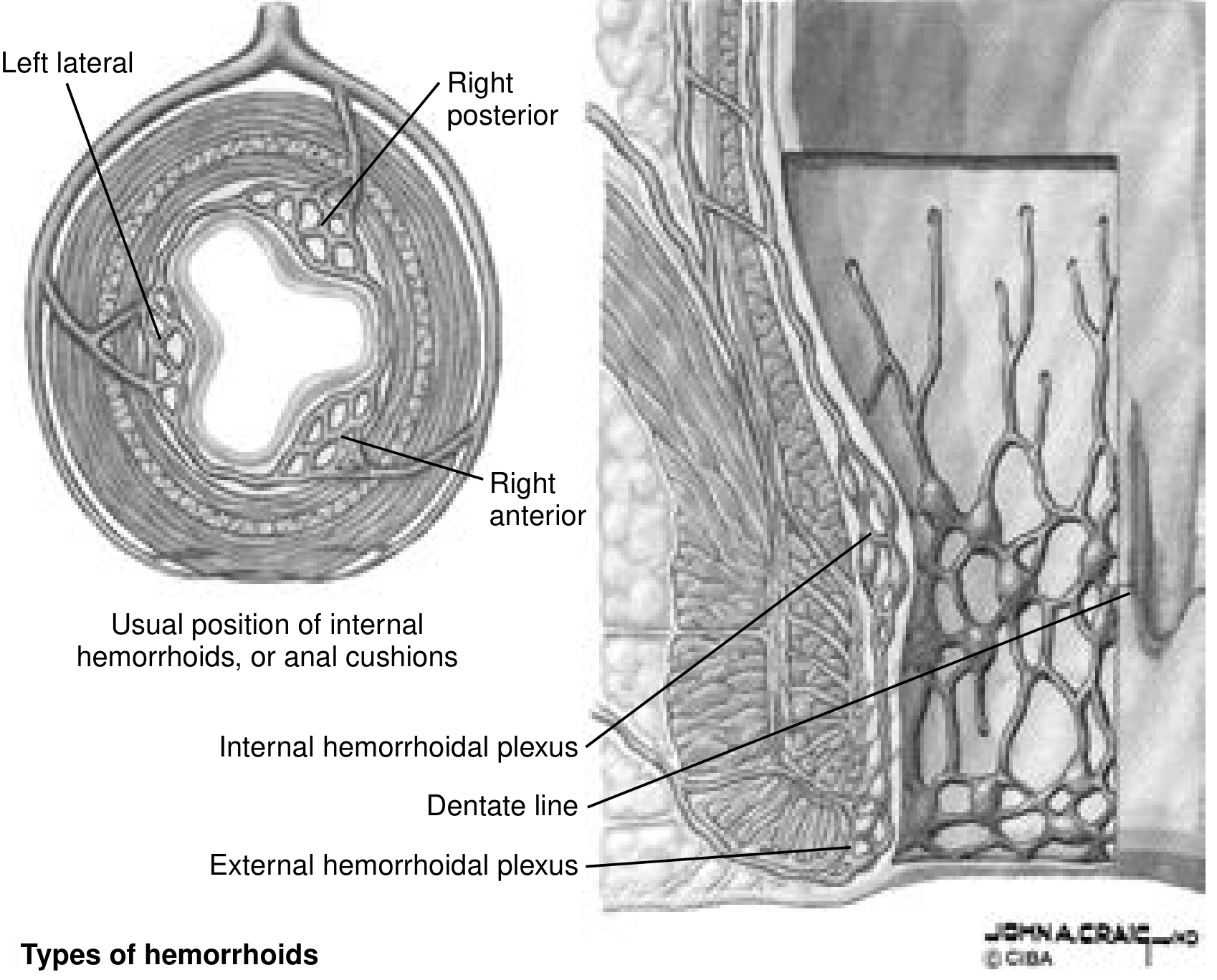
Anatomy of hemorrhoids showing the three cushion positions and the relationship to the dentate line. Current Surgical Therapy 14e.
The dentate line (pectinate line) is the critical anatomical landmark:
- Above dentate line: internal hemorrhoids (covered by insensate anorectal mucosa, visceral innervation - painless unless thrombosed/strangulated)
- Below dentate line: external hemorrhoids (covered by anoderm, richly innervated by somatic nerves - painful when thrombosed)
3. ETIOLOGY
Predisposing Factors
| Category | Factor |
|---|---|
| Dietary | Low-fiber diet, inadequate fluid intake |
| Bowel habits | Chronic constipation, prolonged straining at defecation, diarrhea |
| Increased intra-abdominal pressure | Pregnancy, obesity, ascites, chronic cough |
| Occupational | Prolonged sitting (e.g., drivers, desk workers); time spent on toilet >3 min |
| Vascular | Portal hypertension (though hemorrhoidal disease is not more common - rectal varices may develop separately) |
| Age | Weakening of supporting connective tissue with aging |
| Lifestyle | Sedentary lifestyle, low physical activity |
| Hereditary | Family history of hemorrhoids |
| Hormonal | Pregnancy (straining during labor causes edema, thrombosis, strangulation) |
4. PATHOGENESIS - FLOW CHART
PREDISPOSING FACTORS
(Low fiber diet, constipation, straining, pregnancy,
obesity, prolonged sitting, aging, portal hypertension)
|
v
INCREASED INTRA-ABDOMINAL / INTRARECTAL PRESSURE
|
_______|_______
| |
v v
VENOUS ENGORGEMENT WEAKENING OF
OF HEMORRHOIDAL ANCHORING CONNECTIVE
PLEXUS TISSUE (Treitz muscle,
Parks ligament)
| |
|_______________|
|
v
ENGORGEMENT + LOSS OF MUCOSAL FIXATION
|
_______|________
| | |
v v v
BLEEDING PROLAPSE THROMBOSIS
(Bright (Grade (External or
red blood I - IV) Incarcerated
per rectum) internal)
| | |
v v v
PAINLESS MUCOID PAIN,
HEMATOCHEZIA DISCHARGE SWELLING,
PRURITUS NECROSIS
|
v
STRANGULATION
(Grade IV - irreducible,
vascular compromise)
|
v
GANGRENE
Key Pathophysiological Mechanism (Sliding Anal Cushion Theory - Thomson 1975):
- Normal: Hemorrhoidal cushions are supported by the internal sphincter, Treitz muscle, and Parks ligament
- Disease: Repeated straining and engorgement cause downward displacement ("sliding") of the cushions
- Venous engorgement leads to enlargement
- Disruption of the mucosal suspensory ligament (Parks ligament) allows prolapse
- Once prolapsed, the mucosa is exposed to the environment, causing mucoid discharge, irritation, and pruritus
5. CLASSIFICATION
A. Anatomical Classification
| Type | Location | Covering | Sensation |
|---|---|---|---|
| Internal | Proximal to dentate line | Anorectal mucosa | Insensate (visceral) - painless unless strangulated |
| External | Distal to dentate line | Anoderm (squamous epithelium) | Somatic innervation - painful when thrombosed |
| Mixed (Combined) | Straddle the dentate line | Both | Both characteristics |
B. Grading of Internal Hemorrhoids (Classic Goligher Classification)
| Grade | Location / Behavior | Symptoms |
|---|---|---|
| Grade I | Bulge into anal canal; do not prolapse | Painless bright red bleeding |
| Grade II | Prolapse through anus with straining/defecation; reduce spontaneously | Bleeding, pressure, itching |
| Grade III | Prolapse through anus; require manual reduction | Bleeding, pressure, mucoid drainage |
| Grade IV | Prolapsed and cannot be reduced; at risk for strangulation | Pain, bleeding, pressure, mucoid drainage |
(Current Surgical Therapy 14e, Table 1)
6. CLINICAL FEATURES
Symptoms
Internal Hemorrhoids:
- Painless bright red rectal bleeding - hallmark symptom; blood drips or squirts into toilet bowl, coats stool (does not mix with it); usually occurs with defecation
- Prolapse - tissue protruding from anus (grades II-IV)
- Mucoid discharge - from exposed mucosa of prolapsed hemorrhoids
- Pruritus ani - from mucoid discharge irritating perianal skin
- Feeling of incomplete evacuation or anal discomfort
- Pain - only if thrombosis or strangulation occurs (severe, constant)
External Hemorrhoids:
- Pain and swelling - sudden onset of painful perianal mass; most commonly due to acute thrombosis
- Perianal lump - tense, bluish, tender swelling at anal verge
- Itching and hygiene difficulty if skin tags are large (skin tags = fibrotic residua of prior thrombosed external hemorrhoids)
- Bleeding - less common; occurs if thrombosis erodes skin
Strangulated / Acutely Prolapsed Hemorrhoids:
- Circumferential prolapse, edematous, dark red or purple
- Severe constant pain
- Unable to be reduced
- Can progress to necrosis / gangrene
Signs on Examination
External inspection:
- Skin tags at anal verge
- Externally visible prolapsed hemorrhoids (grades III-IV)
- Thrombosed external hemorrhoid: tense, bluish, tender perianal mass
Digital Rectal Examination (DRE):
- Internal hemorrhoids are NOT palpable (soft and compressible)
- Important to rule out other anorectal pathology
Proctoscopy / Anoscopy:
- Definitive visualization of internal hemorrhoids
- Hemorrhoids bulge into the lumen when patient strains
- Appearance: purple-red vascular cushions at 3, 7, 11 o'clock positions
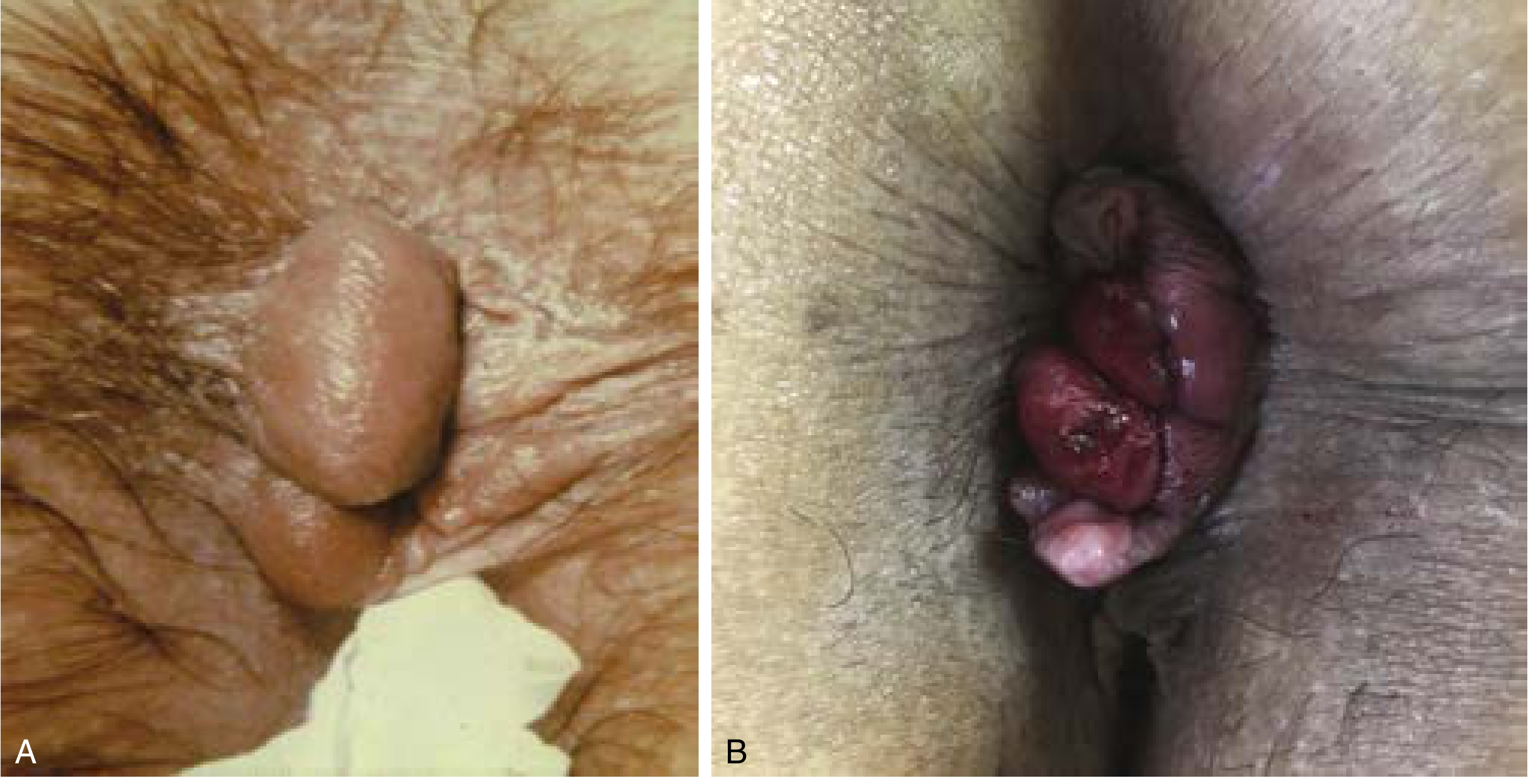
Left: Acute thrombosed external hemorrhoid. Right: Prolapsed and strangulated internal + external hemorrhoids. Current Surgical Therapy 14e.
7. DIAGNOSIS
Clinical Diagnosis
- History of painless bright red PR bleeding, prolapse, mucoid discharge, pruritus
- Examination: inspection, DRE, anoscopy, proctoscopy
Key Investigations
| Investigation | Purpose |
|---|---|
| Anoscopy | Gold standard for visualizing internal hemorrhoids; identifies site, size, grade |
| Rigid/flexible proctoscopy | Views rectum; excludes rectal polyps and carcinoma |
| Colonoscopy | Mandatory if: age > 40, change in bowel habit, family history of colorectal cancer, iron deficiency anemia, or if symptoms do not respond to treatment |
| Full blood count | Assess for anemia from chronic blood loss |
| Coagulation screen | If bleeding disorder suspected |
| LFTs / clotting | If portal hypertension suspected |
Differential Diagnosis (Important - Must Exclude)
| Condition | Distinguishing Feature |
|---|---|
| Colorectal carcinoma | Change in bowel habit, blood mixed with stool, tenesmus, mass on colonoscopy |
| Rectal polyps | Colonoscopy |
| Anal fissure | Tearing pain with defecation, visible fissure at anoderm |
| Rectal prolapse | Full-thickness rectal wall protrudes; concentric mucosal rings |
| Inflammatory bowel disease | Diarrhea, mucus, systemic features |
| Anal carcinoma | Hard ulcerated perianal mass, inguinal lymphadenopathy |
| Rectal varices (in portal HTN) | Lowering portal pressure is the treatment, not hemorrhoidectomy |
Important: Hemorrhoids should never be assumed to be the cause of rectal bleeding in patients over 40 without colonoscopic exclusion of colorectal cancer.
8. TREATMENT
Treatment is indicated only for symptomatic hemorrhoids.
STEP 1: Conservative / Medical Management (All Grades, First Line)
(Sufficient for Grade I and Grade II in the majority of patients)
- High-fiber diet - 25-35 g/day; psyllium or methylcellulose supplement
- Increased fluid intake - 8 or more glasses of water per day; reduce caffeine and alcohol
- Stool softeners - docusate sodium
- Bowel habit modification - avoid straining; reduce time on toilet to < 3 minutes; no reading/phone on toilet
- Warm sitz baths - 2-3 times daily; reduces edema and soothes
- Topical agents - witch hazel (cotton application), topical hydrocortisone or -caine preparations (temporary symptomatic relief only - do not reduce hemorrhoids long-term)
- Phlebotonics - flavonoids (e.g., diosmin, hesperidin); improve venous tone, reduce inflammation, decrease bleeding and pruritus
STEP 2: Office-Based (Non-Operative) Procedures
(For Grade I, II, and selected Grade III hemorrhoids that fail conservative management)
1. Rubber Band Ligation (RBL) - Most Common Office Procedure
- Indication: Grade I, II, III internal hemorrhoids
- Contraindicated in: patients on anticoagulants, antiplatelet therapy, or latex allergy
- Technique: Mucosa 1-2 cm proximal to dentate line is grasped and pulled into rubber band applier; band strangulates underlying tissue → fibrosis → prevents bleeding/prolapse
- Only 1-2 quadrants banded per session (spaced 3-4 weeks apart)
- Complications: Pain if band placed too close to dentate line; urinary retention (~1%); vasovagal reaction; thrombosis of external hemorrhoid; delayed bleeding (7-10 days when pedicle sloughs); necrotizing infection (rare but life-threatening - presents with severe pain + fever + urinary retention - requires urgent exam under anesthesia, debridement, broad-spectrum antibiotics)
- Success rate > 90%
2. Sclerotherapy (Injection Therapy)
- Indication: Grade I, II hemorrhoids; safe for patients on anticoagulants
- Sclerosants: 5% phenol in almond oil, hypertonic saline, ethanolamine, sodium morrhuate, quinine urea
- Technique: 1-3 mL injected into submucosa of hemorrhoid at 1 cm above dentate line; all 3 hemorrhoids may be treated in one session
- Mechanism: Sclerosis → shrinkage → fibrosis → fixation
- Complications: Injection into muscle (pain, ulceration, sloughing); infection; fibrosis
3. Infrared Photocoagulation (IRC)
- Indication: Grade I, II hemorrhoids
- Infrared energy applied at apex of hemorrhoid → coagulation → thrombosis → tissue destruction → scarring/fixation
- 3-4 applications per hemorrhoid; all 3 treated in one session
- Well tolerated; similar side effects to RBL
4. HET Bipolar System
- Grade I, II hemorrhoids
- Specialized forceps grasp hemorrhoid; bipolar energy applied
- Well tolerated
STEP 3: Operative Treatment
(For Grade III-IV hemorrhoids failing office treatment; Grade IV and strangulated hemorrhoids; combined internal-external hemorrhoids; postpartum hemorrhoids)
Only ~5-10% of patients with symptomatic hemorrhoids require surgery.
A. Closed Submucosal Hemorrhoidectomy (Ferguson / Parks Hemorrhoidectomy)
- Most common technique
- Patient in prone jackknife or lithotomy position
- Elliptical incision from just distal to anal verge proximally to anorectal ring
- Internal sphincter fibers identified and preserved (not injured)
- Apex of hemorrhoidal plexus ligated; hemorrhoid excised
- Wound closed with running absorbable suture
- All three hemorrhoidal cushions may be removed; must preserve adequate perianal skin bridges to prevent anal stenosis
B. Open Hemorrhoidectomy (Milligan-Morgan Technique)
- Same excision as above, but wounds left open to heal by secondary intention
- Traditional technique; used widely in UK
- Slower healing but lower risk of wound infection
C. Whitehead's Hemorrhoidectomy
- Circumferential excision of all hemorrhoidal cushions just proximal to dentate line
- Largely abandoned due to risk of ectropion (Whitehead's deformity) - rectal mucosa pulled down to anal verge
D. Procedure for Prolapse and Hemorrhoids (PPH) / Stapled Hemorrhoidopexy
- Best suited for Grade II-III internal hemorrhoids
- Stapling device removes a ring of mucosa and submucosa proximal to the dentate line
- Mechanism: pexies redundant hemorrhoidal tissue + ligates venules feeding hemorrhoidal plexus + fixes redundant mucosa proximally
- Advantages: less postoperative pain and disability; shorter recovery
- Complications: chronic anal pain, bacteremia, rectovaginal fistula, obstructing rectal stricture, rectal perforation
- Recurrence rate slightly higher than excisional hemorrhoidectomy
E. Doppler-Guided Hemorrhoidal Artery Ligation (DGHAL) / Trans-Anal Hemorrhoidal Dearterialization (THD)
- Doppler probe identifies the feeding artery/arteries
- Vessels are ligated
- Less invasive; early results promising; long-term durability still being assessed
Special Situations
Acute Thrombosed External Hemorrhoid
- Present within first 72 hours: Elliptical excision under local anesthesia in outpatient/office setting (simple incision and drainage is rarely effective as clot is loculated)
- After 72 hours: clot begins to resorb; pain resolves spontaneously; conservative management with sitz baths and analgesics sufficient; excision unnecessary
Acute Hemorrhoidal Crisis (Circumferential Prolapse)
- Circumferential prolapsed, thrombosed, incarcerated internal and external hemorrhoids ± necrosis
- Without necrosis: Inject mixture of 1% lidocaine with epinephrine + normal saline + hyaluronidase into all edematous tissues; massage; pressure dressing
- With necrosis: Emergency hemorrhoidectomy
Postpartum Hemorrhoids
- Hemorrhoidectomy is often the treatment of choice, especially in patients with chronic hemorrhoidal symptoms
Portal Hypertension + Hemorrhoids
- Hemorrhoidal disease is NOT more common in portal hypertension
- Rectal varices (distinct from hemorrhoids) may develop and bleed
- Treatment of rectal varices: lower portal venous pressure (pharmacologic/TIPS); rarely suture ligation
- Surgical hemorrhoidectomy should be avoided in portal hypertension due to bleeding risk
9. COMPLICATIONS
Complications of Hemorrhoidal Disease
| Complication | Description |
|---|---|
| Anemia | Chronic iron deficiency from repeated painless bleeding |
| Thrombosis | Thrombosis of external or prolapsed internal hemorrhoids; acute pain |
| Strangulation | Grade IV prolapsed hemorrhoids with vascular compromise |
| Gangrene / Necrosis | End stage of strangulated hemorrhoids; sepsis risk |
| Prolapse | Progressive prolapse from Grade II to Grade IV |
| Perianal skin irritation | From mucoid discharge causing excoriation and pruritus ani |
Complications of Rubber Band Ligation
| Complication | Notes |
|---|---|
| Pain | Band placed too close to dentate line |
| Urinary retention | ~1%; more likely if internal sphincter included in ligation |
| Vasovagal reaction | During procedure |
| External hemorrhoid thrombosis | Contiguous thrombosis |
| Delayed bleeding | 7-10 days post-ligation when pedicle sloughs |
| Necrotizing infection | Rare but life-threatening; severe pain + fever + urinary retention = emergency |
Complications of Hemorrhoidectomy
| Complication | Notes |
|---|---|
| Postoperative pain | Most common; requires multimodal analgesia (opioids, NSAIDs, muscle relaxants, sitz baths) |
| Urinary retention | 10-50% in some series; minimize by limiting intraoperative IV fluids and adequate analgesia |
| Bleeding (early) | Inadequate ligation of vascular pedicle; requires return to OR for suture ligation |
| Bleeding (delayed, 7-10 days) | Sloughing of necrotic mucosa; exam under anesthesia ± ligation |
| Fecal impaction | Secondary to pain inhibiting defecation; preoperative enemas + postoperative laxatives reduce risk |
| Infection | Uncommon; necrotizing soft tissue infection possible - presents with severe pain + fever + urinary retention |
| Anal stenosis (long-term) | From scarring after excessive resection of perianal skin/anoderm |
| Fecal incontinence (long-term) | Transient incontinence to flatus common; permanent rare; from sphincter injury |
| Ectropion / Whitehead's deformity | After Whitehead's hemorrhoidectomy; rectal mucosa everts to anal verge |
| Recurrence | Higher after PPH/stapled hemorrhoidopexy than excisional hemorrhoidectomy |
| Rectovaginal fistula | Complication specific to PPH |
| Rectal perforation | Rare complication of PPH |
Summary Treatment Algorithm
SYMPTOMATIC HEMORRHOIDS
|
v
GRADE I + II
|
+--> Conservative: High fiber + fluids + sitz baths + avoidance of straining
| |
| If fails
| v
| Office-based: RBL (preferred) / Sclerotherapy / IRC
|
GRADE III
|
+--> Office-based: RBL (first line)
| |
| If fails
| v
| Operative: Ferguson / Milligan-Morgan / PPH / DGHAL
|
GRADE IV / STRANGULATED / MIXED
|
+--> Operative Hemorrhoidectomy (Ferguson or Milligan-Morgan)
|
ACUTE THROMBOSED EXTERNAL (<72 hr)
|
+--> Elliptical Excision under local anesthesia
ACUTE THROMBOSED EXTERNAL (>72 hr)
|
+--> Conservative: sitz baths + analgesics
Sources: Schwartz's Principles of Surgery 11th Ed. (pp. 1337-1340), Current Surgical Therapy 14th Ed. (pp. 329-333), Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.