Interstitial lung disease
Reading File
Finding Sources
Searching PubMed
"interstitial lung disease"[MeSH Terms] AND diagnosis AND management
Reading File
Reading File
Searching PubMed
"interstitial lung disease"[MeSH Terms] AND treatment
Finding Sources
Finding Sources
Searching PubMed
"idiopathic pulmonary fibrosis"[MeSH Terms] AND ("antifibrotic" OR "nintedanib" OR "pirfenidone")
Reading File
Reading File
Reading Article
PMID: 40387033
Reading Article
PMID: 41812190
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive material to write a thorough, well-structured answer on ILD. Let me compile the final response.
Interstitial Lung Disease (ILD)
Interstitial lung diseases (ILDs) are a large, heterogeneous group of more than 200 conditions that affect the lung parenchyma - primarily the interstitial space (between the epithelium and endothelium) - with varying degrees of inflammation and fibrosis. Despite the diversity, the vast majority of patients present with progressive exertional dyspnea and/or a persistent dry cough.
- Harrison's Principles of Internal Medicine 22E, Chapter 304
Classification
ILDs are broadly categorized by their underlying cause:
| Category | Examples |
|---|---|
| Idiopathic interstitial pneumonias (IIPs) | IPF, NSIP, COP, AIP, RB-ILD, DIP, LIP |
| Connective tissue disease (CTD)-associated | SSc-ILD, RA-ILD, DM/PM-ILD, SLE-ILD |
| Granulomatous | Sarcoidosis, hypersensitivity pneumonitis |
| Occupational/environmental | Silicosis, asbestosis, berylliosis |
| Drug-induced | Amiodarone, methotrexate, bleomycin |
| Other | LAM, pulmonary alveolar proteinosis |
The major idiopathic IIPs and their key clinical features:
| IPF | NSIP | RB-ILD | SSc-ILD | Sarcoidosis | |
|---|---|---|---|---|---|
| Symptoms | Gradual SOB, dry cough; older adults | Subacute SOB; often with CTD | Can be asymptomatic | SOB + skin tightening, Raynaud's | SOB/cough; eye, skin, joint findings |
| Physical exam | Basal rales; digital clubbing common | Rales; clubbing less common | Rales common; clubbing rare | Rales ± skin thickening | Often normal; lymphadenopathy |
| Key exposure | Idiopathic; smoking common | Often CTD-associated | Strong smoking link | Unknown | Unknown |
Pathogenesis
ILD pathogenesis varies by type, but common threads include:
- Epithelial injury - recurrent microinjury to alveolar epithelial type II cells triggers aberrant repair
- Fibroblast/myofibroblast activation - driven by TGF-β, connective tissue growth factor (CTGF), endothelin-1
- Immune dysregulation - CD45Ro+ memory T cells, Th1/Th2 cytokine imbalance, germinal centers in CTD-ILD
- Pro-inflammatory cytokines - IL-8, TNF-α, MIP-1α, RANTES accumulate in BAL fluid
- Genetic susceptibility - MHC class II associations (especially in SSc), MUC5B promoter variant (linked to UIP/IPF phenotype in RA-ILD)
In SSc-ILD, the Scl-70 (anti-DNA topoisomerase) antibody drives immune responses; TGF-β is present in high amounts in the lung and leads to excessive collagen biosynthesis. - Murray & Nadel's Textbook of Respiratory Medicine
Clinical Features
Symptoms:
- Progressive exertional dyspnea (most common)
- Dry, nonproductive cough
- Fatigue, weight loss in advanced disease
- Extrapulmonary features when associated with CTD (skin changes, joint swelling, Raynaud's phenomenon)
Physical examination:
- Bibasilar "Velcro" crackles (fine inspiratory rales) - hallmark finding
- Digital clubbing (especially in IPF)
- Signs of pulmonary hypertension in advanced disease (RV heave, loud P2)
- Cyanosis in end-stage disease
Pulmonary function tests (PFTs):
- Restrictive pattern: reduced TLC, FVC, FEV1/FVC ratio preserved or elevated
- Reduced DLCO - often the most sensitive early marker
- Reduced 6-minute walk distance (6MWD)
Diagnosis
Step 1 - History and Exposure Assessment
Identify potential causes: occupational dusts, drug exposures, CTD features, family history of pulmonary fibrosis.
Step 2 - HRCT Chest
HRCT is the cornerstone of ILD diagnosis. The following illustrates key patterns across the four main ILD subtypes:
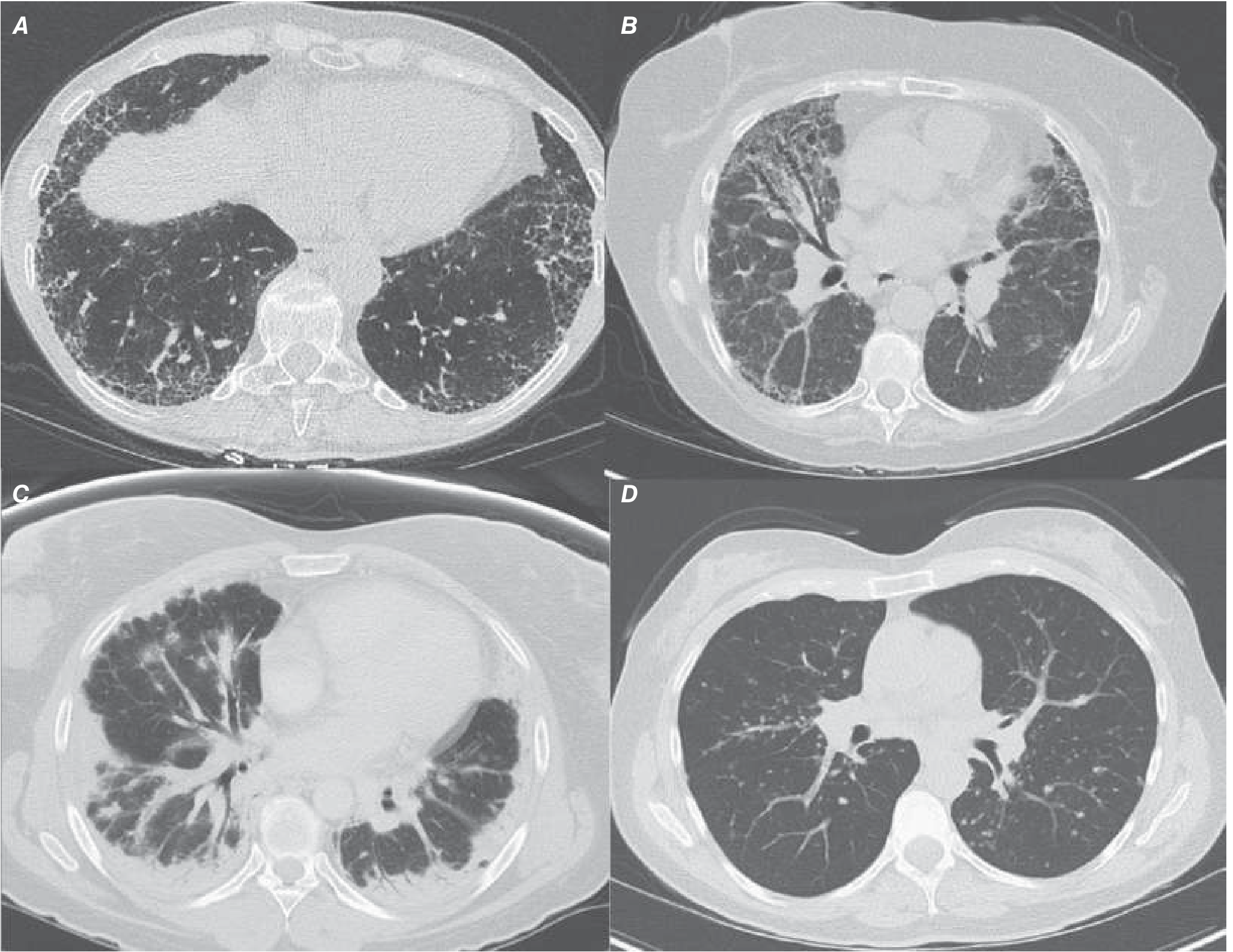
| Pattern | Key HRCT Features |
|---|---|
| UIP (IPF) | Subpleural, posterior-basilar reticulation; honeycombing; traction bronchiectasis |
| NSIP | Bilateral ground-glass opacities; subpleural sparing; bronchovascular thickening |
| COP | Subpleural/peribronchial consolidation; "reversed halo (atoll) sign" |
| Sarcoidosis | Bilateral hilar lymphadenopathy; perilymphatic nodules along bronchovascular bundles |
| HP | Upper/mid lung predominance; mosaic attenuation; centrilobular nodules |
Step 3 - Diagnostic Algorithm for IPF
The diagnostic algorithm for IPF per joint society guidelines:
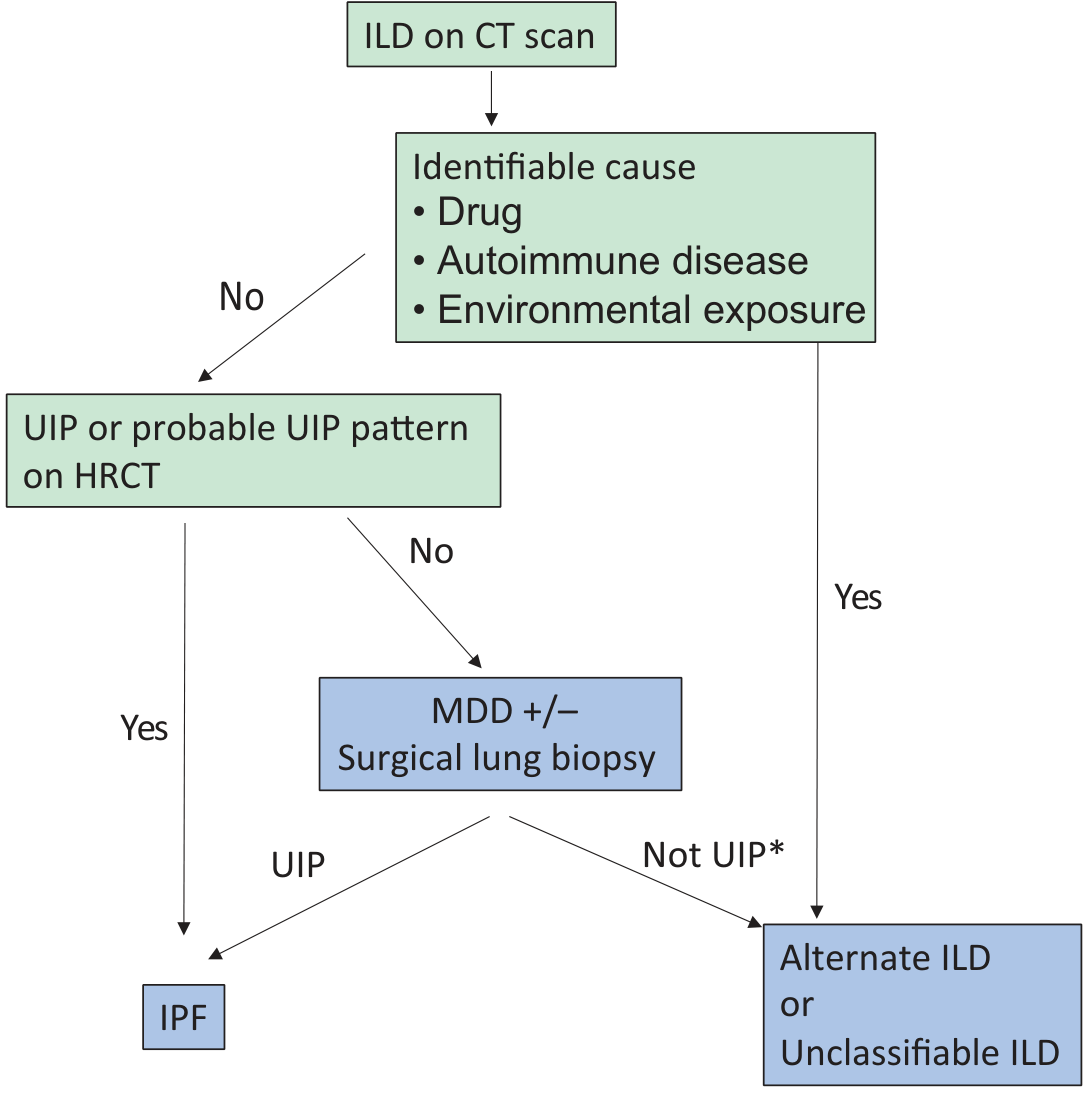
IPF diagnostic criteria (ATS/ERS/JRS/ALAT):
- Exclusion of other known causes (CTD, drugs, occupational exposures)
- AND either:
- HRCT showing a UIP pattern, OR
- Specific HRCT + histopathology UIP combination (surgical lung biopsy showing subpleural honeycombing + fibroblast foci with temporal/spatial heterogeneity)
Step 4 - Serologies and BAL
- ANA, anti-dsDNA, RF, anti-CCP, anti-Scl-70, anti-Jo-1, anti-synthetase antibodies
- BAL cellular differential (lymphocytosis suggests HP or NSIP; eosinophilia suggests eosinophilic pneumonia)
- Transbronchial cryobiopsy - yields diagnostic histopathology in ~80% of cases; has largely supplanted VATS biopsy in many centers
Major ILD Entities
Idiopathic Pulmonary Fibrosis (IPF)
- Most common ILD of unknown cause; prevalence 50-200/100,000
- Typically men in the 5th-6th decade; strong association with smoking
- UIP is the histopathologic pattern: fibroblast foci, honeycombing, temporal/spatial heterogeneity
- Poor prognosis: estimated 50% 3-5 year survival
- Complicated by pulmonary hypertension (PH) in 30-50%, which dramatically worsens prognosis (median survival <1 year when PASP >50 mmHg)
NSIP
- Bilateral symmetric ground-glass opacities; subpleural sparing
- Commonly associated with CTD (especially SSc, DM/PM)
- Responds better to immunosuppression than IPF; better prognosis
- Histology: uniform interstitial fibrosis without fibroblast foci; temporally homogeneous
Cryptogenic Organizing Pneumonia (COP)
- Subacute onset; bilateral subpleural consolidation; reversed halo sign
- Responds dramatically to corticosteroids (>80% response)
- Can relapse on steroid taper
Hypersensitivity Pneumonitis (HP)
- Caused by inhaled antigens (bird proteins, molds, chemicals)
- Acute, subacute, and chronic forms
- Chronic HP can be fibrotic and difficult to distinguish from IPF
CTD-ILD
- SSc-ILD: Most common CTD-ILD; NSIP pattern predominates; treat with mycophenolate or cyclophosphamide
- RA-ILD: Male predominance (3:1); both UIP and NSIP patterns; UIP carries worse prognosis
- DM/PM-ILD: Up to 45% with anti-synthetase antibodies develop ILD; anti-Jo-1 most common; NSIP ± COP pattern
Treatment
General Measures (all ILDs)
- Smoking cessation - essential
- Supplemental oxygen when indicated (improves exercise tolerance, reduces PH risk)
- Pulmonary rehabilitation - improves exercise capacity and quality of life
- Treat comorbidities - GERD (microaspiration is a trigger), PH, sleep apnea
- Vaccinations - influenza, pneumococcal
Antifibrotic Therapy (IPF)
Two antifibrotic agents are approved for IPF and shown in Phase 3 trials to slow FVC decline:
| Drug | Mechanism | Key Evidence |
|---|---|---|
| Pirfenidone | Anti-fibrotic, anti-inflammatory, antioxidant | ASCEND, CAPACITY trials (2014) |
| Nintedanib | Triple kinase inhibitor (VEGFR, FGFR, PDGFR) | INPULSIS trials (2014); also approved for progressive pulmonary fibrosis |
Nintedanib has also been approved for progressive pulmonary fibrosis (PPF) beyond IPF (including SSc-ILD), based on the INBUILD trial.
Emerging Treatments (2025-2026 data)
Two landmark Phase 3 RCTs published in the New England Journal of Medicine have expanded the IPF treatment landscape:
1. Nerandomilast (FIBRONEER-IPF, NEJM 2025) - PMID 40387033
- Preferential PDE4B inhibitor with antifibrotic and immunomodulatory effects
- 1,177 patients (77.7% already on nintedanib or pirfenidone)
- Nerandomilast 18 mg BID vs placebo: FVC decline -114.7 ml vs -183.5 ml (difference +68.8 ml, p<0.001)
- Effective on top of standard antifibrotic therapy
- Main adverse effect: diarrhea (41.3% with 18 mg dose)
2. Inhaled Treprostinil (TETON-2, NEJM July 2026) - PMID 41812190
- A prostacyclin analog previously used for pulmonary hypertension; has antifibrotic preclinical data
- 593 patients; 75.4% on background antifibrotic therapy
- Treprostinil vs placebo: FVC change -49.9 ml vs -136.4 ml (difference +95.6 ml, p<0.001)
- Also reduced clinical worsening (HR 0.71; p=0.02)
- Main adverse effect: cough (48.3% vs 24.1%)
These trials suggest that combination antifibrotic regimens may become standard of care for IPF.
Immunosuppression
- Not indicated in IPF - the PANTHER trial showed immunosuppression (prednisone + azathioprine + NAC) increased mortality in IPF
- Used in CTD-ILD (SSc, RA, DM/PM):
- Mycophenolate mofetil (first-line for SSc-ILD; SLS II trial)
- Cyclophosphamide (SLS I trial; induction for severe/rapidly progressive CTD-ILD)
- Rituximab for refractory DM/PM-ILD
- Corticosteroids for COP, HP (acute), sarcoidosis
Lung Transplantation
- Remains the only option that can extend survival in advanced IPF
- Bilateral lung transplant preferred over single-lung transplant
- Pre-transplant PH significantly increases risk of primary graft dysfunction
- Combined emphysema + pulmonary fibrosis: PH prevalence 30-50%, 1-year survival as low as 48% if PVR elevated
Monitoring and Prognosis
- Serial PFTs every 3-6 months: >10% decline in FVC or >15% decline in DLCO indicates disease progression
- 6-minute walk test: distance and oxygen desaturation are prognostic markers
- HRCT: progression of fibrosis (honeycombing, traction bronchiectasis)
- GAP index (Gender, Age, Physiology): validated prognostic model for IPF based on FVC and DLCO
Poor prognostic factors in IPF:
- Extensive fibrosis on HRCT
- Low DLCO (<40% predicted)
- PH at rest (mPAP >25 mmHg)
- Rapid FVC decline (>10%/year)
- Acute exacerbations (5-10% annual incidence; 50-90% in-hospital mortality)
Summary Table
| Feature | IPF | NSIP | COP | HP |
|---|---|---|---|---|
| Demographics | Older men, smokers | Middle-aged women, CTD | Any age | Any age (exposure-linked) |
| HRCT | Honeycombing, basal reticulation | GGO, subpleural sparing | Subpleural consolidation | Upper/mid GGO, mosaic |
| Histology | UIP (fibroblast foci, heterogeneous) | Uniform fibrosis, no foci | Intraluminal fibrosis (Masson bodies) | Peribronchiolar granulomas |
| Prognosis | Poor (50% 5-yr survival) | Moderate-good | Good (steroid-responsive) | Variable (chronic worse) |
| Treatment | Pirfenidone/nintedanib | Immunosuppression | Steroids | Antigen avoidance ± steroids |
Sources: Harrison's Principles of Internal Medicine 22E (Ch. 304), Murray & Nadel's Textbook of Respiratory Medicine (Ch. 92, 20), Goldman-Cecil Medicine (Ch. 80).
2026 Update: The TETON-2 trial (PMID 41812190) published in NEJM July 2026 demonstrated inhaled treprostinil significantly reduces FVC decline and clinical worsening in IPF - a potential new treatment paradigm. The FIBRONEER-IPF trial (PMID 40387033) in 2025 showed nerandomilast (PDE4B inhibitor) also slows IPF progression even in patients already on standard antifibrotics.
Bronchodilators
Reading File
Finding Sources
Searching PubMed
"bronchodilators"[MeSH Terms] AND ("COPD" OR "asthma") AND pharmacology
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I have all the information needed. Let me now compose the comprehensive answer.
Bronchodilators
Bronchodilators are drugs that relax constricted airway smooth muscle, causing immediate reversal of airway obstruction in conditions such as asthma and COPD. They may act directly (relaxing smooth muscle) or indirectly (blocking bronchoconstrictor mediators/neurotransmitters). They do not suppress airway inflammation - that is the role of corticosteroids.
Three major classes are in clinical use:
- β₂ Adrenergic agonists (sympathomimetics)
- Anticholinergic agents (muscarinic receptor antagonists)
- Methylxanthines (theophylline)
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Ch. 44
1. β₂ Adrenergic Agonists
Chemistry
Derived from the catecholamine structure of epinephrine by substitutions on the catechol ring and terminal amine group. Modifications at the amine confer β₂ selectivity. All approved inhaled β₂-selective agonists have similar selectivity; differences are mainly in duration of action.
Mechanism of Action
β₂ receptor activation triggers the Gs → adenylyl cyclase → cAMP → PKA pathway, leading to:
- Opening of Ca²⁺-activated K⁺ channels → membrane hyperpolarization
- Decreased phosphoinositide hydrolysis
- Decreased myosin light chain kinase (MLCK) activity + increased MLC phosphatase activity
- Net result: smooth muscle relaxation regardless of the bronchoconstrictor stimulus (functional antagonism)
Additional indirect effects include:
- Inhibition of mast cell mediator release
- Reduction of microvascular leakage (reduces mucosal edema)
- Enhanced mucociliary clearance (increased ion transport, mucus secretion)
- Presynaptic β₂ receptor activation → inhibits ACh release from cholinergic nerves
Key point: β₂ agonists do NOT suppress chronic airway inflammation - regular use does not reduce eosinophils or activated inflammatory cells in the airways.
Classification by Duration
| Class | Duration | Examples | Route | Use |
|---|---|---|---|---|
| SABA (Short-Acting) | 3-6 h | Albuterol (salbutamol), levalbuterol, terbutaline | MDI, nebulizer | Rescue/reliever therapy |
| LABA (Long-Acting) | 12 h | Salmeterol, formoterol | DPI, MDI | Maintenance (must be with ICS in asthma) |
| Ultra-LABA | >24 h | Indacaterol, vilanterol, olodaterol | DPI, SMI | Once-daily maintenance in COPD |
Mechanism of prolonged action:
- Salmeterol - long aliphatic side chain anchors to an "exosite" within the receptor binding cleft
- Formoterol - bulky substitution + moderate lipophilicity keeps the drug in the membrane near the receptor (slow-release effect); also has rapid onset and can serve as reliever
- Ultra-LABAs (indacaterol, vilanterol, olodaterol) - exceed 24 h duration; once-daily dosing
Clinical Use
In Asthma:
- SABAs (albuterol) are the first-line rescue therapy for acute symptoms
- If symptoms require rescue >2×/week, FEV₁ <80% predicted, or nocturnal symptoms >2×/month → add low-dose ICS
- LABAs are never used as monotherapy in asthma (risk of fatal attacks without ICS coverage); always combined with ICS
- GINA guidelines recommend budesonide/formoterol combination as both maintenance AND reliever (SMART/AIR strategy)
In COPD:
- SABAs and long-acting agents both used; inhaled bronchodilators are the foundation of COPD treatment
- Regular maintenance with LABA and/or LAMA reduces dyspnea and exacerbation frequency
Adverse Effects (β₂ Agonists)
| Effect | Mechanism | Comment |
|---|---|---|
| Tremor | β₂ stimulation of skeletal muscle | Most common; decreases with tolerance |
| Tachycardia/palpitations | β₁ spill-over, reflex | More with systemic/oral routes |
| Hypokalemia | β₂-mediated K⁺ uptake into cells | Clinically relevant with high doses/IV |
| Hyperglycemia | Glycogenolysis, gluconeogenesis | Relevant in diabetics |
| LABA safety concern | Unchecked β₂ stimulation without ICS | FDA black box warning - LABA monotherapy in asthma increases risk of severe asthma attacks and death |
2. Anticholinergic Agents (Muscarinic Antagonists)
Mechanism of Action
Airway smooth muscle is maintained in a degree of resting tone by vagal cholinergic activity via muscarinic M3 receptors. Anticholinergics competitively block muscarinic receptors (primarily M1 and M3), reducing:
- Bronchoconstriction from vagal tone
- Mucus secretion from submucosal glands
Note: M2 receptors on presynaptic cholinergic nerves normally inhibit ACh release (auto-inhibition). Blockade of M2 receptors (as occurs with ipratropium) can paradoxically increase ACh release - this is why ipratropium occasionally causes paradoxical bronchoconstriction.
Classification by Duration
| Class | Duration | Examples | Route | Use |
|---|---|---|---|---|
| SAMA (Short-Acting) | 4-6 h | Ipratropium bromide | MDI, nebulizer | Acute COPD/asthma exacerbations |
| LAMA (Long-Acting) | 24 h | Tiotropium, glycopyrrolate, umeclidinium, aclidinium, revefenacin | DPI, SMI, nebulizer | Once/twice-daily maintenance in COPD; add-on in asthma |
Clinical Use
In COPD:
- LAMAs are first-line maintenance agents; they improve functional capacity and significantly reduce exacerbation frequency
- Tiotropium is the most studied LAMA; shown to reduce exacerbations, hospitalizations, and improve quality of life
- Mixed data on whether LAMAs slow the rate of FEV₁ decline in COPD
In Asthma:
- Ipratropium has modest bronchodilator effect (similar magnitude to β₂ agonists at baseline) but used mainly as an alternative when β₂ agonists are not tolerated
- In acute severe asthma, combination ipratropium + SABA reduces hospitalization rates
- Tiotropium (LAMA) added to ICS in severe asthma is comparable in effect to adding a LABA; adding tiotropium to ICS/LABA triple therapy further reduces exacerbations in patients with persistent obstruction, high symptom burden, and exacerbation history
Adverse Effects (Anticholinergics)
| Effect | Notes |
|---|---|
| Dry mouth | 10-15% with LAMAs; usually resolves with continued use |
| Bitter taste | Ipratropium; contributes to poor compliance |
| Urinary retention | Elderly patients; rare |
| Glaucoma | Nebulized ipratropium via face mask (direct ocular contact); use mouthpiece |
| Paradoxical bronchoconstriction | Mainly with nebulized ipratropium (due to benzalkonium chloride additive or M2 blockade); not seen with tiotropium |
| Constipation | Uncommon |
Systemic anticholinergic effects are rare because inhaled agents have minimal systemic absorption.
3. Methylxanthines (Theophylline)
Mechanism of Action
Multiple mechanisms (not fully understood):
- Non-selective PDE inhibition → ↑ cAMP and cGMP → smooth muscle relaxation
- Adenosine receptor antagonism (A1, A2A) → bronchodilation and reduced bronchoconstriction
- Histone deacetylase (HDAC) activation (at low therapeutic doses) → anti-inflammatory effects; restores steroid sensitivity in COPD and severe asthma
- Stimulation of respiratory center (increases hypoxic/hypercapnic ventilatory drive)
Pharmacokinetics
- Metabolized by CYP1A2 and CYP3A4 in the liver
- Narrow therapeutic window: therapeutic range 5-15 mg/L (or 55-85 μmol/L); toxicity begins at >20 mg/L
- Half-life ~8 h (highly variable): shortened by smoking, enzyme inducers; prolonged by heart failure, liver disease, older age, enzyme inhibitors (e.g., erythromycin, ciprofloxacin, cimetidine)
Clinical Use
- COPD: low-dose theophylline used as add-on when response to inhaled bronchodilators is insufficient; reduces dyspnea, improves mucociliary clearance
- Asthma: third-line agent due to toxicity concerns; sustained-release preparations used as maintenance
- Neonatal apnea: IV aminophylline (theophylline ethylenediamine) or caffeine
Adverse Effects
| Dose/Level | Effects |
|---|---|
| 15-20 mg/L | Nausea, vomiting, headache, insomnia |
| 20-30 mg/L | Sinus tachycardia, tremor, agitation |
| >30-40 mg/L | Seizures (often without warning), severe ventricular arrhythmias |
Drug interactions are a key concern: erythromycin, ciprofloxacin, cimetidine, oral contraceptives, and allopurinol all increase theophylline levels. Rifampicin, phenytoin, and carbamazepine decrease levels.
4. PDE4 Inhibitors (Selective)
Roflumilast (oral) is a selective PDE4 inhibitor approved for COPD with chronic bronchitis and frequent exacerbations:
- Inhibits PDE4 → ↑ cAMP in inflammatory cells (mast cells, eosinophils, neutrophils, T cells, macrophages)
- Anti-inflammatory effect rather than direct bronchodilation
- Used as add-on therapy when patients have repeated exacerbations despite triple inhaler therapy (ICS/LABA/LAMA)
- Side effects: nausea, diarrhea, weight loss, headache, psychiatric effects (depression, suicidal ideation - black box warning)
Inhaled Bronchodilator Drug Reference Table
| Drug | Class | Dose | Formulation | Frequency |
|---|---|---|---|---|
| Albuterol (salbutamol) | SABA | 90 μg/puff | MDI | q4-6h PRN |
| Levalbuterol | SABA | 45 μg/puff | MDI | q4-6h PRN |
| Salmeterol | LABA | 50 μg/dose | DPI | BID |
| Formoterol | LABA | 12 μg/capsule | DPI | BID |
| Indacaterol | Ultra-LABA | 75 μg/capsule | DPI | Once daily |
| Olodaterol | Ultra-LABA | 5 μg | SMI | Once daily |
| Ipratropium | SAMA | 17 μg/puff | MDI | q4-6h |
| Tiotropium | LAMA | 18 μg/dose (DPI); 2.5 μg/puff (SMI) | DPI / SMI | Once daily |
| Aclidinium | LAMA | 400 μg/dose | DPI | BID |
| Umeclidinium | LAMA | 62.5 μg | DPI | Once daily |
| Glycopyrrolate | LAMA | 15.6 μg/dose | DPI | BID |
| Revefenacin | LAMA | 175 μg/3 mL | Nebulizer | Once daily |
- Fishman's Pulmonary Diseases and Disorders, Table 40-7
Fixed-Dose Combination Inhalers (COPD)
| Combination | Drugs | Frequency |
|---|---|---|
| LABA/LAMA | Umeclidinium/vilanterol | Once daily |
| LABA/LAMA | Tiotropium/olodaterol | Once daily |
| LABA/LAMA | Glycopyrrolate/formoterol | BID |
| LABA/LAMA | Ipratropium/albuterol | q6h |
| ICS/LABA/LAMA (triple) | Fluticasone furoate/vilanterol/umeclidinium | Once daily |
| ICS/LABA/LAMA (triple) | Budesonide/formoterol/glycopyrrolate | BID |
| ICS/LABA/LAMA (triple) | Beclomethasone/formoterol/glycopyrrolate | BID |
Triple inhalers are more effective than LABA/LAMA or ICS/LABA combinations at reducing exacerbations in COPD and may also reduce cardiovascular mortality.
Step-Up Approach in COPD
The stepwise pharmacological approach to COPD management:
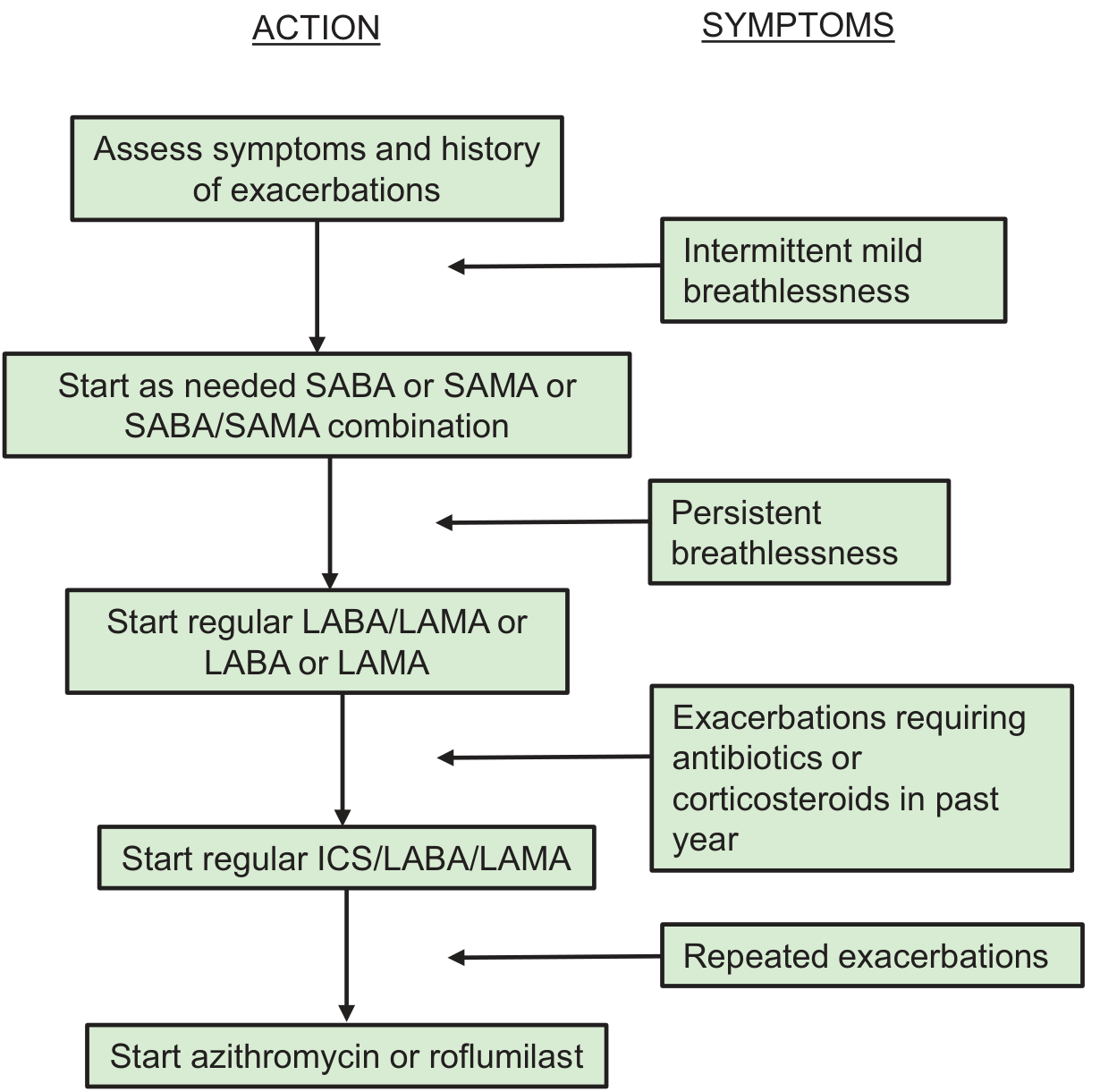
Fishman's Pulmonary Diseases and Disorders, Fig. 40-2
Comparison: β₂ Agonists vs Anticholinergics
| Feature | β₂ Agonists | Anticholinergics |
|---|---|---|
| Primary mechanism | ↑ cAMP → smooth muscle relaxation | Block M1/M3 → reduce vagal tone |
| Onset (SABA) | 1-3 min | 15-30 min |
| Best for | Acute relief (SABA); maintenance (LABA) | COPD maintenance; add-on asthma |
| Systemic side effects | Tremor, tachycardia, hypokalemia | Dry mouth, urinary retention (minimal systemic) |
| Role in asthma | Central (SABA rescue; LABA+ICS maintenance) | Limited (ipratropium as alternative; tiotropium as add-on) |
| Role in COPD | First-line maintenance | First-line maintenance |
| Combination effect | Additive/synergistic with anticholinergics | Additive with β₂ agonists |
Novel Classes in Development
- MABA (Muscarinic Antagonist - Beta Agonist dual action): Single molecule with both LAMA and LABA activities; balancing the two activities has been challenging in development
- Selective PDE inhibitors: PDE4B-selective agents (e.g., nerandomilast - approved for IPF, also under study for airway disease)
- Rho-kinase inhibitors: Target airway smooth muscle contraction at a post-receptor level
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics (Ch. 44), Fishman's Pulmonary Diseases and Disorders (Ch. 40), Katzung's Basic and Clinical Pharmacology 16th Ed., Goldman-Cecil Medicine
Tb meningitis
Finding Sources
Searching PubMed
"tuberculous meningitis"[MeSH Terms] AND treatment
Reading File
Reading File
Searching PubMed
"tuberculous meningitis"[MeSH Terms] AND ("dexamethasone" OR "rifampicin" OR "treatment outcome")
Reading File
Finding Sources
Searching PubMed
"tuberculous meningitis"[MeSH Terms] AND ("intensive phase" OR "dexamethasone" OR "corticosteroid")
Reading File
Loading Image
Finding Sources
Loading Image
Searching PubMed
"tuberculous meningitis" AND diagnosis AND prognosis
Reading Article
PMID: 41406445
I now have everything needed for a comprehensive, well-illustrated answer. Let me compile it.
Tuberculous Meningitis (TBM)
Tuberculous meningitis (TBM) is the most severe and life-threatening form of extrapulmonary tuberculosis. It results in severe disability or death in roughly half of all cases, even with treatment. Caused primarily by Mycobacterium tuberculosis, it is a true meningoencephalitis - the inflammatory process penetrates beyond the subarachnoid space into the brain parenchyma.
- Adams and Victor's Principles of Neurology, 12th Ed., Ch. 31
Epidemiology & Risk Factors
- Incidence parallels systemic TB prevalence; markedly higher in sub-Saharan Africa, South/Southeast Asia
- HIV co-infection is the dominant risk factor: TB incidence is ~500x higher in AIDS patients; TBM may be the first clinical manifestation of HIV
- Other risk factors: alcoholism, malnutrition, extremes of age, immigrants from high-prevalence regions (Asia, Africa, India, former Soviet states)
- Drug-resistant TBM is an increasing concern, particularly with MDR-TB strains
Pathogenesis
TBM follows a two-stage process:
- Bacteremia and seeding: M. tuberculosis reaches the CNS via hematogenous spread (typically from a primary pulmonary focus). Bacilli seed the meninges and subpial brain regions, forming small tubercles (Rich foci) in the meningeal or subependymal layers
- Rupture and subarachnoid spread: One or more tubercles ruptures, discharging bacteria directly into the subarachnoid space, triggering the full meningitic syndrome
In ~2/3 of patients, active TB is found elsewhere at presentation - most commonly in the lungs. In others, only inactive scars or no extracranial focus is found.
TBM may also complicate miliary tuberculosis (hematogenous dissemination), where TB seeds the whole body including the meninges simultaneously.
Pathology
The pathologic changes are concentrated at the base of the brain:
- Thick gelatinous basal exudate obliterates the pontine, interpeduncular, and perimesencephalic cisterns; extends around the medulla, optic chiasm, floor of third ventricle, and undersurfaces of the temporal lobes
- Microscopy: Central caseation → surrounded by epithelioid cells, Langhans giant cells, lymphocytes, plasma cells → fibrin exudate in CSF
- Cranial nerves traversing the basal cisterns are involved more often than in bacterial meningitis (20% of cases at presentation)
- Arteritis: Perforating arteries supplying the basal ganglia, internal capsule, and brainstem undergo inflammatory endarteritis → ischemic infarction (stroke)
- Hydrocephalus: Basal cistern obliteration → communicating hydrocephalus (most common); ependymitis blocking the aqueduct → obstructive hydrocephalus (less common)
- Spinal involvement: Meningeal exudate extends around the cord → myeloradiculitis, posterior/lateral column signs
MRI in TBM - Gadolinium Enhancement of Basal Meninges
The hallmark MRI finding - thick gadolinium enhancement of the basal meninges with multiple ring-enhancing foci (micro-abscesses), accompanied by hydrocephalus and cranial nerve palsies:
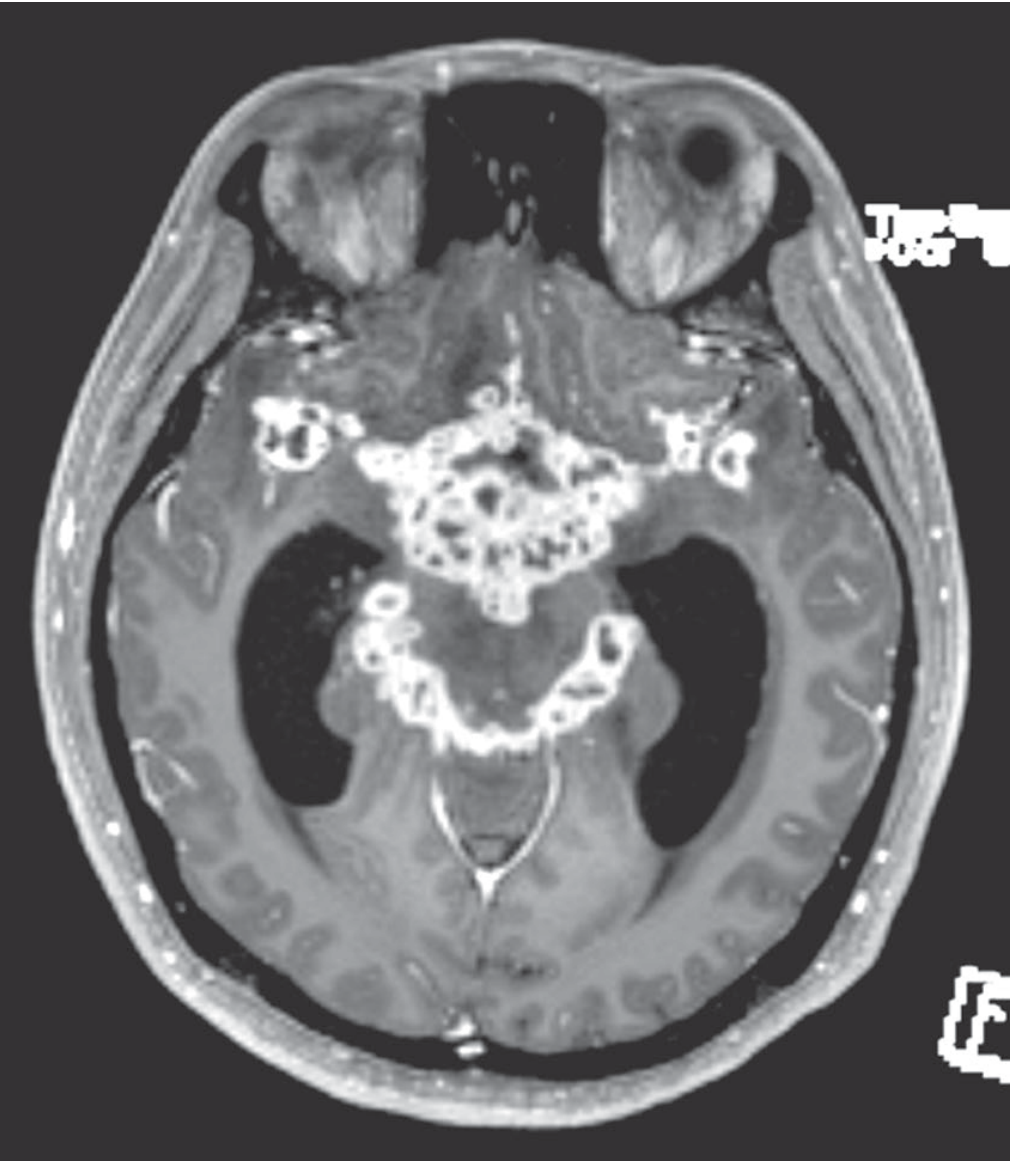
Adams & Victor's Principles of Neurology, Fig. 31-3
Clinical Features
TBM can affect all age groups. In adults in developed countries, it is now seen most often in HIV-positive patients, alcoholics, and immigrants from high-prevalence regions.
Onset
- Subacute - hallmark feature. Symptoms evolve over 1-2 weeks (occasionally longer), in sharp contrast to the hours-to-days of bacterial meningitis
Prodromal symptoms (days to weeks before meningism)
- Low-grade fever
- Malaise, fatigue
- Personality change, irritability
- Headache (>50% of cases)
Meningitic stage
- Persistent headache and fever (most consistent findings)
- Neck stiffness (75% of cases); Kernig and Brudzinski signs
- Confusion, lethargy, altered consciousness
- Nausea, vomiting
Later/advanced features
- Cranial nerve palsies (20% at presentation): CN III, IV, VI (ocular palsies) most common; less often CN VII (facial), CN VIII (deafness)
- Papilledema (raised ICP due to hydrocephalus)
- Focal neurologic deficits from cerebral infarction (basal ganglia, internal capsule)
- Seizures (20-25%)
- Hypothermia and hyponatremia (SIADH is common)
- Stupor and coma in advanced disease
In infants and young children: apathy, hyperirritability, vomiting, and seizures predominate; neck stiffness may be absent, making early diagnosis especially difficult.
British MRC Staging
| Grade | Clinical Description |
|---|---|
| I | Alert and oriented; no focal deficit; GCS 15 |
| II | Altered consciousness (confused/drowsy); minor focal deficit (CN palsy); GCS 11-14 |
| III | Coma or stupor; severe neurologic deficit; GCS ≤10 |
Prognosis is closely tied to MRC grade at presentation - Grade I patients have the best outcomes; Grade III carries very high mortality.
Diagnosis
Lumbar Puncture - CSF Analysis
CSF analysis is the cornerstone of diagnosis:
| Parameter | Typical TBM Finding |
|---|---|
| Opening pressure | Elevated (usually 200-400 mmH₂O) |
| Appearance | Clear or slightly turbid; may form cobweb clot |
| Cell count | 100-500 cells/μL (lymphocytic predominance) |
| Cell type | Initially may be mixed PMN/lymphocyte → rapidly converts to lymphocytic |
| Protein | Elevated - typically 100-500 mg/dL (sometimes >500) |
| Glucose | Low (CSF:serum glucose ratio <0.5; often <0.3) |
| AFB smear | Positive in only 10-40% (low sensitivity) |
| AFB culture | Gold standard but takes 4-8 weeks; sensitivity 45-90% |
| ADA (adenosine deaminase) | Elevated; supports diagnosis |
A CSF glucose:serum protein ratio <0.5 is a key diagnostic clue. CT of the head may be normal in 30% of mild cases, so a normal CT does not exclude TBM.
Key Diagnostic Tests
| Test | Sensitivity | Specificity | Notes |
|---|---|---|---|
| CSF AFB smear | 10-40% | High | Examine multiple samples; concentrate CSF by centrifugation |
| CSF culture | 45-90% | Very high | 4-8 weeks; essential for drug sensitivity |
| CSF NAAT/PCR | ~60-80% | ~98% | Rapid; preferred when available |
| Xpert MTB/RIF (CSF) | ~60% | >98% | Also detects rifampicin resistance |
| CSF ADA | ~60-90% | ~85% | Useful supporting test |
| CSF protein | Universal elevation | Low | Nonspecific |
| Chest X-ray/CT | ~50-60% show active TB | - | Miliary pattern highly suggestive |
| Tuberculin skin test (TST) | Often negative in TBM | - | Negative test does NOT exclude TBM |
| IGRA (blood) | Moderate sensitivity | Moderate | Better than TST in immunocompromised |
MRI/CT Brain
- MRI (with gadolinium) is the preferred neuroimaging modality
- Classic findings: basilar meningeal enhancement, hydrocephalus, infarcts (especially basal ganglia), tuberculomas
- Tuberculoma on MRI: thick ring-enhancing lesion that may mimic brain tumor (see Fig. 31-4)
Before (left) and after (right) anti-TB treatment of a pontine tuberculoma:
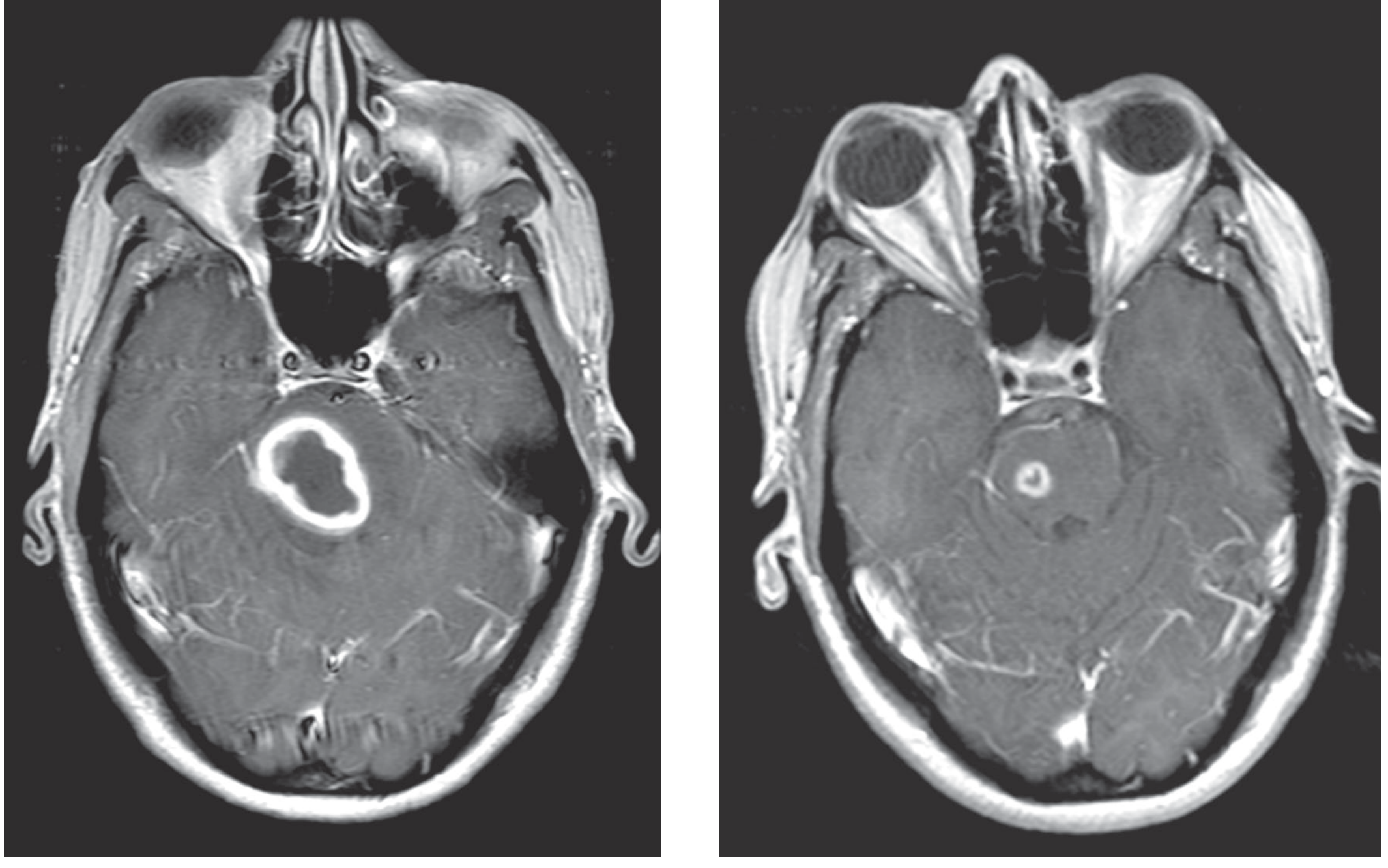
Adams & Victor's Principles of Neurology, Fig. 31-4
Treatment
Antituberculous Drugs
Treatment should begin immediately on clinical suspicion - do not wait for confirmatory culture results.
Intensive Phase (first 2 months): Four-drug regimen
| Drug | Adult Dose | CNS Penetration | Key Adverse Effects |
|---|---|---|---|
| Isoniazid (INH) | 5 mg/kg/day (max 300 mg) | Excellent (70-90% of plasma) | Peripheral neuropathy, hepatitis |
| Rifampicin (RMP) | 10 mg/kg/day adults; 15 mg/kg children | Good (inflamed meninges) | Hepatitis, drug interactions, orange body fluids |
| Pyrazinamide (PZA) | 15-30 mg/kg/day | Excellent | Hepatotoxicity, hyperuricemia/gout, arthralgia |
| Ethambutol (EMB) | 15 mg/kg/day (single daily dose) | Moderate | Optic neuropathy (check visual acuity + red-green color monthly) |
INH and PZA have the best CNS penetration among first-line drugs. Rifampicin penetration is limited with normal meninges but improves significantly with inflammation.
Continuation Phase (months 3-9/12)
- Continue INH + RMP for 7-10 more months (total 9-12 months)
- Some guidelines extend to 12 months for TBM (vs 6 months for pulmonary TB)
- Pyridoxine (vitamin B6) 50 mg/day given with INH to prevent peripheral neuropathy (especially in alcoholics, diabetics, pregnant women, HIV patients)
Alternative Regimen (drug-resistant/severe cases)
- INH + PZA + high-dose RMP + moxifloxacin (fluoroquinolone with excellent CNS penetration)
- In MDR-TBM: add ethionamide (15-25 mg/kg/day in divided doses after meals; risk of optic neuropathy and gastric irritation)
- Duration extended to 18-24 months for MDR-TBM
Corticosteroids (Adjunctive Therapy) - MANDATORY
Dexamethasone is standard of care alongside antituberculous drugs:
- Dose: 0.4 mg/kg/day IV for 2-4 weeks, then tapered over 4-8 weeks (total 6-8 weeks)
- Benefit: Reduces mortality and severe disability, particularly in MRC Grade II-III
- Reduces meningeal inflammation and vasculitis → less ischemic injury
- Particularly beneficial in non-HIV patients; benefit in HIV co-infection is less clear but still recommended
Based on the landmark Thwaites et al. NEJM 2004 trial, dexamethasone reduced 9-month mortality from 41% to 31% in HIV-negative TBM patients. It is now standard of care globally.
Neurosurgical Interventions
- Hydrocephalus requiring intervention: up to 25% of patients
- External ventricular drainage (acute, severe hydrocephalus)
- Ventriculoperitoneal (VP) shunt (communicating hydrocephalus refractory to medical management)
- Endoscopic third ventriculostomy (obstructive hydrocephalus at aqueduct level)
- Repeat lumbar punctures can temporarily reduce ICP
2025 Update - High-Dose Rifampicin Trial
A pivotal Phase 3 RCT published in the New England Journal of Medicine (December 2025) addressed whether increasing rifampicin dose would improve TBM outcomes, given its limited standard-dose CNS penetration:
Trial: NEJM 2025, Meya et al. - PMID 41406445
- 499 adults with TBM in Indonesia, South Africa, Uganda; 60.9% HIV co-infected
- High-dose rifampicin (cumulative 35 mg/kg/day) vs standard dose (10 mg/kg/day) for 8 weeks, on background standard 4-drug therapy
- Primary outcome (6-month mortality): 44.6% vs 40.7% - no significant difference (HR 1.17; p = 0.25)
- High-dose group had earlier deaths (median time to death 13 vs 24 days) and more drug-induced liver injury (8.0% vs 4.4%)
- Conclusion: High-dose oral rifampicin did not improve survival and may be harmful - standard dosing remains the recommendation
Complications
| Complication | Frequency | Notes |
|---|---|---|
| Hydrocephalus | 30-80% | Most common; communicating >> obstructive |
| Cerebral infarction | 20-40% | Basal ganglia, internal capsule; from arteritis of perforating vessels |
| Cranial nerve palsies | ~20% | CN III, IV, VI (ocular); CN VII (facial); CN VIII (auditory) |
| Seizures / status epilepticus | 20-25% | Both at presentation and during treatment |
| Cerebral edema | Common | Contributes to raised ICP |
| Hyponatremia (SIADH) | Common | Requires fluid restriction and/or hypertonic saline |
| Spinal arachnoiditis | Less common | Myeloradiculopathy, cord compression |
| Paradoxical reaction | 10-20% | Worsening after starting treatment; due to immune reconstitution (especially in HIV patients starting ART) |
| TB-IRIS | HIV co-infected | Immune reconstitution inflammatory syndrome on ART initiation |
Prognosis
- Overall mortality: 20-50% (higher in HIV-positive, Grade III, drug-resistant)
- Long-term neurologic sequelae in survivors: ~50%
- Cognitive impairment, memory deficits
- Focal motor deficits from infarction
- Epilepsy
- Cranial nerve deficits (visual loss, hearing loss)
- Hydrocephalus requiring shunting
- Hypothalamic/pituitary dysfunction
- Prognostic factors (poor outcome):
- MRC Grade III at presentation
- HIV co-infection
- Drug-resistant organisms
- Extreme age (infants, elderly)
- Delay in diagnosis and treatment initiation
- Cerebral infarction on imaging
HIV and TBM
- TBM in HIV patients may progress faster with more frequent multi-organ involvement
- ART should be deferred 2-8 weeks after starting anti-TB treatment to reduce risk of TB-IRIS (severe paradoxical worsening from immune reconstitution)
- CD4 count <50 cells/μL: start ART within 2 weeks; CD4 50-200: can defer up to 8 weeks
- HIV treatment does not fundamentally change TBM management but TB-IRIS can be severe and life-threatening
Summary
| Feature | TBM |
|---|---|
| Organism | Mycobacterium tuberculosis (most common) |
| Pathology | Basal gelatinous exudate; caseating granulomas; arteritis |
| Onset | Subacute (1-2 weeks) |
| CSF | Lymphocytic pleocytosis, high protein, low glucose, low opening pressure |
| Key imaging | Basal meningeal enhancement; hydrocephalus; infarcts; tuberculomas |
| Treatment | INH + RMP + PZA + EMB × 2 months, then INH + RMP × 7-10 months |
| Adjunctive | Dexamethasone (mandatory) |
| Prognosis | 20-50% mortality; 50% neurological sequelae in survivors |
Sources: Adams and Victor's Principles of Neurology 12th Ed. (Ch. 31), Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, Henry's Clinical Diagnosis by Laboratory Methods.
2025 Update: The NEJM high-dose rifampicin RCT (PMID 41406445) confirmed that increasing rifampicin dose beyond 10 mg/kg/day does not improve TBM mortality and may be harmful - standard dosing remains the recommendation.
This is a shared conversation. Sign in to Orris to start your own chat.