analyse_media
Reading File
Finding Sources
Finding Sources
Reading File
I now have excellent source material. Let me compile the full ECG interpretation based on what was captured from the image analysis and the medical textbook content.
ECG Report Interpretation
Patient Details (from the ECG printout)
| Field | Value |
|---|---|
| ID | 20260710014433 |
| Name | Kishan Gpal |
| Age | 63 Years |
| Gender | Male |
| HR | 152 bpm |
| PR interval | 64 ms |
| QRS | 171 ms |
| QT/QTc | 307/0700 ms |
| P/QRS/T axis | 86/19/70 |
| VQ/REST | 0.453/0.324 mV |
| SN+SV1 | 0.781 mV |
| Date | 19-07-2026, 01:44:33 |
Systematic ECG Interpretation
1. Rate & Rhythm
- Heart rate: 152 bpm - this is a tachycardia
- Regular rhythm with P waves visible (PR 64 ms is very short, suggesting possible pre-excitation or measurement artifact at this rate)
2. QRS Duration - KEY FINDING
- QRS = 171 ms (normal <120 ms)
- This represents markedly widened QRS, meeting criteria for complete bundle branch block (≥120 ms)
3. Bundle Branch Block Pattern
The AI vision analysis identified the morphology as consistent with Left Bundle Branch Block (LBBB):
- V1: Wide, predominantly negative QS or rS complex
- V5/V6/lateral leads: Broad, monophasic positive R waves (no septal q waves)
- The posterior leads (V7-V9) show dominant R waves
Per Harrison's (22nd Ed, 2025):
"Left bundle branch block alters both early and later phases of ventricular depolarization... generates wide, predominantly negative (QS) complexes in lead V1 and entirely positive (R) complexes in V6."
- Harrison's Principles of Internal Medicine 22E, Bundle Branch Blocks section
Formal LBBB criteria (all met here):
- QRS ≥ 120 ms ✓ (171 ms)
- Broad monophasic R in I, V5, V6 ✓
- Absent septal q waves in I, V5, V6 ✓
- QS or rS in V1 ✓
4. Rate - Tachycardia at 152 bpm
The combination of LBBB + tachycardia at 152 bpm raises two major diagnostic possibilities:
A. Supraventricular Tachycardia (SVT) with LBBB aberrancy - e.g., sinus tachycardia or atrial flutter/tachycardia with pre-existing or rate-related LBBB
B. Ventricular Tachycardia (VT) - Wide-complex tachycardia with LBBB morphology is VT until proven otherwise in a 63-year-old male
The vision analysis itself raised this exact differential: "Is it LBBB or Ventricular Tachycardia (VT)?"
Critical Differential: SVT with LBBB vs. VT
In a 63-year-old male with wide-complex tachycardia at 152 bpm, VT must be the primary concern. Features favoring VT:
| Feature | This ECG |
|---|---|
| QRS width > 140 ms | Yes (171 ms) - strongly favors VT |
| Age > 50 + structural heart disease risk | Yes |
| LBBB-morphology VT | Very wide complex |
The Brugada algorithm and Vereckei algorithm (both referenced in Tintinalli's Emergency Medicine) are used to differentiate VT from SVT with aberrancy in wide-complex tachycardia.
Sgarbossa Criteria - MI in LBBB
If this is LBBB (pre-existing or new), the Sgarbossa criteria should be applied to exclude concurrent STEMI, as LBBB masks ST-segment changes. Per Goldman-Cecil Medicine:
"The presence of a new (or presumed new) left bundle branch block often obscures ST-segment analysis in patients with suspected acute MI."
Summary / Interpretation
| Finding | Significance |
|---|---|
| HR 152 bpm | Tachycardia - requires urgent evaluation |
| QRS 171 ms (markedly widened) | Complete bundle branch block or VT |
| LBBB morphology | LBBB pattern across precordial leads |
| 63-year-old male | High-risk for structural heart disease / VT |
Primary Interpretation: Wide-Complex Tachycardia (WCT) at 152 bpm with LBBB morphology
Differential Diagnosis (in order of urgency):
- Ventricular Tachycardia (VT) - must be excluded first; most dangerous
- SVT with pre-existing LBBB (sinus tachycardia, atrial flutter 2:1, AVNRT/AVRT with LBBB)
- SVT with rate-related (functional) LBBB aberrancy
Clinical Action Required: This ECG requires immediate clinical correlation. If the patient is hemodynamically unstable, this should be treated as VT and managed per ACLS guidelines. If stable, additional history, prior ECGs, and Brugada/Vereckei algorithm analysis are needed to differentiate VT from SVT + aberrancy. A QRS of 171 ms is beyond typical LBBB aberrancy width and increases VT probability significantly.
⚠️ This interpretation is for educational purposes. All ECG findings must be reviewed by a qualified physician in the context of the patient's clinical presentation.
Treatment options patient has fever too
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Here is a structured treatment guide based on authoritative emergency medicine textbooks.
Treatment: Wide-Complex Tachycardia + Fever in a 63-Year-Old Male
Step 1 - Immediate Hemodynamic Assessment (Do This First)
The single most important decision is: Is the patient hemodynamically stable or unstable?
| Signs of instability | Action |
|---|---|
| Hypotension (SBP < 90), altered consciousness, chest pain, acute pulmonary edema | Immediate synchronized DC cardioversion |
| HR 152 bpm but conscious, BP maintained, talking | Pharmacologic approach first |
Step 2 - Address the Fever (Critical - May Be the Cause)
Fever drives tachycardia - roughly 10 bpm increase per 1°C rise above normal. At 152 bpm, fever could be a major contributor, especially if this is sinus tachycardia with LBBB rather than true VT.
| Priority | Action |
|---|---|
| Antipyretics | Paracetamol (Acetaminophen) 500-1000 mg IV/oral; avoid NSAIDs if cardiac cause suspected |
| Identify the fever source | Blood cultures x2, CBC, CRP, procalcitonin, urine culture, chest X-ray |
| Treat sepsis if present | Broad-spectrum antibiotics empirically (e.g. piperacillin-tazobactam or ceftriaxone + metronidazole) |
| IV fluid resuscitation | If fever + hypotension = sepsis - give 30 mL/kg crystalloid bolus (cautiously if cardiac dysfunction) |
Key point from Goldman-Cecil Medicine: Underlying conditions such as sepsis and electrolyte disorders must be treated before the arrhythmia is likely to resolve on its own. Treating the fever alone may reduce the rate significantly.
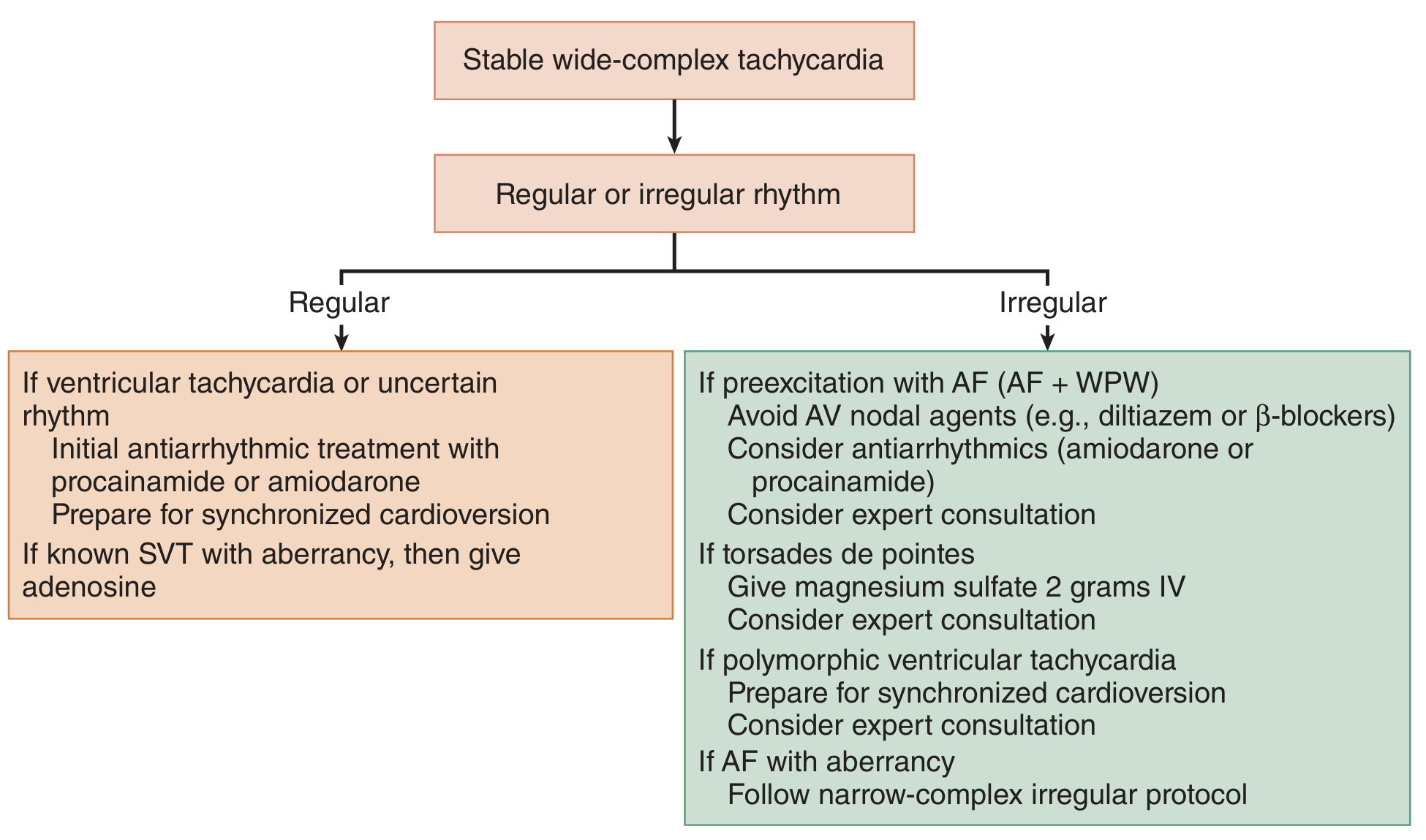
Step 3 - Arrhythmia Treatment Algorithm
(From Tintinalli's Emergency Medicine, Figure 18-3)
If UNSTABLE (hypotensive, altered, ischemic):
- Synchronized DC cardioversion immediately
- Biphasic: start at 100-200 J
- Sedate if time permits (midazolam 2-5 mg IV or fentanyl)
- Airway management ready
If STABLE - Regular WCT (most likely VT or uncertain):
| Drug | Dose | Notes |
|---|---|---|
| Procainamide (1st choice) | 20-50 mg/min IV infusion up to 17 mg/kg; maintenance 1-4 mg/min | Drug of choice for stable VT; avoid if prolonged QT or HF |
| Amiodarone (2nd choice) | 150 mg IV over 10 min, then 1 mg/min x 6 hrs, then 0.5 mg/min | Preferred if LV dysfunction present; slower conversion |
| Lidocaine (3rd choice) | 1-1.5 mg/kg IV bolus, repeat 0.5-0.75 mg/kg q5-10 min (max 3 mg/kg); maintenance 1-4 mg/min | Alternative to amiodarone; less effective for sustained VT |
"Procainamide is superior to amiodarone or lidocaine for converting patients with stable ventricular tachycardia." - Tintinalli's Emergency Medicine
"In general, wide-complex tachycardias should be managed as ventricular tachycardia until proven otherwise." - Harrison's Principles of Internal Medicine 22E
If known SVT with aberrancy (documented prior LBBB + clear SVT):
- Adenosine 6 mg rapid IV push (then 12 mg if no response) - diagnostic and therapeutic
- Avoid if pre-excitation (WPW) is suspected
Step 4 - Things to AVOID
| Drug | Reason to Avoid |
|---|---|
| Calcium channel blockers (verapamil, diltiazem) | Can cause cardiovascular collapse in VT |
| Beta-blockers (IV) | Dangerous in VT, may worsen hemodynamics |
| Digoxin | Contraindicated in WCT, dangerous in WPW |
| AV nodal agents | If pre-excitation suspected, can accelerate accessory pathway conduction |
Step 5 - Investigations to Run in Parallel
| Test | Why |
|---|---|
| 12-lead ECG comparison with old ECGs | Is LBBB new? New LBBB = treat as STEMI equivalent |
| Troponin, CK-MB | Rule out acute MI triggering VT |
| Electrolytes (K+, Mg2+, Ca2+) | Hypokalemia/hypomagnesemia provoke VT |
| Blood cultures x2 | Fever workup - sepsis-induced arrhythmia |
| Echo (urgent bedside) | Assess LV function, wall motion abnormalities |
| Thyroid function (TSH) | Hyperthyroidism causes refractory tachycardia |
| Chest X-ray | Pulmonary source for fever, cardiac silhouette |
Step 6 - After Stabilization
- Cardiology consult - mandatory for all sustained VT
- If VT confirmed: consider ICD implantation (secondary prevention) after workup
- If LBBB + heart failure: assess for cardiac resynchronization therapy (CRT/biventricular pacing)
- Electrophysiology study if etiology unclear
Summary Decision Tree
WCT 152 bpm + Fever
|
Hemodynamically stable?
/ \
NO YES
| |
Synchronized - Treat fever (paracetamol, find source)
Cardioversion - Correct electrolytes
(100-200 J biphasic) - Procainamide IV (1st line)
- Amiodarone IV (if LV dysfunction)
- If deteriorates → Cardioversion
⚠️ This is for clinical guidance only. All treatment decisions must be made by the treating physician based on real-time clinical status, local protocols, and full patient context.
This is a shared conversation. Sign in to Orris to start your own chat.