Explain me everything about cushings syndrome
Reading File
Finding Sources
Searching PubMed
"Cushing syndrome" diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from authoritative textbooks plus excellent diagrams. Here is the complete guide to Cushing's syndrome:
Cushing's Syndrome - A Complete Guide
1. Definition
Cushing's syndrome is the clinical state resulting from prolonged, inappropriate exposure of tissues to excess glucocorticoids - specifically cortisol. It is a rare condition, occurring in 2-5 per million people per year. When the cause is a pituitary ACTH-secreting tumor, the term Cushing's disease specifically applies. The broader term "Cushing's syndrome" covers all causes.
- Campbell Walsh Wein Urology, p. 3134
2. Normal Physiology - The HPA Axis (Background)
The hypothalamic-pituitary-adrenal (HPA) axis is the governing feedback system:
-
The hypothalamus secretes corticotropin-releasing hormone (CRH), following circadian rhythms (peak cortisol in the morning, nadir ~11 PM)
-
CRH stimulates anterior pituitary corticotrophs to release ACTH (cleaved from pro-opiomelanocortin, POMC)
-
ACTH drives the zona fasciculata of the adrenal cortex to produce up to 20 mg of cortisol daily
-
Cortisol feeds back to the hypothalamus and pituitary to suppress further CRH and ACTH - completing the negative loop
-
Without ACTH, adrenal cortical cells (except mineralocorticoid-producing cells) undergo apoptosis
-
Campbell Walsh Wein Urology, p. 3134-3135
3. Classification and Causes
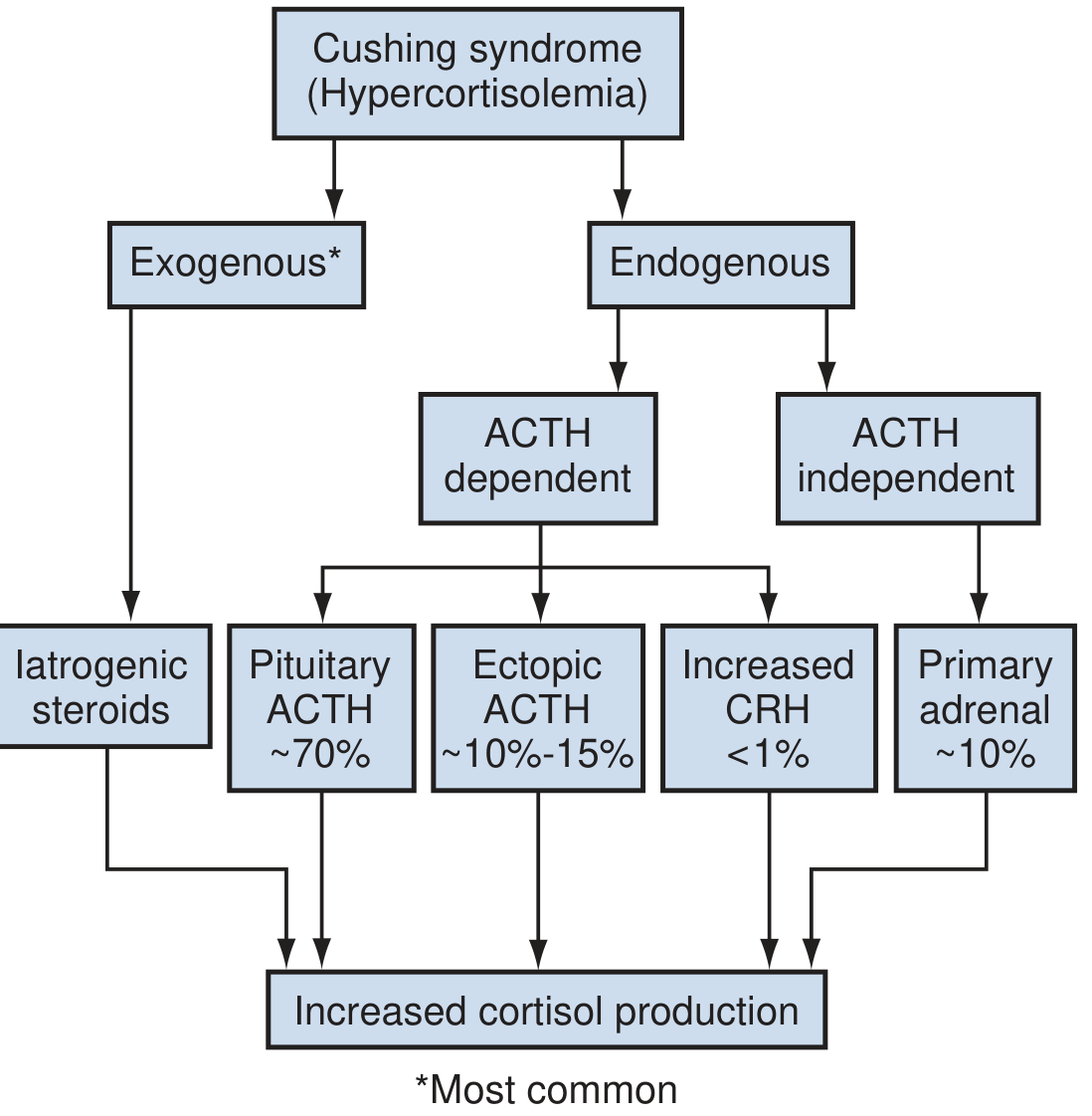
A. Exogenous (Iatrogenic) - MOST COMMON Overall
- Administration of synthetic glucocorticoids (oral, topical, inhaled, nasal, injectable)
- Even low doses can cause it; doses equivalent to ≥20 mg prednisone daily for >1 month are particularly risky
- Patients may be unaware (herbal preparations, nasal sprays) or use steroids surreptitiously
B. Endogenous - ACTH-Dependent (80-85% of endogenous cases)
| Cause | Frequency | Notes |
|---|---|---|
| Cushing's Disease (pituitary corticotroph adenoma) | ~70% of endogenous | Usually a microadenoma; macroadenomas only ~5%; 2/3 female |
| Ectopic ACTH syndrome | ~10-15% | Caused by non-pituitary malignant tumors (small cell lung cancer, carcinoids, pancreatic islet tumors, medullary thyroid cancer); very high ACTH levels |
| Ectopic CRH syndrome | <1% | Extremely uncommon |
C. Endogenous - ACTH-Independent (~15-20% of endogenous)
| Cause | Frequency | Notes |
|---|---|---|
| Adrenal adenoma | ~10% | Benign, unilateral; most common ACTH-independent cause |
| Adrenocortical carcinoma (ACC) | ~8% | Independent predictor of poor outcome |
| ACTH-independent macronodular adrenal hyperplasia (AIMAH) | <1% | Large bilateral nodules, each gland >60 g |
| Primary Pigmented Nodular Adrenocortical Disease (PPNAD) | <1% | Normal-sized glands with black/brown nodules; associated with Carney complex (autosomal dominant) |
- Campbell Walsh Wein Urology, pp. 3135-3136
4. Clinical Features
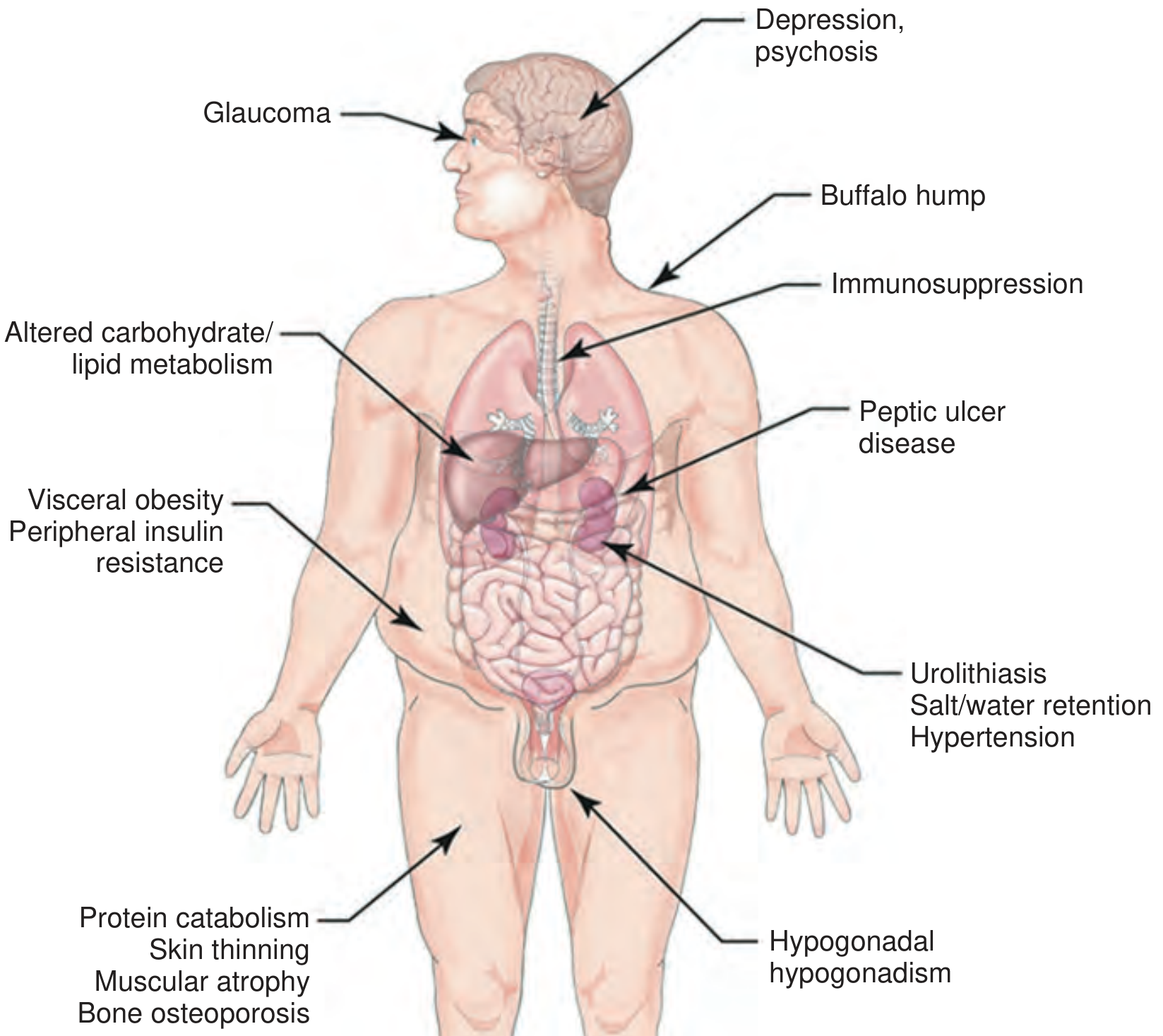
Body Habitus & Fat Distribution
- Central obesity - face, neck, trunk, abdomen - with sparing of the limbs
- Moon face - round, wide, plethoric
- Buffalo hump - dorsal cervical fat pad
- Supraclavicular fat pads
Skin Changes (highly characteristic)
- Violaceous (purple) striae - wide (>1 cm), atrophic; abdomen, flanks, breasts, thighs
- Skin thinning and fragility - "cigarette paper" wrinkling, easy peeling after adhesive tape (Liddle sign)
- Easy bruising - ecchymoses without trauma
- Plethora - reddish facial flush
- Hypertrichosis / facial lanugo hair (especially in women)
- Acne
- Susceptibility to superficial fungal infections (dermatophytes, Pityrosporum)
Musculoskeletal
- Proximal muscle weakness - difficulty rising from a chair, climbing stairs
- Osteoporosis - kyphosis, vertebral fractures, back pain
- Bone loss begins early in the course
Metabolic
- Hypertension (75-80%) - multiple mechanisms: sodium/water retention, increased vascular reactivity, RAAS activation
- Diabetes mellitus / insulin resistance (18-30%)
- Dyslipidemia
- Central obesity / metabolic syndrome
Neuropsychiatric
- Depression - most common psychiatric feature
- Anxiety, emotional lability, cognitive impairment
- Psychosis (less common but serious)
Reproductive / Endocrine
- Hypogonadism - loss of libido, impotence, menstrual irregularities, amenorrhea
- Decreased axillary/pubic hair
- Clitoromegaly (in women, from androgen excess)
Cardiovascular
- Ventricular hypertrophy, cardiac fibrosis
- Prothrombotic state - DVT, pulmonary embolism (major cause of death)
Other
-
Glaucoma, cataracts
-
Peptic ulcer disease
-
Urolithiasis (hypercalciuria)
-
Immunosuppression - increased infection risk
-
Impaired wound healing
-
Fitzpatrick's Dermatology, p. 578 | Campbell Walsh Wein Urology, pp. 3136-3138 | Braunwald's Heart Disease, p. 1141
5. Pseudo-Cushing's Syndrome
Certain conditions can mimic Cushing's syndrome biochemically and clinically, but do not represent true pathological hypercortisolism:
- Alcohol dependence
- Morbid obesity
- Poorly controlled diabetes mellitus
- Glucocorticoid resistance
- Major depression
These states are particularly difficult to distinguish from true Cushing's and may require specialized testing.
- Campbell Walsh Wein Urology, p. 3138
6. Diagnosis
Diagnosis is a two-step process: (1) confirm hypercortisolism, then (2) identify the cause.
Step 1: Confirm Cushing's Syndrome
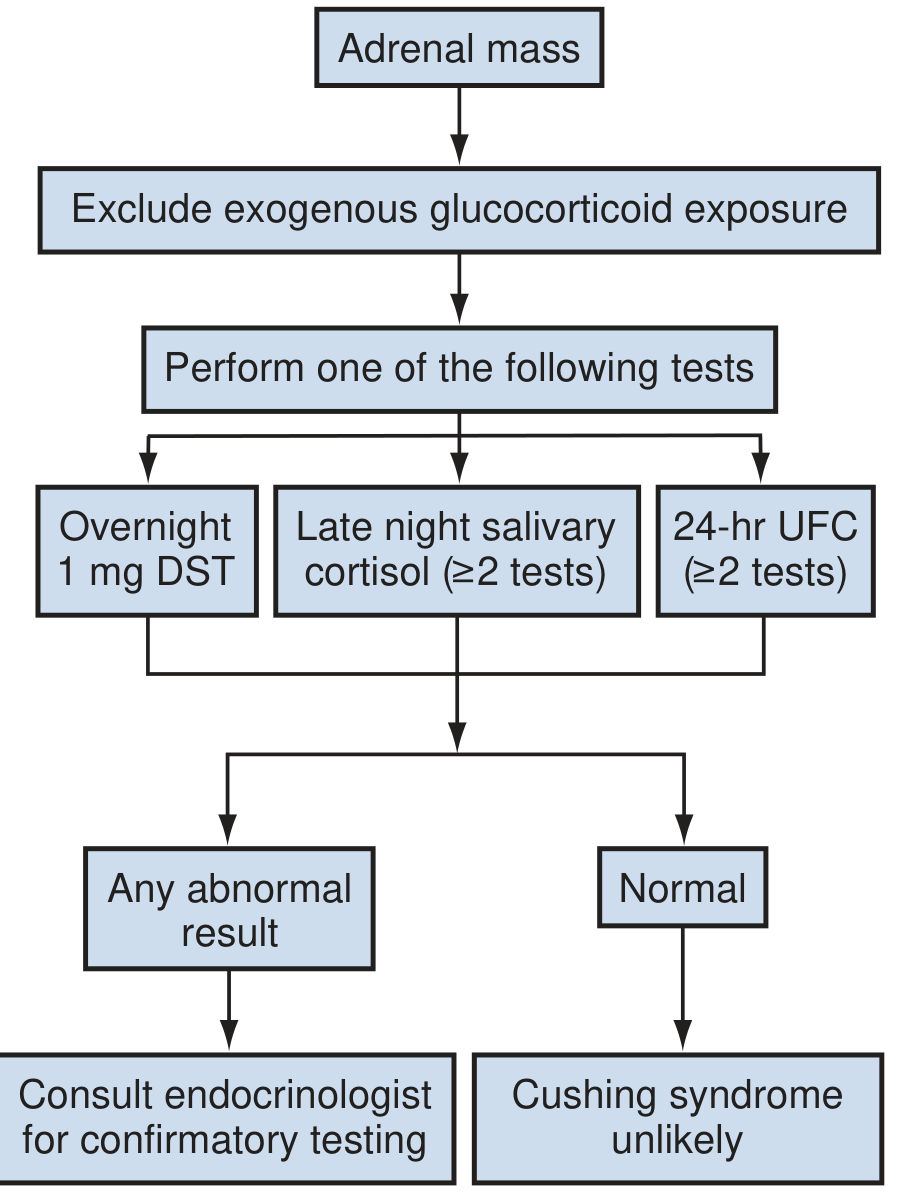
First, exclude exogenous glucocorticoid use (careful drug history). Then perform one or more of:
| Test | Details | Cut-off/Notes |
|---|---|---|
| Overnight 1 mg dexamethasone suppression test (DST) | 1 mg dexamethasone at 11 PM; plasma cortisol at 8 AM | Cortisol <50 nmol/L = normal (rules out Cushing's) |
| 24-hour urinary free cortisol (UFC) | ≥2 collections recommended | ≥3x upper limit of normal = 95-100% sensitive and specific |
| Late-night salivary cortisol | ≥2 samples recommended | Exploits the lost circadian nadir; highly sensitive |
| Low-dose DST (2 mg/48 hrs) | More thorough confirmation | Used when overnight DST equivocal |
Repeat testing is prudent when any single result is positive. Late-night plasma cortisol >207 nmol/L is also highly suggestive.
Step 2: Identify the Cause - Localization
Measure serum ACTH:
-
Low ACTH (<10 pg/mL) → ACTH-independent → adrenal imaging (CT/MRI of adrenals)
- Normal adrenals → suspect exogenous steroids or PPNAD (check for paradoxical cortisol rise on DST)
- Bilateral lesions → consider adrenal venous sampling (AVS)
-
High ACTH (>20 pg/mL) → ACTH-dependent → need to distinguish pituitary vs. ectopic
Distinguishing pituitary from ectopic ACTH:
-
MRI of the pituitary (gadolinium-enhanced) - microadenomas found in only ~50% of Cushing's disease
-
High-dose DST (8 mg overnight): Cushing's disease typically suppresses; ectopic ACTH syndrome does NOT suppress
-
CRH stimulation test: pituitary adenomas respond with ACTH/cortisol rise; ectopic tumors typically do not
-
Inferior petrosal sinus sampling (IPSS) - gold standard for distinguishing pituitary from ectopic; requires expertise at specialized centers
-
CT chest/abdomen for ectopic tumors
-
Campbell Walsh Wein Urology, pp. 3138-3142 | Andrews' Diseases of the Skin, p. 3834 | Fitzpatrick's Dermatology, p. 578
7. Management
A. Surgery - First-Line
Cushing's Disease (pituitary):
- Transsphenoidal surgery (TSS) - treatment of choice; remission rates 65-90% for microadenomas, lower for macroadenomas
- If pituitary adenoma cannot be found or resected, bilateral adrenalectomy is an option
- Radiation (stereotactic radiosurgery / conventional) as adjunct or second-line
ACTH-Independent adrenal causes:
- Adrenalectomy - laparoscopic preferred for unilateral disease
- Bilateral adrenalectomy for bilateral disease (AIMAH, PPNAD)
- Cushingoid phenotype resolves in 7-9 months post-adrenalectomy; may persist years in some
Ectopic ACTH:
- Resect primary tumor if possible
- Bilateral adrenalectomy if tumor not resectable
B. Perioperative Management (especially adrenalectomy)
Pre-operative:
- Metyrapone to block cortisol production when severe symptoms (hypertension, DM, hypokalemia, myopathy)
- Correct hypertension and hyperglycemia
- VTE prophylaxis (high thrombotic risk)
- Preoperative antibiotics
- Stress-dose steroid administration intraoperatively
Post-operative:
- Replacement glucocorticoids mandatory (the contralateral/remaining adrenal is suppressed and requires time to recover)
- Monitor for adrenal insufficiency
- Bone mineral density (BMD) improves after resolution - recent meta-analysis (PMID: 39689783) confirms significant BMD recovery post-cure
C. Medical Therapy
Used as bridge to surgery, or when surgery is not possible:
| Drug | Mechanism | Notes |
|---|---|---|
| Metyrapone | 11β-hydroxylase inhibitor; blocks cortisol synthesis | Rapid onset; most commonly used |
| Ketoconazole | Multiple steroidogenesis enzymes; blocks cortisol and androgen synthesis | Risk of hepatotoxicity |
| Mitotane | Adrenolytic; used for adrenocortical carcinoma | Slow onset; toxic |
| Osilodrostat | 11β-hydroxylase inhibitor | Newer agent |
| Mifepristone | Glucocorticoid receptor antagonist | Useful when surgical cure not possible |
| Pasireotide | Somatostatin receptor agonist → reduces ACTH from pituitary | For Cushing's disease |
| Cabergoline | Dopamine agonist | Some response in Cushing's disease |
D. Radiation
-
Stereotactic radiosurgery (Gamma Knife) for residual/recurrent pituitary tumors
-
Conventional fractionated radiation as alternative
-
Onset of effect is delayed (months to years)
-
Campbell Walsh Wein Urology, pp. 3142-3150 | Braunwald's Heart Disease, p. 1141
8. Prognosis and Complications
-
Untreated Cushing's syndrome carries significantly elevated mortality, primarily from cardiovascular events and infections
-
Venous thromboembolism is a major cause of death; prophylaxis is essential
-
Cardiovascular risk persists even after cure - cardiac structural changes can take years to reverse
-
Bone density recovers after successful treatment, though may not fully normalize
-
Psychiatric symptoms often persist or take months to resolve post-cure
-
Nelson's syndrome: after bilateral adrenalectomy for Cushing's disease, the underlying pituitary tumor can expand aggressively due to loss of cortisol feedback, causing hyperpigmentation and mass effects
-
Braunwald's Heart Disease, pp. 1141-1142 | Campbell Walsh Wein Urology, p. 3150
9. Special Situations
Subclinical Cushing's syndrome: Biochemical evidence of hypercortisolism without the full clinical picture; discovered incidentally on adrenal imaging. Management is debated - surgery vs. watchful waiting. A 2024 meta-analysis (PMID: 39086899) examined surgical vs. conservative approaches for mild autonomous cortisol secretion.
Cyclic Cushing's: Intermittent hypercortisolism making diagnosis elusive; multiple UFC measurements improve detection.
Pediatric Cushing's: Growth retardation is an early sign; adrenal carcinoma is relatively more common than in adults.
MEN1 / Carney Complex: Cushing's syndrome occurs as part of hereditary syndromes and should prompt genetic evaluation.
Summary Table
| Feature | Details |
|---|---|
| Definition | Prolonged excess glucocorticoid exposure |
| Most common cause | Exogenous steroids (iatrogenic) |
| Most common endogenous cause | Cushing's disease (pituitary microadenoma) |
| Female:male ratio | ~4:1 (non-iatrogenic) |
| Key classic signs | Central obesity, moon facies, buffalo hump, purple striae, easy bruising, proximal myopathy |
| First-line screening test | Overnight 1 mg DST + 24-hr UFC |
| Distinguish ACTH-dep vs. indep | Serum ACTH level |
| Best test pituitary vs. ectopic | Inferior petrosal sinus sampling (IPSS) |
| First-line treatment | Surgery (transsphenoidal or adrenalectomy depending on cause) |
| Main cause of death | VTE and cardiovascular disease |
Sources: Campbell Walsh Wein Urology, 3e | Fitzpatrick's Dermatology | Andrews' Diseases of the Skin | Braunwald's Heart Disease | PubMed (PMIDs 39086899, 39689783)
This is a shared conversation. Sign in to Orris to start your own chat.