Explain emergency management for hepatic coma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hepatic encephalopathy"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, multi-source information to write a thorough answer. Let me compile everything.
Emergency Management of Hepatic Coma (Hepatic Encephalopathy)
Hepatic coma - more precisely termed hepatic encephalopathy (HE) - is a neuropsychiatric syndrome of altered cerebral function secondary to hepatic dysfunction and/or portal-systemic shunting. It ranges from subtle personality change to deep coma, and should always be regarded as a grave condition with a grim prognosis, though it can be reversed if precipitating factors are corrected.
Pathophysiology (Brief)
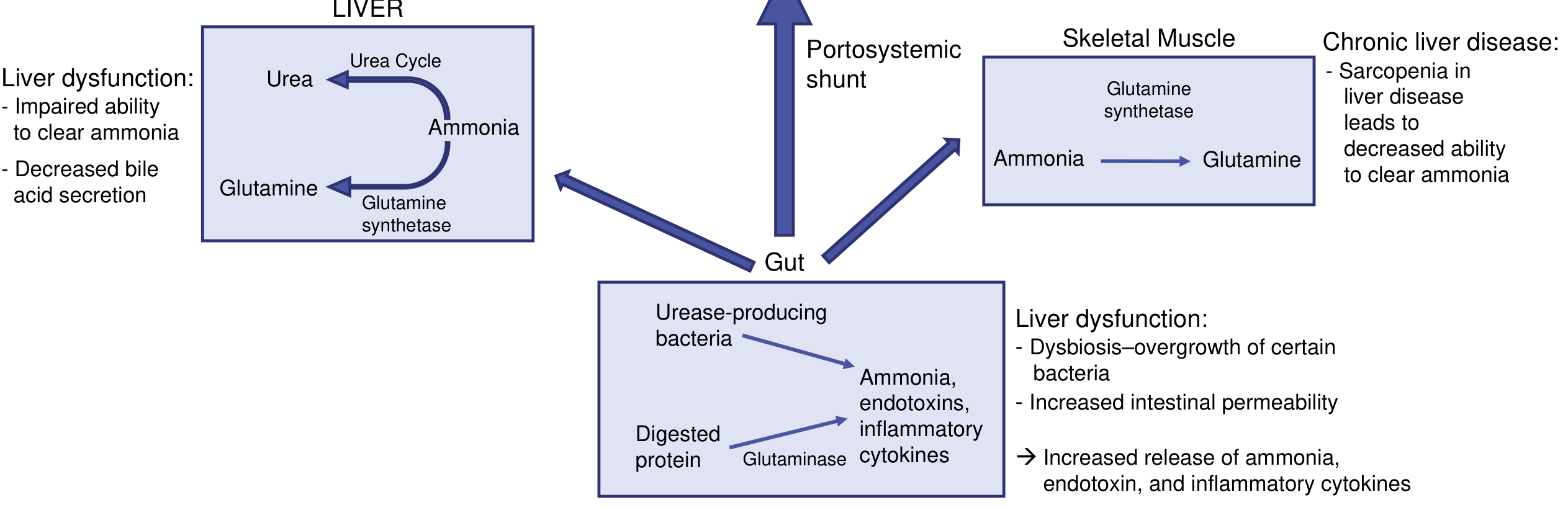
The core mechanism is hyperammonemia from multiple sources:
-
Gut urease-producing bacteria generate ammonia from protein and blood
-
Liver dysfunction impairs the urea cycle (cannot convert NH3 to urea)
-
Portosystemic shunting bypasses hepatic clearance entirely
-
Sarcopenia in chronic liver disease further reduces glutamine synthetase-based ammonia buffering in skeletal muscle
-
Ammonia crosses the blood-brain barrier, causes astrocyte swelling, increased glutamine production, cerebral edema, and neuron dysfunction
-
Current Surgical Therapy 14e, p. 490
Grading of Hepatic Encephalopathy (West Haven Criteria)
| Grade | Category | Clinical Features |
|---|---|---|
| Minimal | Covert | Abnormal neuropsychometric tests only; no clinical signs |
| Grade 1 | Covert | Trivial lack of awareness, euphoria or anxiety, shortened attention span, altered sleep rhythm |
| Grade 2 | Overt | Lethargy/apathy, disorientation to time, inappropriate behavior, asterixis |
| Grade 3 | Overt | Somnolence, gross confusion, gross disorientation |
| Grade 4 | Overt | Coma (hepatic coma proper) |
- Current Surgical Therapy 14e, p. 490
Grade I-II patients who are otherwise stable may be considered for outpatient management with gastroenterology follow-up. Grade III-IV requires immediate hospital admission and emergency management.
- Tintinalli's Emergency Medicine
Precipitating Factors - Identify and Treat
Before treating the coma itself, identify and correct the trigger:
| Precipitant | Mechanism |
|---|---|
| GI hemorrhage | Blood protein broken down by intestinal bacteria produces ammonia load |
| Infection / sepsis | Increased protein catabolism, hypoxia |
| Hypokalemia / alkalosis | Promotes NH3 (uncharged form) entry into CNS |
| Diuretic overuse / dehydration | Electrolyte disturbance, reduced renal NH3 excretion |
| Constipation | Increases colonic ammonia production |
| Sedatives, opiates, benzodiazepines | Decreased hepatic clearance prolongs CNS depression |
| Excessive protein intake | Nitrogen load to gut |
| Portosystemic shunt surgery | Bypasses hepatic detoxification |
| Alcoholic binge | Acute hepatocellular toxicity on chronic disease |
- Adams and Victor's Principles of Neurology 12e, p. 1146
- 22nd Edition Pye's Surgical Handicraft
Emergency Management - Step by Step
1. Airway, Breathing, Circulation (ABC)
-
Intubation is required for Grade III-IV encephalopathy, respiratory failure from ascites/effusions, or risk of aspiration. BPAP is generally not suitable in somnolent patients.
-
Circulatory failure is common due to third-spacing, hemorrhage, and malnutrition. Treat with a judicious normal saline bolus.
-
Vasopressors: norepinephrine is first choice for volume-refractory hypotension. Add vasopressin if escalating doses are needed. Use vasopressin with caution in severe encephalopathy (may worsen cerebral vasodilation and intracranial hypertension).
-
Hydrocortisone may be added for refractory hypotension (AASLD recommendation).
-
Check and treat hypoglycemia urgently - the failing liver has impaired gluconeogenesis and glycogen stores.
-
Tintinalli's Emergency Medicine
2. Nutrition - Restrict and Substitute
-
Nil protein in acute coma: calories are provided by glucose. In the pre-comatose state, glucose drinks; if in frank coma, 20% glucose via intracaval (central) drip.
-
After recovery begins, protein is reintroduced cautiously - only 25-50 g/day, at the limit of tolerance.
-
Full parenteral vitamin supplements, especially vitamins B and K. Vitamin K addresses coagulopathy from hepatic synthetic failure.
-
Branched-chain amino acids (BCAA) have shown benefit without increased mortality and may be added to lactulose + rifaximin.
-
22nd Edition Pye's Surgical Handicraft; Rosen's Emergency Medicine
3. Bowel Decontamination and Ammonia Reduction
This is the central pharmacological strategy.
Lactulose (First-Line)
-
A synthetic, non-absorbed disaccharide. It acidifies the colon, trapping ammonia as NH4+ (non-diffusible form) and increasing nitrogen excretion in stool.
-
Also inhibits glutamine-dependent ammonia production in the gut wall.
-
Oral: Initial 20-30 g every hour until defecation occurs, then reduce to 20-30 g every 4-6 hours. Maintenance: 15-45 mL (20 g) PO bid-qid, titrated to 2-3 soft stools per day.
-
If the patient cannot swallow: lactulose enema - 300 mL lactulose in 700 mL water/normal saline, retained for 30 minutes, repeated every 4-6 hours.
-
Blood ammonia can fall by up to 50% with lactulose therapy.
-
Do NOT give if ileus or bowel obstruction suspected.
-
Washington Manual of Medical Therapeutics; Tintinalli's Emergency Medicine; Current Surgical Therapy 14e
Rifaximin (Add-on / Second-Line)
-
Oral, non-systemic broad-spectrum antibiotic. Suppresses intestinal flora and reduces bacterial ammonia/endotoxin production.
-
Dose: 550 mg PO twice daily (or 400 mg PO every 8 hours per some sources).
-
Recommended in combination with lactulose for overt HE and for prevention of recurrence (Grade IA recommendation, AASLD/EASL).
-
Better tolerated than neomycin; no renal or ototoxic effects.
-
Current Surgical Therapy 14e; Washington Manual; Rosen's Emergency Medicine
Neomycin (Alternative)
-
6 g daily in divided doses, reduces ammonia-forming colonic bacteria.
-
Limited by nephrotoxicity and ototoxicity with prolonged use; reserved for short-term or when rifaximin is unavailable.
-
22nd Edition Pye's Surgical Handicraft; Tintinalli's Emergency Medicine
Purges and Enemas
-
Magnesium sulfate cathartic and colonic enemas are important to clear protein load from the bowel, especially when GI hemorrhage is the precipitant.
-
22nd Edition Pye's Surgical Handicraft
Polyethylene Glycol (PEG) - Alternative
-
PEG-based electrolyte solution: 4 L over 4 hours or 2 L every 12 hours. Emerging evidence it may be more effective than lactulose; further studies needed.
-
Current Surgical Therapy 14e
4. Fluid and Electrolyte Management
-
Maintain strict fluid balance chart; daily serum electrolytes and acid-base estimations.
-
Correct hypokalemia and metabolic alkalosis - both worsen ammonia entry into the CNS.
-
Correct hypo- or hypernatremia (cirrhotic patients on diuretics are at risk for both).
-
Maintain adequate renal perfusion to support ammonia excretion.
-
22nd Edition Pye's Surgical Handicraft; Adams and Victor's 12e
5. Blood Transfusion / Coagulopathy
-
Maintain hemoglobin above 10 g/dL to ensure adequate oxygen delivery to the failing liver.
-
Coagulopathy: Vitamin K 10 mg IV/PO; fresh-frozen plasma for bleeding or pre-procedure; cryoprecipitate (1 unit/10 kg) preferred over FFP for active bleeding.
-
Platelet count should be >50,000/mm3 before invasive procedures.
-
22nd Edition Pye's Surgical Handicraft; Rosen's Emergency Medicine
6. Cerebral Edema Management (Grade III-IV / Fulminant Failure)
Cerebral edema occurs in ~80% of Grade IV HE from fulminant hepatic failure. This is the leading cause of death.
Risk factors for cerebral edema: Grade III-IV HE + renal failure + critically elevated ammonia (>150 µmol/L) + hypotension.
-
Prophylactic hypertonic saline - goal sodium 145-155 mEq/L in high-risk patients.
-
Mannitol 0.5-1 g/kg IV for confirmed raised intracranial pressure.
-
Maintain head elevation at 30 degrees; avoid hyperventilation.
-
Consider ICP monitoring in fulminant hepatic failure with Grade III-IV HE.
-
If intracranial hemorrhage is identified, treat coagulopathy urgently and consult neurosurgery.
-
Tintinalli's Emergency Medicine; Plum and Posner's Diagnosis and Treatment of Stupor and Coma; Current Surgical Therapy 14e
7. Infection Control
-
Sepsis is a major precipitant AND complication of hepatic coma. Screen for and treat infection aggressively.
-
Rule out spontaneous bacterial peritonitis (SBP) in all patients with ascites (diagnostic paracentesis; ascitic granulocytes >250 cells/mm3 is diagnostic; treat with cefotaxime 2 g IV every 8 hours for 5 days).
-
Consider blood cultures and empiric antibiotics for systemic sepsis.
-
Rosen's Emergency Medicine
8. Corticosteroids (Selected Cases)
-
Corticosteroids may be used in acute hepatic coma associated with viral hepatitis.
-
22nd Edition Pye's Surgical Handicraft
9. Liver Transplant Evaluation
-
For fulminant hepatic failure or cirrhosis with refractory encephalopathy, urgent evaluation for liver transplantation is required. This is the only definitive treatment for end-stage disease.
-
Approximately 50% of cirrhotic patients die within 1 year of demonstrating encephalopathy, making early transplant referral important.
-
Surviving transplant recipients may have persistent cognitive dysfunction in severe cases.
-
Plum and Posner's Diagnosis and Treatment of Stupor and Coma; Current Surgical Therapy 14e
Drugs to AVOID
The following are contraindicated or should be avoided:
| Drug | Reason |
|---|---|
| Thiazide diuretics | Worsen hypokalemia, precipitate encephalopathy |
| Paracentesis (large-volume without albumin replacement) | Causes circulatory dysfunction and HE |
| Morphine and opioids | Decreased hepatic clearance → prolonged CNS depression |
| Barbiturates and benzodiazepines | Same as opioids - sedation is dramatically prolonged |
| ACE inhibitors / ARBs | Worsened renal clearance in decompensated cirrhosis |
- 22nd Edition Pye's Surgical Handicraft; Rosen's Emergency Medicine
Summary Flowchart
Hepatic Coma (Grade III-IV)
↓
ABCs → Intubate if needed → Correct hypoglycemia
↓
Identify & treat precipitant (GI bleed, sepsis, electrolytes, drugs)
↓
Bowel decontamination:
→ Lactulose (oral/rectal) + Rifaximin
→ Purgation with Mg sulfate + enemas
↓
Nutrition: Zero protein → 20% IV glucose → parenteral vitamins
↓
Fluids/Electrolytes: Correct K+, Na+, acid-base
↓
Blood: Maintain Hb >10, treat coagulopathy
↓
Grade III-IV? → Screen for cerebral edema
→ Hypertonic saline (Na 145-155)
→ Mannitol 0.5-1 g/kg for raised ICP
↓
Transplant evaluation if fulminant or refractory
Prognosis Note
-
Patients with chronic cirrhosis or portacaval shunting have better recovery than those with fulminant hepatic failure.
-
Among all nontraumatic coma types, hepatic encephalopathy has the best chance for recovery (33%).
-
Cerebral edema with raised ICP (mostly fulminant failure) carries >50% mortality.
-
~50% of cirrhotic patients die within 1 year after first episode of overt encephalopathy.
-
Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 686; Adams and Victor's Principles of Neurology 12e
This is a shared conversation. Sign in to Orris to start your own chat.