Spinothalamic tract physiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Excellent - I now have comprehensive content and two key diagrams. Let me compile the full answer.
Spinothalamic Tract - Physiology
Overview
The spinothalamic tract (STT) is the principal ascending pathway for pain, temperature, crude touch, and pressure from the body to the brain. It runs in the anterolateral white matter of the spinal cord and is part of a broader anterolateral system. It is a three-neuron chain: first-order (peripheral), second-order (spinal cord), and third-order (thalamus to cortex).
1. First-Order Neurons (Peripheral Afferents)
Primary afferent fibers carrying nociceptive and thermal information enter via the dorsal root:
| Fiber Type | Modality | Diameter / Myelination |
|---|---|---|
| A-delta (III) | Sharp, fast pain; cold temperature | Thinly myelinated, 5-30 m/s |
| C fibers (IV) | Slow, burning pain; warmth | Unmyelinated, 0.5-2 m/s |
These fibers enter the dorsal root entry zone and some collaterals travel up or down 1-2 segments in Lissauer's tract (dorsolateral fasciculus) before synapsing in the dorsal horn.
2. Second-Order Neurons (Dorsal Horn)
Synapses occur mainly in the dorsal horn laminae:
- Lamina I (marginal zone) - nociception-specific and thermosensitive neurons
- Lamina II (substantia gelatinosa) - modulation of pain (gate control)
- Lamina V - wide-dynamic-range (WDR) neurons responding to both nociceptive and non-nociceptive stimuli
- Laminae VII and VIII - deep dorsal horn neurons (for spinoreticular tract origin)
Key step - decussation: Axons of second-order neurons cross the midline via the anterior (ventral) white commissure to the contralateral anterolateral funiculus. Critically, this decussation takes 2-3 spinal segments to complete, so a lateral cord lesion produces contralateral sensory loss beginning 2-3 segments below the lesion level.
As new fibers cross and join the tract, they add onto the medial side, so:
- Sacral fibers = most lateral/superficial (outermost)
- Cervical fibers = most medial/deepest
This somatotopic organization explains the clinical phenomenon of sacral sparing in central cord lesions (the innermost sacral fibers are protected when a centrally placed lesion expands outward).
3. The Two Divisions of the STT
Lateral STT (Neospinothalamic Tract)
- Projects to the ventral posterolateral (VPL) nucleus of the thalamus
- Carries discriminative aspects of pain and temperature: location, intensity, duration, quality
- Fast pathway; sharp, well-localized pain
- Phylogenetically newer
Medial STT (Paleospinothalamic Tract)
- Projects to medial thalamic nuclei (mediodorsal, intralaminar - including centromedian nucleus)
- Mediates autonomic, affective, and emotional aspects of pain (the suffering component)
- Associated with arousal and poorly localized, diffuse pain
4. Ascending Course Through the Neuraxis
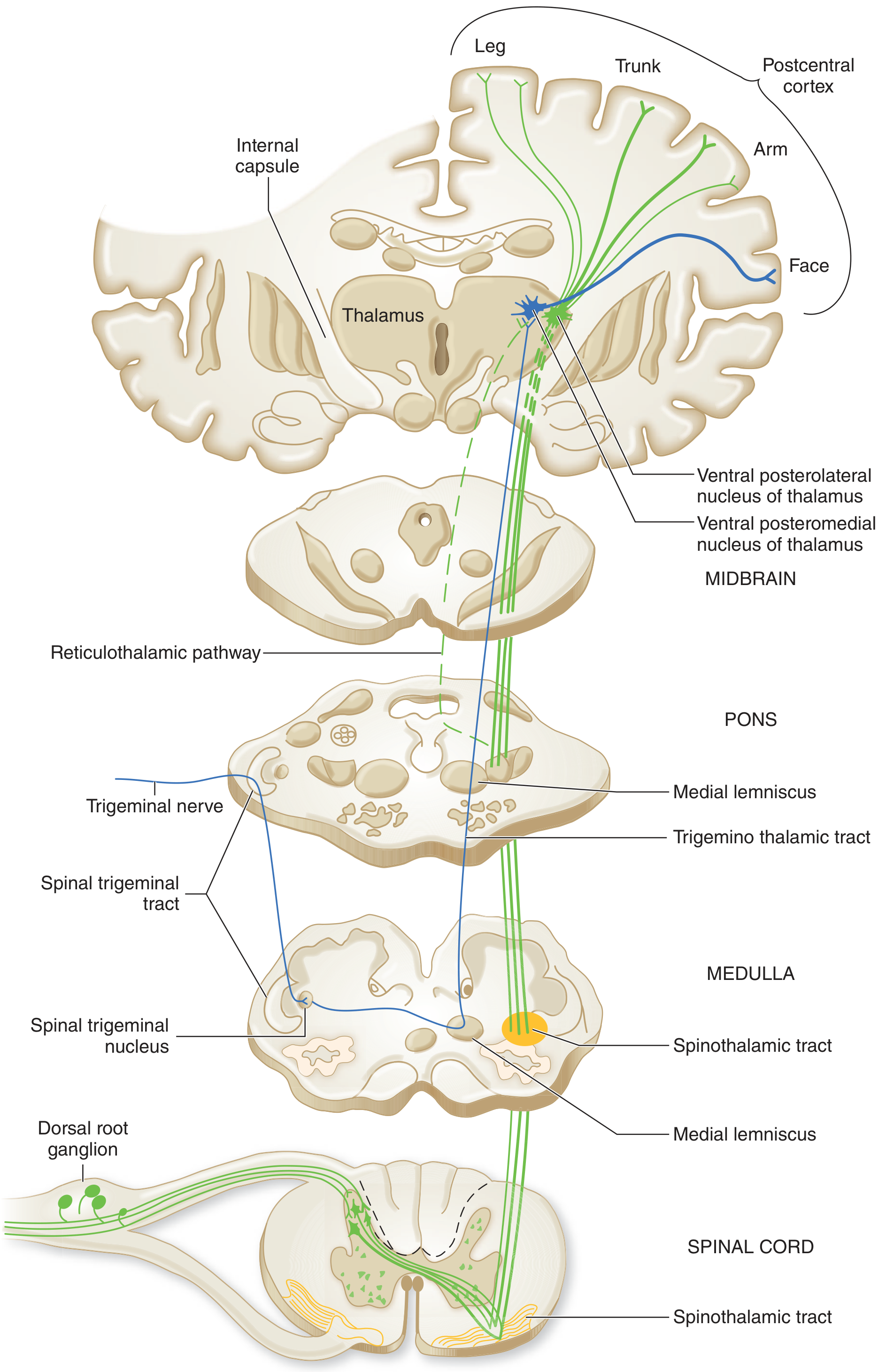
Figure from Adams and Victor's Principles of Neurology, 12th Ed.
| Level | Position of STT |
|---|---|
| Spinal cord | Anterolateral white matter, contralateral side |
| Medulla | Lateral surface, in groove between inferior olive and inferior cerebellar peduncle |
| Pons | Tegmentum, just lateral to the medial lemniscus |
| Midbrain | Lateral tegmentum, lateral to medial lemniscus |
| Thalamus | Terminates in VPL (lateral STT) and medial/intralaminar nuclei (medial STT) |
5. Spinal Cord Cross-Section: Somatotopic Arrangement
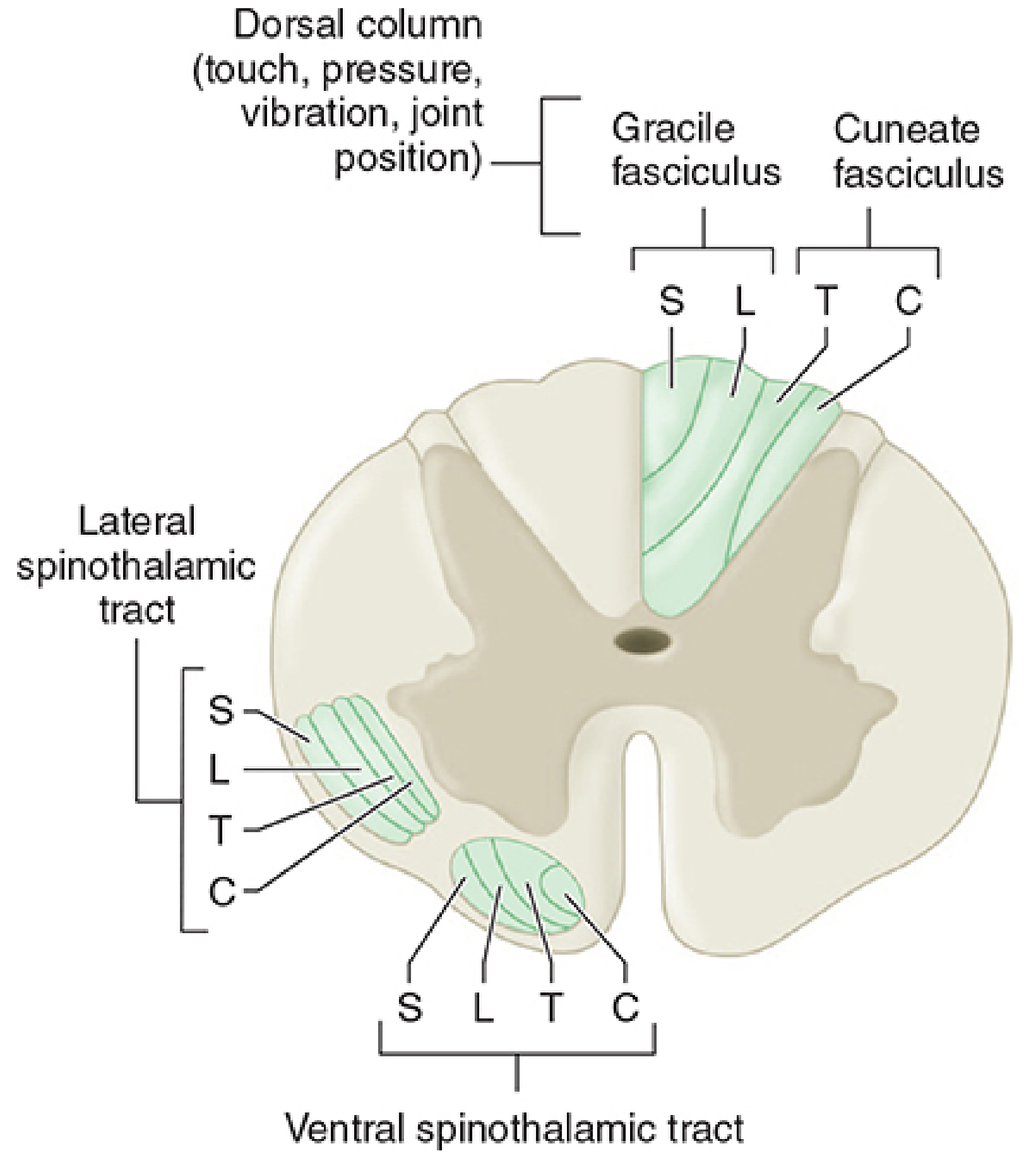
From Morgan and Mikhail's Clinical Anesthesiology, 7th Ed. - showing spatial distribution of fibers from different spinal levels (C, T, L, S) in the lateral and ventral spinothalamic tracts.
6. Third-Order Neurons (Thalamus to Cortex)
From the VPL, fibers pass via the posterior limb of the internal capsule and thalamic somatosensory radiations to the primary somatosensory cortex (S1, Brodmann areas 3, 1, 2) in the postcentral gyrus. This generates conscious perception of pain and temperature with localization.
The medial thalamic projections connect to the anterior cingulate cortex and insula via diffuse thalamocortical projections - generating the affective/unpleasant quality of pain.
7. Associated Anterolateral Tracts
The STT is part of a broader anterolateral system. Four major ascending nociceptive pathways exist (Kandel, Principles of Neural Science):
| Tract | Origin (Laminae) | Target | Function |
|---|---|---|---|
| Spinothalamic | I, V-VII | VPL/VPM thalamus | Discriminative pain/temperature; localization |
| Spinoreticular | VII, VIII | Reticular formation → intralaminar thalamus | Diffuse pain; arousal; autonomic responses |
| Spinoparabrachial | I, V | Parabrachial nucleus (pons) → amygdala | Affective/emotional component of pain |
| Spinohypothalamic | I, V, VII, VIII | Hypothalamus | Neuroendocrine and cardiovascular responses to pain |
8. Modalities Carried
| Division | Sensations |
|---|---|
| Lateral STT | Pain (sharp, fast), temperature (hot and cold), itch |
| Ventral (Anterior) STT | Crude touch, deep pressure, tickle |
9. Key Clinical Correlates
| Lesion | Deficit |
|---|---|
| Unilateral STT lesion | Contralateral loss of pain and temperature, 2-3 levels below lesion |
| Bilateral STT lesion (e.g., anterior cord syndrome) | Bilateral pain/temperature loss below lesion; dorsal columns (proprioception/vibration) spared |
| Central cord lesion | Sacral sparing - outer sacral fibers escape central damage |
| Brown-Séquard syndrome | Ipsilateral motor loss + dorsal column loss; contralateral pain/temperature loss (STT) |
| Syringomyelia | Disrupts decussating fibers in anterior commissure → bilateral "cape" distribution loss of pain/temperature at level of lesion, with preservation below (suspended sensory loss) |
| Anterolateral cordotomy | Surgical interruption used for intractable pain in terminal cancer - reduces contralateral pain below the level of the cut |
10. The Face - Trigeminothalamic Tract
An analogous pathway, the trigeminothalamic tract, subserves pain and temperature for the face via cranial nerve V. The spinal trigeminal nucleus (especially its caudal subnucleus) is the equivalent of the spinal dorsal horn; crossed fibers ascend to the ventral posteromedial (VPM) nucleus of the thalamus and on to S1.
Sources:
- Neuroanatomy through Clinical Cases, 3rd Edition
- Adams and Victor's Principles of Neurology, 12th Edition
- Morgan and Mikhail's Clinical Anesthesiology, 7th Edition
- Kandel - Principles of Neural Science, 6th Edition
Take reference from guyton
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have all the Guyton content needed. Here is the complete, Guyton-based answer:
Spinothalamic Tract - Physiology (Guyton & Hall, Medical Physiology)
The Two Somatic Sensory Pathways
Guyton begins by framing the spinothalamic tract within the context of the two major ascending somatic sensory systems:
| Feature | Dorsal Column-Medial Lemniscal System | Anterolateral System (Spinothalamic) |
|---|---|---|
| Fiber size | Large myelinated | Smaller myelinated |
| Conduction velocity | 30-110 m/s | A few m/s up to 40 m/s |
| Spatial localization | High fidelity, well-organized | Poor, crude |
| Intensity discrimination | Up to 100 gradations | Only 10-20 gradations |
| Temporal fidelity | High (handles rapidly changing signals) | Poor |
| Modalities | Fine touch, vibration, proprioception, pressure (fine) | Pain, temperature, crude touch, tickle, itch, sexual sensations |
"The anterolateral system has a special capability that the dorsal system does not have - the ability to transmit a broad spectrum of sensory modalities, such as pain, warmth, cold, and crude tactile sensations." - Guyton & Hall
Modalities Carried by the Anterolateral (Spinothalamic) System
According to Guyton, the anterolateral system carries:
- Pain
- Thermal sensations - both warm and cold
- Crude touch and pressure - capable only of crude localizing ability on the surface of the body
- Tickle and itch sensations
- Sexual sensations
Anatomy of the Anterolateral Pathway
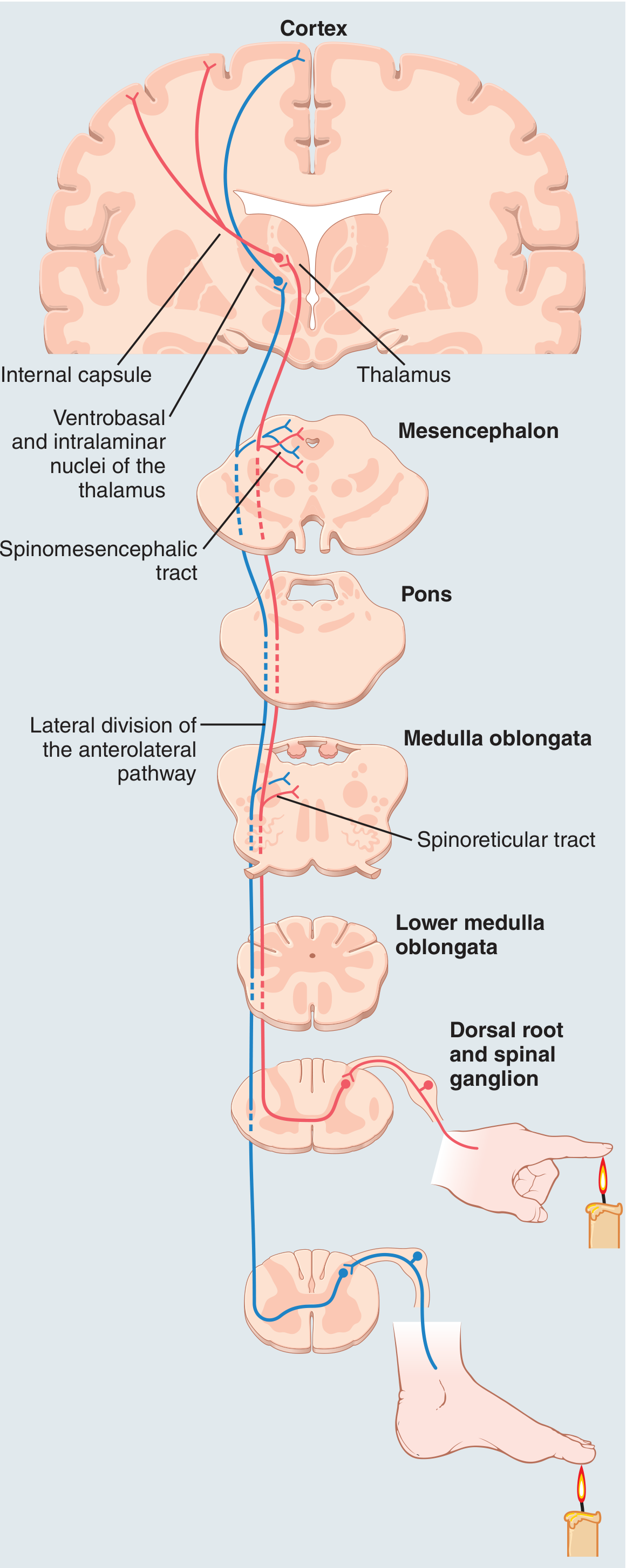
Figure 48.13 from Guyton & Hall - Anterior and lateral divisions of the anterolateral sensory pathway.
Step-by-Step Pathway
1. Origin - Dorsal Horn Laminae
Anterolateral fibers originate mainly in dorsal horn laminae I, IV, V, and VI - the layers where dorsal root sensory fibers terminate after entering the cord.
2. Decussation - Anterior Commissure
The anterolateral fibers cross immediately in the anterior commissure of the cord to the opposite anterior and lateral white columns, then turn upward toward the brain. This is the key step explaining why the STT produces contralateral sensory deficits.
3. Ascent - Two Divisions
The tract ascends as two divisions:
- Lateral spinothalamic tract - in the lateral white column
- Anterior (ventral) spinothalamic tract - in the anterior white column
4. Upper Terminus - Thalamus (Two Destinations)
Guyton identifies two main termination zones:
| Destination | Via | Signals Relayed |
|---|---|---|
| Ventrobasal complex of thalamus (VPL/VPM) | Direct spinothalamic projection | Tactile signals mainly; some pain |
| Intralaminar nuclei of thalamus | Via reticular nuclei of brain stem (spinoreticular route) | Most pain signals |
"Only a small fraction of the pain signals project directly to the ventrobasal complex of the thalamus. Instead, most pain signals terminate in the reticular nuclei of the brain stem and from there are relayed to the intralaminar nuclei of the thalamus." - Guyton & Hall
5. Cortical Projection
From the ventrobasal complex, signals are transmitted via the internal capsule to the somatosensory cortex.
Characteristics of Transmission in the Anterolateral Pathway
Guyton specifically lists how the anterolateral pathway differs from the dorsal column system:
- Velocity - only one-third to one-half that of the dorsal column system: 8 to 40 m/s
- Spatial localization - poor
- Intensity gradations - far less accurate - only 10 to 20 gradations of strength (vs. ~100 in dorsal column system)
- Temporal signal handling - poor ability to transmit rapidly changing or repetitive signals
"Thus, it is evident that the anterolateral system is a cruder type of transmission system than the dorsal column-medial lemniscal system. Even so, certain modalities of sensation are transmitted only in this system and not at all in the dorsal column-medial lemniscal system." - Guyton & Hall
Role of the Thalamus
Guyton makes a critical physiological distinction:
- Critical tactile sensibilities - depend heavily on the somatosensory cortex; lost when the cortex is destroyed
- Pain and temperature - the thalamus and lower brain stem play dominant roles in discriminating these sensibilities; cortical destruction has little effect on pain perception and only moderate effect on temperature
"Loss of the somatosensory cortex has little effect on one's perception of pain sensation... Therefore, the lower brain stem, the thalamus, and other associated basal regions of the brain are believed to play dominant roles in discrimination of these sensibilities." - Guyton & Hall
This reflects the phylogenetically older nature of the pain/temperature pathway.
Corticofugal Control (Top-Down Modulation)
Guyton describes a feedback control system: the cerebral cortex sends corticofugal signals back down to relay nuclei in the thalamus, medulla, and spinal cord. These signals are almost entirely inhibitory and serve to:
- Decrease lateral spread of sensory signals (sharpen the signal pattern)
- Keep the sensory system in an optimal sensitivity range - not too low (ineffective) nor too high (swamped)
Clinical Correlate: Brown-Séquard Syndrome (Guyton)
Guyton uses Brown-Séquard syndrome to illustrate STT physiology directly:
In a hemisection of the spinal cord:
| Deficit | Side | Pathway Explanation |
|---|---|---|
| Motor loss | Ipsilateral below lesion | Corticospinal tract (ipsilateral) |
| Pain, heat, cold loss | Contralateral, 2-6 segments below lesion | Spinothalamic tract already crossed |
| Vibration, proprioception, position loss | Ipsilateral below lesion | Dorsal columns (cross in medulla) |
| Fine/discrete light touch impaired | Ipsilateral | Dorsal column interrupted |
| Crude touch preserved | Both sides | Partial transmission in opposite spinothalamic tract |
"The sensations of pain, heat, and cold - sensations served by the spinothalamic pathway - are lost on the opposite side of the body in all dermatomes two to six segments below the level of the transection." - Guyton & Hall
Summary Comparison Table (Guyton Framework)
| Feature | Spinothalamic (Anterolateral) | Dorsal Column-Medial Lemniscal |
|---|---|---|
| Crosses | Immediately in anterior commissure | At medulla (gracile/cuneate nuclei) |
| Side of deficits | Contralateral | Ipsilateral |
| Thalamic relay | VPL + intralaminar (via reticular) | VPL (direct) |
| Cortical dependence for perception | Low (thalamus dominant for pain) | High |
| Speed | 8-40 m/s | 30-110 m/s |
| Localization | Crude | Fine, precise |
Source: Guyton and Hall Textbook of Medical Physiology (Chapter 48: Somatic Sensations; Chapter 49: Pain, Headache, and Thermal Sensations)
This is a shared conversation. Sign in to Orris to start your own chat.