explain mechanism of labour in detail and easy to understandable way
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the content I need - detailed textbook descriptions, and a clear diagram. Let me now compose the full, detailed, easy-to-understand explanation.
Mechanism of Labour - Complete Explanation
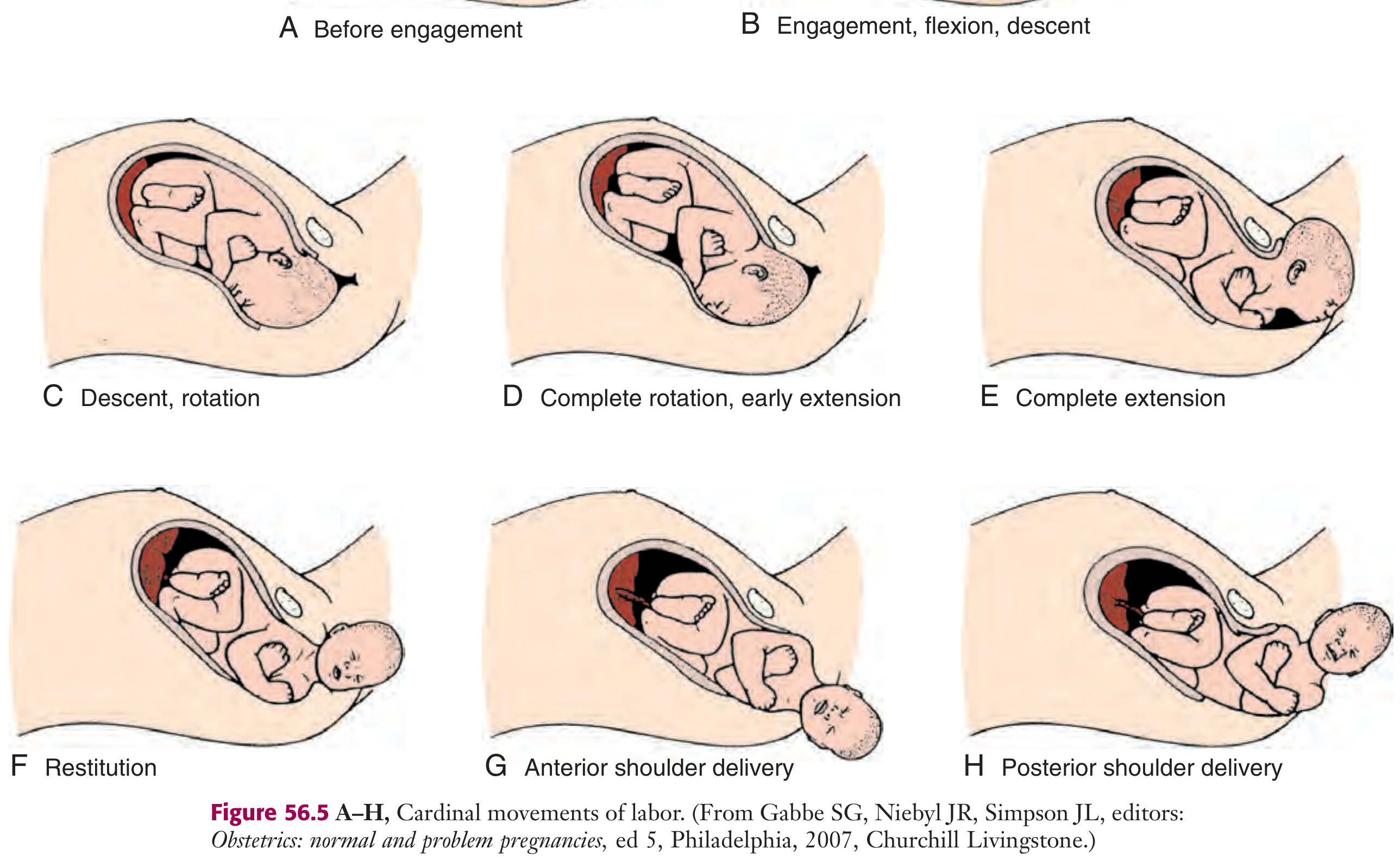
The "mechanism of labour" describes the series of movements a baby's head (and body) makes as it travels through the birth canal. Think of it like navigating a curved tunnel - the baby has to tilt, rotate, and adjust at each turn to fit through the narrowest points. These movements are called the cardinal movements of labour.
Background Concepts to Understand First
Before diving in, a few terms to know:
| Term | What it means (simple) |
|---|---|
| Presenting part | The part of the baby that enters the pelvis first - in 97% of babies at term, this is the head (vertex) |
| Biparietal diameter (BPD) | The widest width of the baby's head (from one parietal bone to the other, ~9.5 cm) |
| Occiput | The back of the baby's head - used as the reference point to describe position |
| Station | How far down the baby has descended (0 station = head is at the level of the ischial spines) |
| Pelvic inlet | The entrance to the pelvis (wider side-to-side = transverse) |
| Pelvic outlet | The exit of the pelvis (wider front-to-back = anteroposterior) |
Key insight: The pelvis is wide transversely (side to side) at the inlet but wide anteroposteriorly (front to back) at the outlet. The baby's head is also an oval - widest from side to side. So the head must ROTATE as it moves down to match the changing shape of the pelvis. This is the whole reason for cardinal movements!
The 7 Cardinal Movements (for Vertex/Head-First Presentation)
Most commonly, the baby presents as occiput anterior (back of the head facing mum's front) - this is the easiest and most favourable position.
1. Engagement
What happens: The widest part of the baby's head (biparietal diameter, ~9.5 cm) passes through the pelvic inlet and enters the pelvis.
Simple analogy: The baby's head "locks in" to the pelvis like putting a key into a keyhole.
- The head enters the inlet in the transverse diameter (sideways) because the inlet is widest side-to-side
- Engagement is confirmed when the presenting part is at 0 station (level with ischial spines)
- In first-time mothers (primiparous), this typically happens in the last 2 weeks of pregnancy
- In women who have delivered before (multiparous), it may only happen at the start of labour
2. Flexion
What happens: The baby's chin tucks toward its chest, making the head as small as possible.
Why it matters: An unflexed head presents a larger diameter (occipitofrontal ~11.5 cm). A fully flexed head presents the smaller suboccipitobregmatic diameter (~9.5 cm) - saving nearly 2 cm, which makes all the difference when fitting through the bony pelvis.
Simple analogy: Think of tucking your chin to your chest before squeezing through a tight gap - you make yourself smaller.
- This happens passively as the head meets resistance from the pelvic floor muscles and bony pelvis
- In most cases, flexion occurs simultaneously with engagement
3. Descent
What happens: The baby moves progressively downward through the birth canal.
- Driven by uterine contractions, abdominal (pushing) effort by the mother, and the straightening of the fetal body
- Descent is gradual and not always continuous - it may pause between contractions
- All other cardinal movements occur alongside descent; they don't happen in a strict separate sequence
Clinical note: Descent is measured in "stations" from -5 (high in pelvis) to +5 (at the introitus/crowning).
4. Internal Rotation
What happens: The baby's head rotates so the occiput (back of the head) moves from the transverse position to the front (anterior), facing the mother's tailbone.
Why it happens: As the head descends to the level of the ischial spines (the narrowest part), the shape of the pelvis forces the head to rotate so the longer axis of the head aligns with the longer (anteroposterior) axis of the pelvic outlet.
- In the most common position (LOT - left occiput transverse), the occiput rotates 45° forward to become occiput anterior (OA)
- This is again a passive movement driven by the shape of the levator ani muscle and the pelvic floor
- Occasionally, the occiput rotates backward (occiput posterior/OP) - this is less favourable and can prolong labour
Simple analogy: Imagine screwing a bolt - as it goes deeper, it has to turn to fit the thread.
5. Extension
What happens: Once the head reaches the vaginal opening (introitus), it extends (lifts up and back), and the face emerges.
Why: The vaginal canal points slightly upward and forward. The baby's head, which came through in a flexed position, now extends around the pubic symphysis like a pivot point.
The sequence of delivery of the head is:
- Occiput appears first (at the introitus/crowning)
- Then the bregma (anterior fontanelle)
- Then the forehead
- Then the nose
- Then the mouth
- Finally the chin emerges
After the head is born, it drops downward so the chin lies over the mother's anal region.
Simple analogy: Think of the baby's head rolling over the edge of a table - the back comes out first, then the face lifts out.
6. External Rotation (Restitution)
What happens: After the head is born, it rotates back to its natural position aligned with the baby's shoulders.
- The head rotates back to the transverse position it was in before internal rotation
- This is called restitution - it's simply the head realigning with the rest of the body
- Meanwhile, the shoulders (which entered the pelvis in a transverse or oblique diameter) now perform their own internal rotation to align anteroposteriorly for delivery
Simple analogy: Like unscrewing that bolt - it naturally unwinds as it comes out.
7. Expulsion
What happens: The rest of the baby's body is delivered.
- Anterior shoulder is delivered first, sliding beneath the pubic symphysis
- Then the posterior shoulder is swept over the perineum
- The rest of the body (trunk, legs) follows quickly, as the widest parts have already passed
Summary Table
| Step | Movement | Key Point |
|---|---|---|
| 1. Engagement | Head enters pelvic inlet | Biparietal diameter passes inlet; 0 station |
| 2. Flexion | Chin tucks to chest | Reduces presenting diameter from ~11.5 to ~9.5 cm |
| 3. Descent | Baby moves down | Driven by contractions + pushing |
| 4. Internal rotation | Occiput rotates to front | Head aligns with anteroposterior outlet diameter |
| 5. Extension | Head lifts out | Occiput pivots under pubic symphysis; face delivers |
| 6. External rotation | Head realigns with shoulders | Passive; shoulders rotate internally |
| 7. Expulsion | Body delivers | Anterior shoulder first, then posterior |
What Drives All This?
The mechanism is not random - it follows the principle of path of least resistance: the baby adapts the smallest possible diameter of its head to the most favourable dimension of the pelvis at each point. Three factors determine how this unfolds:
- Pelvic dimensions and shape (gynecoid pelvis is most favourable)
- Size of the fetus (macrosomia can impede normal mechanism)
- Strength of uterine contractions
Quick Memory Aid - "EFDIEE" or "Every Fetal Descent Involves Elegant Exit"
- Engagement
- Flexion
- Descent
- Internal rotation
- Extension
- External rotation + Expulsion
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine, 6th ed. | Tintinalli's Emergency Medicine: A Comprehensive Study Guide | Textbook of Family Medicine, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.