Create a medical health education topic is prevention of catract in detailed summary and information
Reading File
Checking Date & Time
Finding Sources
Searching PubMed
cataract prevention risk factors
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching Images
cataract types lens opacification diagram
I now have comprehensive information from the textbooks and images. Let me compile the full health education document.
🔍 Health Education Topic: Prevention of Cataract
A Comprehensive Guide for Patients, Caregivers & Health Educators
April 2026
1. What Is a Cataract?
A cataract is the opacification (clouding) of the crystalline lens of the eye. The lens — normally crystal-clear — focuses light onto the retina to produce sharp vision. When it becomes cloudy, light cannot pass through efficiently, causing blurred and dimmed vision.
The lens grows throughout life: new "fiber cells" are laid down beneath the lens capsule, compressing older fibers into the center. By age 45, the lens starts losing flexibility (reducing near vision), and eventually loses its transparency — a process called nuclear sclerosis. In advanced cases, the nucleus turns brown or black, blocking all useful light.
"As the process progresses, the lens loses its transparency, beginning at the center of the lens (nuclear sclerosis). The concurrent change in density of the lens nucleus may alter the optical characteristics of the eye to cause acquired nearsightedness ('second sight')." — Goldman-Cecil Medicine
2. Why Prevention Matters — The Global Burden
Cataract is the leading cause of preventable blindness worldwide. Key facts:
- Affects hundreds of millions of people globally
- Responsible for ~51% of world blindness (WHO estimates)
- Predominantly affects people over age 60, but modifiable risk factors accelerate onset
- Surgery is effective, but access remains limited in low-income countries
- Up to 50% of cataract cases may be preventable or delayable through lifestyle and environmental modifications
3. How the Lens Becomes Opacified — The Pathology
Understanding how cataracts form guides prevention:
| Mechanism | Explanation |
|---|---|
| Oxidative stress | Free radicals damage lens proteins (crystallins), causing them to aggregate and scatter light |
| Protein cross-linking | Lens proteins denature and cross-link, forming insoluble clumps (opacities) |
| Osmotic changes | Excess glucose (in diabetes) forms sorbitol → water influx → cortical lens swelling and vacuoles |
| UV-B radiation damage | Ultraviolet light directly damages DNA and proteins in lens epithelial cells |
| Steroid-induced | Corticosteroids (topical or systemic) cause posterior subcapsular opacities |
"Cortical cataract opacities start as clefts and vacuoles between lens fibres due to cortical hydration." — Kanski's Clinical Ophthalmology, 10th Edition
4. Types of Cataract
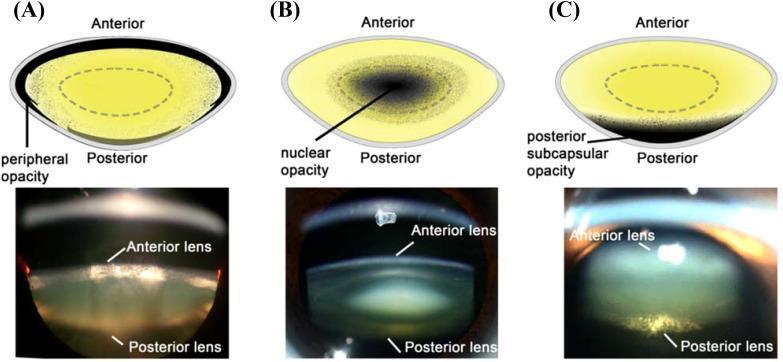
Figure: Educational comparison of the three primary cataract types (cortical, nuclear, posterior subcapsular) with slit-lamp photographic images.
A. Nuclear Sclerotic Cataract
- Most common age-related type
- Yellowing/browning of the central lens nucleus
- Causes gradual blurring, myopic shift ("second sight"), reduced color perception
- Best assessed with oblique slit-lamp illumination
B. Cortical Cataract
- Wedge-shaped ("spoke-like") opacities starting at the lens periphery
- Associated with diabetes and UV radiation exposure
- Causes glare, especially in bright light
C. Posterior Subcapsular Cataract (PSC)
- Located just in front of the posterior lens capsule
- Causes profound glare from car headlights; worsens near vision (miosis)
- Strongly associated with corticosteroid use, diabetes, and radiation
- Progresses faster than nuclear cataract
5. Risk Factors for Cataract
🔴 Non-Modifiable Risk Factors
| Factor | Details |
|---|---|
| Age | Most significant risk factor; exponential increase after age 60 |
| Genetics | Family history increases risk; congenital cataracts can be inherited |
| Race/Ethnicity | Some studies show higher rates of cortical cataract in certain populations |
| Sex | Women have slightly higher lifetime risk (partly due to longer lifespan) |
🟡 Modifiable Risk Factors
| Factor | Details |
|---|---|
| Diabetes mellitus | Osmotic lens changes (sorbitol pathway); accelerates cortical and PSC types |
| Ultraviolet-B (UV-B) radiation | Cumulative occupational or outdoor UV exposure damages lens proteins |
| Cigarette smoking | Increases oxidative stress; dose-dependent risk — doubles risk of nuclear cataract |
| Alcohol excess | Associated with nuclear and cortical cataracts |
| Prolonged corticosteroid use | Topical eye drops, oral, or inhaled — causes posterior subcapsular cataract |
| Obesity | Associated with higher cataract risk (particularly cortical) |
| Hypertension | Vascular mechanisms damage lens nutrition |
| Nutritional deficiencies | Low antioxidant intake (vitamins C, E, lutein, zeaxanthin) linked to higher risk |
| Dehydration / diarrheal illness | Especially in children; disrupts lens osmotic balance |
| Ionizing radiation | X-ray, gamma, microwave exposure (occupational) |
| Intraocular inflammation (uveitis) | Chronic anterior uveitis causes secondary (complicated) cataract |
| High myopia | Associated with early-onset nuclear and posterior subcapsular cataract |
6. Symptoms to Recognize Early
Early recognition allows timely intervention and preservation of quality of life:
| Symptom | Type Often Responsible |
|---|---|
| Blurred or hazy vision (gradual onset) | Nuclear sclerosis |
| Glare from lights (especially at night/headlights) | Posterior subcapsular, cortical |
| Halos around lights | Cortical, PSC |
| Faded or yellowed colors | Nuclear sclerosis |
| Frequent change in glasses prescription | Nuclear (myopic shift) |
| Double vision in one eye | Any type |
| Difficulty reading small print | PSC (worsens with near vision) |
7. Prevention Strategies — Evidence-Based
🛡️ Primary Prevention (Stopping Cataract Before It Starts)
1. Protect Eyes from UV-B Radiation
- Wear UV-400 certified sunglasses outdoors (blocks 100% of UV-A and UV-B)
- Choose wide-brim hats that shade the face and eyes
- Avoid peak UV hours (10 AM – 4 PM) when possible
- Especially important for farmers, fishermen, construction workers, and those living at high altitudes or near equatorial regions
- UV-blocking contact lenses offer additional benefit for contact lens wearers
2. Control Diabetes Mellitus
- Maintain HbA1c < 7% with diet, exercise, and medications
- Good glycemic control delays and reduces the severity of diabetic cataracts (cortical type especially)
- Regular eye exams (annually) for all diabetic patients
3. Stop Smoking
- Smoking doubles the risk of nuclear cataract
- Even former smokers have lower risk than current smokers — quitting at any age reduces risk
- Provide smoking cessation counseling and pharmacotherapy where available
4. Reduce Alcohol Intake
- Limit to recommended safe limits (≤2 standard drinks/day for men; ≤1 for women)
- Excess alcohol depletes antioxidants in the lens
5. Nutrition and Antioxidant-Rich Diet
Strong evidence supports the following dietary measures:
| Nutrient | Food Sources | Role |
|---|---|---|
| Vitamin C | Citrus fruits, bell peppers, broccoli | Powerful antioxidant; highest concentration in healthy lens |
| Vitamin E | Nuts, seeds, vegetable oils | Protects lens cell membranes from oxidative damage |
| Lutein & Zeaxanthin | Leafy greens (kale, spinach), egg yolks, corn | Filter high-energy blue and UV light; concentrate in the lens and macula |
| Beta-carotene/Vitamin A | Carrots, sweet potatoes, leafy greens | Antioxidant; part of the AREDS formulation |
| Omega-3 fatty acids | Oily fish (salmon, sardines), flaxseed | Anti-inflammatory; supports overall eye health |
| Zinc | Oysters, legumes, whole grains | Cofactor in antioxidant enzyme systems |
A diet rich in fruits and vegetables providing antioxidants is strongly associated with reduced risk of nuclear and cortical cataracts.
6. Manage Blood Pressure
- Hypertension accelerates cataract formation
- Control with lifestyle modification (low-sodium diet, exercise) and medications as needed
7. Minimize Corticosteroid Use
- Use corticosteroids only when medically necessary, at the lowest effective dose
- Alert patients using inhaled or topical steroids chronically to undergo annual eye exams
- Never self-medicate with steroid eye drops
8. Occupational and Radiation Protection
- Workers exposed to UV, infrared, or ionizing radiation should use appropriate protective eyewear
- Welders: use certified welding shields; glassblowers: infrared-protective goggles
- Healthcare workers exposed to X-ray should use lead-equivalent protective eyewear
9. Maintain Healthy Body Weight
- BMI in the normal range (18.5–24.9 kg/m²) reduces metabolic cataract risk
- Regular aerobic physical activity (≥150 min/week moderate intensity) supports weight control and metabolic health
10. Prevent Dehydration and Eye Injuries
- Maintain adequate hydration, particularly in hot climates
- Use protective eyewear during sports and occupational hazards to prevent traumatic cataract
- Promptly treat any ocular inflammation or infection
🔵 Secondary Prevention (Early Detection & Slowing Progression)
| Measure | Recommendation |
|---|---|
| Regular eye examinations | Every 1–2 years for adults over 40; annually for diabetics and steroid users |
| Prompt treatment of uveitis | Reduces risk of complicated secondary cataract |
| Treat underlying systemic disease | Diabetes, hypertension — reduces cataract progression |
| Monitor for medication side effects | Alert provider if vision changes on steroids |
| Adjust glasses prescription | Optimizes functional vision during early cataract |
8. Who Is at Highest Risk? — Target Groups for Prevention Education
| Population | Priority Prevention Measures |
|---|---|
| Adults > 60 years | UV protection, nutrition, regular eye exams |
| People with diabetes | Tight glycemic control, annual eye review |
| Corticosteroid users | Minimize dose/duration; annual slit-lamp exam |
| Outdoor workers (farmers, fishermen, construction) | UV-400 sunglasses, wide-brim hats |
| Smokers | Smoking cessation counseling |
| People with chronic uveitis | Treat inflammation, minimize steroids |
| High myopes | Regular monitoring from early adulthood |
9. When to See an Eye Doctor
Seek evaluation promptly if you experience:
- ✅ Gradual blurring of vision not corrected by new glasses
- ✅ Increasing glare, especially at night while driving
- ✅ Halos around lights
- ✅ Rapid change in glasses prescription
- ✅ Colors appearing faded or washed out
- ✅ Difficulty with contrast in low-light conditions
- ✅ Any sudden change in vision (this warrants urgent evaluation)
10. Cataract Surgery — When Prevention Is No Longer Sufficient
Surgery is elective and highly effective when cataract significantly impairs daily life. Key points for patient education:
- Performed as a day procedure under local anesthesia
- Phacoemulsification (ultrasound-assisted lens removal) is the standard technique
- A synthetic intraocular lens (IOL) is implanted to restore focusing power
- Visual prognosis is excellent if the retina is healthy
- Surgery is timed based on how much vision loss affects the patient's lifestyle, not by a specific visual acuity threshold
- Both eyes are treated separately; the worse eye is operated on first
"Cataract surgery, performed as an outpatient, is elective and depends on how much the decreased vision interferes with the normal lifestyle of the patient." — Goldman-Cecil Medicine
11. Key Health Education Messages (Summary)
| # | Take-Home Message |
|---|---|
| 1 | Cataract is the #1 cause of preventable blindness worldwide |
| 2 | Aging is unavoidable, but lifestyle changes can delay onset by years |
| 3 | Wear UV-400 sunglasses every time you are outdoors |
| 4 | Control diabetes — it directly accelerates cataract formation |
| 5 | Quit smoking — it doubles your nuclear cataract risk |
| 6 | Eat a colorful diet rich in leafy greens, fruits, and antioxidants |
| 7 | Minimize unnecessary corticosteroids — always use lowest effective dose |
| 8 | Get regular eye exams — early detection preserves vision options |
| 9 | Cataract surgery is safe and highly effective when needed |
| 10 | Protect your eyes at work — wear appropriate industrial eyewear |
12. References
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition — Sections on Age-related, Acquired, and Secondary Cataract (Ch. 10)
- Goldman-Cecil Medicine, International Edition — Chapter 391: Cataract and Glaucoma
- Robbins & Kumar Basic Pathology / Robbins & Cotran Pathologic Basis of Disease — Cataract (Lens Pathology)
- WHO Global Eye Health Atlas — Cataract burden data
This health education material is intended for use by healthcare providers, health educators, and the general public. It does not replace individualized clinical advice. Patients with vision concerns should be evaluated by a qualified ophthalmologist or optometrist.
This is a shared conversation. Sign in to Orris to start your own chat.