discuss hanau articulator and describe in details mechanics in gnathic system
Hanau articulator mechanics gnathic system condylar guidance Bennett movement prosthodontics
Hanau articulator H2 components five factors mechanics prosthodontics complete denture
Hanau Articulator and the Mechanics of the Gnathic System
1. Introduction
2. Classification of Articulators
| Class | Type | Examples |
|---|---|---|
| I | Simple hinge (non-adjustable) | Hinge articulator |
| II | Average value | Galetti, Dentatus ARL |
| III | Semi-adjustable | Hanau H2, Whip-Mix, Denar Mark II |
| IV | Fully adjustable | Stuart, Gnathograph, Denar D5A |
3. Historical Development
- 1920s: Rudolph L. Hanau introduced the original articulator based on his research into complete denture occlusion.
- Hanau's Quint (1926): He proposed five interrelated factors governing balanced occlusion, which became the theoretical foundation of the instrument.
- Models: Hanau 130-21, Hanau H2 (most popular), Hanau Modular Articulator System.
- The Hanau H2 uses an Arcon design (articulator condyle) where the condylar elements are in the lower member and the fossae are in the upper member - mimicking actual anatomy.
4. Hanau's Quint - The Five Factors of Balanced Occlusion
Factor 1: Condylar Guidance (Sagittal Condylar Inclination - SCI)
- The angle the condylar path makes with the horizontal reference plane (Frankfort or occlusal plane).
- In the Hanau H2: adjusted by a protractor scale on the condylar housing, typically set from 0° to 60°.
- Average value: ~33° (range 15°-60°).
- As SCI increases, the posterior teeth must be higher (more cusp height) to maintain balance.
- Obtained by: protrusive interocclusal records, then transferred to the articulator.
Factor 2: Incisal Guidance (Anterior Guidance)
- The angle the incisal guide pin traces on the incisal guide table during protrusion.
- Determined by the incisal guide table on the articulator's anterior end.
- Directly influenced by anterior tooth position and vertical/horizontal overlap (overjet and overbite).
- Average value: ~10° (can be flat, 0°, or steep).
- If incisal guidance is steep, posterior cusps must be steep to balance; if flat, cusps must be shallow.
Factor 3: Plane of Occlusion
- The orientation of the occlusal plane relative to the condylar path.
- If the plane of occlusion is raised (tilted more steeply), balance is harder to achieve.
- Measured by the occlusal plane angle relative to the axis-orbital plane.
- Adjusted by the height of the occlusal rims during try-in.
Factor 4: Compensating Curve (Anteroposterior and Lateral Curves)
- Curve of Spee (anteroposterior): The arc of curvature of the occlusal surfaces when viewed from the side, concave upward.
- Curve of Wilson (lateral/transverse): The lateral curvature of the buccal and lingual cusps from side to side.
- Together they form the Monson sphere concept (teeth ideally arranged on a sphere of 4-inch radius).
- The Hanau articulator accommodates the compensating curve by adjusting the mounting of casts.
Factor 5: Cusp Height and Inclination
- The steepness of cusp inclines on posterior teeth.
- Steeper cusps provide better balance but increase lateral forces.
- Shallower cusps (monoplane or 0°-cusp teeth) are more forgiving on residual ridges.
- The cusp angle must harmonize with SCI, incisal guidance, and the plane of occlusion.
Hanau's Formula (Condensed Quint Relationship)
Compensating Curve = (SCI + Incisal Guidance) / 8
5. Structural Components of the Hanau H2 Articulator
Upper Member (Maxillary Frame)
- Holds the maxillary cast via the upper mounting plate.
- Contains the condylar fossae/guidances (in Arcon design) - the slots that the condylar balls ride in.
- The condylar guidance inclination is set here via a calibrated scale.
- Attached to the upper frame are the lateral wall guides for Bennett movement.
Lower Member (Mandibular Frame)
- Holds the mandibular cast via the lower mounting plate.
- Contains the condylar balls (condylar elements) in Arcon design.
- The condylar balls sit in the fossae of the upper member.
Condylar Mechanism
- Located at the posterior aspect of each side.
- The condylar housing contains a graduated protractor to set SCI (0°-60°).
- The condylar path is a straight ramp (not curved) - a limitation of semi-adjustable articulators.
- The intercondylar distance is fixed at ~110 mm (average value) in standard Hanau H2; some models offer three intercondylar settings (narrow, medium, wide).
Incisal Guide Pin and Table
- Located at the anterior aspect between the two members.
- The incisal guide pin extends downward from the upper member and rests on the incisal guide table below.
- The incisal guide table can be angled (adjustable) or flat (average value, typically 10°).
- A custom incisal guide table can be fabricated chairside in acrylic.
- Controls the anterior determinant of occlusion.
Mounting Plates
- Upper and lower mounting plates accept the dental casts with plaster/stone.
- The facebow record is used to mount the maxillary cast so it is spatially oriented relative to the hinge axis - this is transferred via the earbow or kinematic facebow.
Hinge Axis
- The transverse hinge axis (terminal hinge axis / centric relation axis) is the reference axis around which pure rotation of the mandible occurs.
- The Hanau H2 uses an arbitrary hinge axis (pre-auricular point, 13 mm anterior to the tragus of the ear) rather than a true kinematic axis.
- All centric relation records are made with the condyles in their most superior, anterior, and medial position in the glenoid fossa.
Bennett Movement Control
- The lateral wall of the condylar housing provides resistance to mediotrusive (non-working) condyle movement.
- The Bennett angle (also called the Fischer angle) is the angle the working condyle moves laterally, typically 0°-30°, average 15°.
- Some Hanau models have adjustable Bennett angle settings; others use a fixed angle.
- The immediate side shift (ISS) and progressive side shift can be partially simulated.
6. The Gnathic System - Mechanics in Detail
6a. The Temporomandibular Joint (TMJ)
- A ginglymoarthrodial joint - combines rotation (ginglymoid) and translation (arthrodial).
- The condyle is convex, the articular eminence (posterior slope of the articular tubercle) is concave, and the disc acts as a movable third unit.
- The disc divides the joint into:
- Superior compartment: Translation (sliding movements - protrusion, lateral excursion).
- Inferior compartment: Rotation (hinge movements - mouth opening).
- First phase (0-25 mm opening): Pure rotation of the condyle in the inferior compartment. The hinge axis is at the condylar heads.
- Second phase (25+ mm): Translation begins - the condyle and disc together slide forward and downward along the articular eminence.
6b. Mandibular Movements
- The most retruded, reproducible position of the condyles - superior and anterior in the glenoid fossa, against the posterior slopes of the articular eminences.
- A purely ligamentous position - reproducible and independent of tooth contact.
- This is the reference position used to mount casts on the Hanau articulator.
- The position of maximum tooth contact regardless of condylar position.
- In ideal occlusion, CO = CR (they coincide).
- The CR-CO discrepancy (also called "long centric") is typically 0-1 mm anteriorly and is accommodated in prosthetic rehabilitation.
- Both condyles translate forward and downward along the articular eminences.
- Guided by the disclusion of posterior teeth by the anterior teeth (anterior guidance).
- The protrusive condylar path angle = condylar inclination = SCI (~33°).
- The protrusive interocclusal record (with a wax wafer) is used to program the SCI on the Hanau articulator.
- Working side (ipsilateral): The condyle on the side toward which the mandible moves performs a rotation + lateral shift - called the Bennett movement or lateral translation.
- Non-working side (balancing/mediotrusive side): The contralateral condyle moves anteriorly, inferiorly, and medially - tracing the orbiting condyle path.
- Named after Norman Godfrey Bennett (1906).
- The working condyle moves laterally outward.
- Has two components:
- Immediate side shift (ISS): An initial, immediate bodily lateral translation of the entire mandible at the onset of lateral movement (0-3 mm).
- Progressive side shift: The gradual lateral displacement that continues throughout the lateral excursion.
- Bennett angle: The angle between the sagittal plane and the path of the orbiting condyle in the horizontal plane (~15°, range 0°-30°).
- Programmed on the Hanau articulator via the lateral condylar housing adjustments.
- Described by Ulf Posselt (1952) as the three-dimensional envelope of all possible mandibular movements.
- In the sagittal plane:
- Superior border: Tooth contact positions from CR through CO to protrusion.
- Posterior border: Hinge movements from CR (closure) to maximum opening.
- Anterior border: Maximum protrusion.
- Inferior border: Maximum opening arc.
- The articulator can only approximate a portion of this envelope.
7. Occlusal Theories and Their Relationship to the Hanau System
Balanced Occlusion (Bilateral Balance)
- The goal of complete denture occlusion.
- All posterior teeth contact simultaneously during all excursive movements (protrusion, lateral excursion) to stabilize the denture bases.
- The Hanau articulator was specifically designed to help achieve this.
- Governed by Hanau's Quint.
Mutually Protected Occlusion (Canine-Protected Occlusion)
- In natural dentition and fixed prosthetics: canines bear lateral loads, disoccluding posterior teeth in lateral excursion.
- Not applicable to complete dentures (canines cannot protect a denture from tipping).
Group Function Occlusion
- Multiple posterior teeth contact on the working side during lateral movements.
- Used in certain fixed prosthodontic cases and implant-supported prostheses.
8. Facebow Transfer and Mounting Procedure
- Earbow (arbitrary axis): The Hanau earbow (also called the Spring-bow or Springbow) uses ear canal rods positioned ~13 mm anterior to the tragus to locate the approximate hinge axis.
- The orbital pointer establishes the third reference point (infraorbital notch), defining the axis-orbital plane (equivalent to the Frankfort plane).
- The occlusal rim is attached to the facebow, which is then transferred to the upper member of the Hanau articulator.
- This ensures the maxillary cast is positioned in the same spatial relationship to the hinge axis as the maxilla is to the TMJ.
- Without a facebow, the cast is arbitrarily mounted - leading to errors in tooth position, occlusal plane, and cusp contact during excursions.
9. Programming the Hanau H2 - Step by Step
| Step | Procedure | Record Used |
|---|---|---|
| 1 | Mount maxillary cast | Facebow transfer |
| 2 | Mount mandibular cast | Centric relation interocclusal record |
| 3 | Set SCI (condylar inclination) | Protrusive interocclusal record (5-6 mm protrusion) |
| 4 | Set Bennett angle | Lateral interocclusal record |
| 5 | Adjust incisal guide table | Custom acrylic or set average 10° |
| 6 | Check compensating curves | Verify Hanau's formula |
10. Limitations of the Hanau H2
| Limitation | Clinical Impact |
|---|---|
| Arbitrary hinge axis | Error up to 0.5 mm - acceptable for dentures, not ideal for complex fixed cases |
| Straight condylar path (not curved) | The actual condylar path is curved (Bennett curves); the straight ramp introduces minor inaccuracy |
| Fixed intercondylar distance (110 mm average) | Patients with wide or narrow cranial base introduce error |
| Cannot reproduce ISS precisely | Immediate side shift is only approximately simulated |
| No curved protrusive path | Path simulated as linear, not the true arc |
| No envelope of motion beyond set points | Cannot replicate all of Posselt's envelope |
11. Comparison with Other Articulators
| Feature | Hanau H2 | Whip-Mix | Stuart (Fully Adjustable) |
|---|---|---|---|
| Type | Semi-adjustable (Arcon) | Semi-adjustable (Arcon) | Fully adjustable |
| Hinge axis | Arbitrary | Arbitrary | Kinematic |
| Condylar path | Straight | Straight | Curved |
| Bennett movement | Adjustable | Adjustable | Fully customized |
| Intercondylar distance | Fixed | Three settings | Fully adjustable |
| Ideal use | Complete dentures, FPD | Same | Complex occlusal rehab |
12. Clinical Significance Summary
- The Hanau articulator replicates the five mechanical factors (Quint) that govern occlusal balance.
- It translates biological jaw movements (condylar guidance, Bennett movement, hinge rotation) into mechanical analogs (condylar housing, lateral walls, hinge axis).
- Proper programming with accurate interocclusal records ensures that restorations fabricated on the articulator will fit and function harmoniously when placed in the patient.
- The gnathic system - the TMJ, muscles, and teeth - operates through a precisely coordinated neuromuscular program; the articulator approximates only the skeletal/mechanical determinants of this system, not the neuromuscular component.
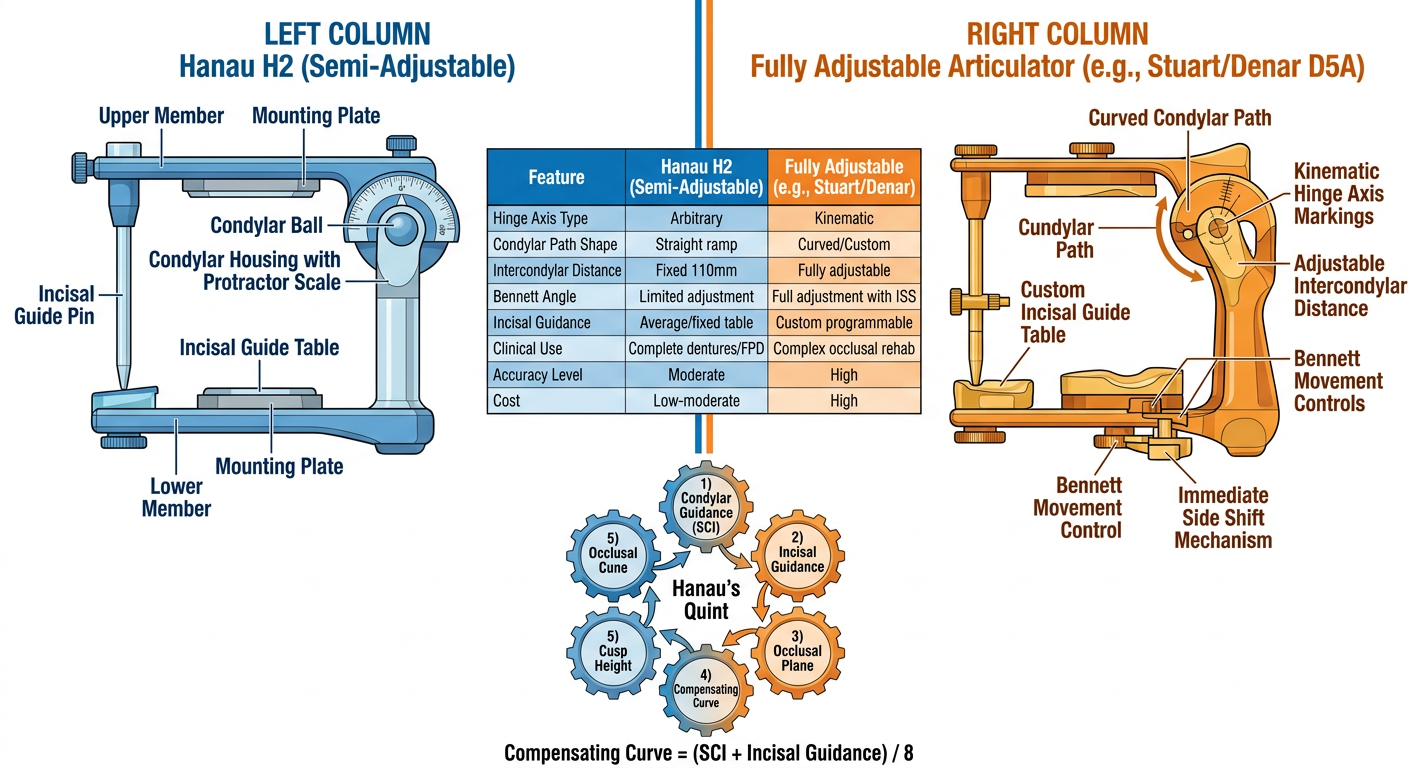
Create a detailed diagram comparing Hanau H2 vs fully adjustable articulators
A detailed professional dental/prosthodontics educational diagram comparing Hanau H2 Semi-Adjustable Articulator vs Fully Adjustable Articulator (Stuart/Denar). The diagram is divided into two main columns with a clear dividing line. LEFT COLUMN - "Hanau H2 (Semi-Adjustable)" with a schematic side-view drawing of the articulator showing: upper member, lower member, condylar housing with protractor scale, incisal guide pin and table, mounting plates, condylar ball. Label all parts clearly. RIGHT COLUMN - "Fully Adjustable Articulator (e.g., Stuart/Denar D5A)" with a schematic drawing showing: curved condylar path, kinematic hinge axis markings, adjustable intercondylar distance, custom incisal guide table, Bennett movement controls, immediate side shift mechanism. MIDDLE SECTION - A comparison table with rows for: Hinge Axis Type (Arbitrary vs Kinematic), Condylar Path Shape (Straight ramp vs Curved/Custom), Intercondylar Distance (Fixed 110mm vs Fully adjustable), Bennett Angle (Limited adjustment vs Full adjustment with ISS), Incisal Guidance (Average/fixed table vs Custom programmable), Clinical Use (Complete dentures/FPD vs Complex occlusal rehab), Accuracy Level (Moderate vs High), Cost (Low-moderate vs High). BOTTOM SECTION - A visual diagram showing "Hanau's Quint" as five interconnected gears or circles labeled: 1) Condylar Guidance (SCI), 2) Incisal Guidance, 3) Occlusal Plane, 4) Compensating Curve, 5) Cusp Height - with arrows showing their interdependence and the formula: Compensating Curve = (SCI + Incisal Guidance) / 8. Color scheme: Blue tones for Hanau H2, Orange/amber tones for Fully Adjustable, white background, clean medical textbook illustration style with clear bold labels and annotations.
- Arcon design with condylar balls in the lower member
- Straight condylar path ramp (0°-60° range, ~33° average)
- Arbitrary hinge axis (~13 mm anterior to tragus)
- Fixed intercondylar distance (~110 mm)
- Adjustable incisal guide table (average 10°)
- Curved, customizable condylar path replicating the actual Bennett curve
- Kinematic hinge axis (true terminal hinge axis located by pantograph or axiograph)
- Fully adjustable intercondylar distance
- Precise immediate side shift (ISS) and progressive Bennett movement programming
- Custom incisal guide table fabricated from patient records
Compensating Curve = (SCI + Incisal Guidance) / 8
Make a presentation on Posselt's envelope of motion and its clinical implications
A detailed anatomical/biomechanics diagram of Posselt's Envelope of Motion (Posselt's envelope of movement) for dental/prosthodontics education. Show TWO views side by side: LEFT - SAGITTAL VIEW (viewed from the side): A tear-drop or leaf-shaped envelope outline with clearly labeled border movements: - Top-left point: "Centric Relation (CR)" with a small condyle diagram - Slightly anterior to CR: "Centric Occlusion (CO) / MIP" with a small arrow showing CR-CO slide (1mm) - Bottom point: "Maximum Opening" (~50mm) - Right border: "Maximum Protrusion" (8-10mm forward) - Posterior superior border: "Terminal Hinge Arc" (pure rotation, dotted arc line) - Anterior inferior border: "Protrusive path" - Label the functional range in the center as a shaded zone: "Functional Chewing Range" - Show arrows indicating direction of movement along each border - Add measurements: Opening ~50mm, Protrusion ~8-10mm, CR-CO ~1mm - Label "SUPERIOR" at top, "INFERIOR" at bottom, "ANTERIOR" right, "POSTERIOR" left RIGHT - FRONTAL/CORONAL VIEW: A diamond/rhombus shaped envelope showing: - Center: "Centric Occlusion" - Left: "Maximum Left Lateral Excursion" (~12mm) - Right: "Maximum Right Lateral Excursion" (~12mm) - Bottom: "Maximum Opening" - Label Bennett movement arcs on each side - Label "Working Side" and "Non-working Side" Clean white background, medical textbook illustration style, blue and teal color scheme, bold labels, anatomical precision. Include a title at top: "Posselt's Envelope of Motion (1952)"
A dental prosthodontics educational diagram showing the clinical implications of Posselt's Envelope of Motion organized as a visual infographic. Six labeled sections arranged around a central "Clinical Significance" hub: 1. "Complete Denture Construction" - icon of denture, text: "Centric relation registration, occlusal balance within functional range" 2. "TMD Diagnosis" - icon of jaw joint, text: "Restricted envelope = limited opening, deviation, muscle splinting" 3. "Occlusal Rehabilitation" - icon of teeth, text: "Restorations must not exceed border movements, freedom in centric" 4. "Implant Dentistry" - icon of implant, text: "No proprioception - wider centric stop needed, flat cusp angles" 5. "Orthodontic Treatment" - icon of braces, text: "Tooth movement changes envelope shape - monitor CR-CO discrepancy" 6. "Articulator Programming" - icon of articulator, text: "Envelope guides condylar inclination, incisal guidance settings" Central hub with connecting arrows, deep navy blue background with white and gold text, professional medical infographic style, clear readable labels, icons are simple line-art style.
Medical dental education diagram showing Border Movements of the mandible - three-dimensional representation. Show a 3D perspective view of the mandible with labeled movement paths: Top section: "SUPERIOR BORDER MOVEMENTS" - show teeth occlusal contact positions as a curved line from CR (centric relation) back through CO (centric occlusion) to maximum protrusion, with lateral excursions shown as arcs on left and right Middle section: Show the mandible silhouette with movement paths as colored arrows: - Blue arrows: Sagittal border movements (hinge + protrusion) - Green arrows: Lateral border movements (left and right Bennett movements) - Red arrows: Opening/closing movements Labeled key positions as numbered dots: 1. Centric Relation (CR) 2. Centric Occlusion (CO) / Maximum Intercuspation 3. Maximum Opening (~50mm) 4. Maximum Protrusion (8-10mm) 5. Maximum Left Lateral (12mm) 6. Maximum Right Lateral (12mm) Bottom: Small table showing: "Functional zone = 1-3mm opening, within 1-2mm lateral" shaded green as "Safe Restoration Zone" White background, clean anatomical illustration, color-coded arrows, professional dental textbook quality
mkdir -p /home/daytona/workspace/posselt-presentation
Failed to create session: unauthorized: authentication failed: Bearer token is invalid
We encountered an error while processing your request. Please try again or reach out to us for help.
Make a presentation on Posselt's envelope of motion and its clinical implications
Detailed anatomical diagram of Posselt's Envelope of Motion for dental education. Show two diagrams side by side on a white background. LEFT DIAGRAM - Sagittal (side) view: A closed teardrop/leaf-shaped border outline with these labeled positions: - Top right: small dot labeled "CR - Centric Relation" with notation "condyles retruded, superior" - Just anterior to CR: dot labeled "CO / MIP" with "1mm slide" arrow between CR and CO - Far right middle: "Maximum Protrusion 8-10mm" - Bottom: "Maximum Opening ~50mm" - The posterior-superior curved arc labeled "Terminal Hinge Arc (pure rotation)" - The anterior border labeled "Protrusive-opening border" - Center shaded blue oval area labeled "Functional Chewing Zone (2-5mm opening)" - Axes labeled: SUPERIOR/INFERIOR (vertical), ANTERIOR/POSTERIOR (horizontal) RIGHT DIAGRAM - Frontal (coronal) view: A diamond/rhombus shape with: - Top: "CO - Centric Occlusion" - Bottom: "Maximum Opening 50mm" - Left: "Left Lateral 10-12mm" - Right: "Right Lateral 10-12mm" - Small curved paths on left and right showing "Bennett movement arcs" - Center shaded area: "Functional Zone" Title at top: "POSSELT'S ENVELOPE OF MOTION (1952)" Subtitle: "Three-Dimensional Limit of Mandibular Movement" Color: navy blue envelope outline, teal shading for functional zones, clean medical illustration style, white background
Professional dental/prosthodontics infographic showing clinical implications of Posselt's Envelope of Motion. Navy blue background. Six rectangular cards arranged in 2 rows of 3, each card with a white rounded rectangle on dark navy: Card 1 - "Complete Dentures": Simple line-art denture icon. Text: "CR used as reference position. Bilateral balance within functional zone essential for stability." Card 2 - "TMD Assessment": Jaw joint icon. Text: "Reduced envelope = pathology. Deviation on opening indicates disc displacement or muscle restriction." Card 3 - "Occlusal Rehabilitation": Tooth icon. Text: "Restorations must not exceed border movements. CR-CO discrepancy must be identified before treatment." Card 4 - "Implant Prosthetics": Implant screw icon. Text: "No periodontal ligament proprioception. Flat cusps and wider centric stop required." Card 5 - "Fixed Prosthodontics": Crown/bridge icon. Text: "Freedom in centric (long centric) must be built in. Avoid interferences outside functional zone." Card 6 - "Articulator Programming": Articulator device icon. Text: "Envelope guides condylar inclination (SCI ~33deg) and incisal guidance settings (~10deg)." Gold/amber accent color for card headers, white text on navy background, clean modern medical infographic design, professional typography. Title at top in gold: "CLINICAL SIGNIFICANCE OF POSSELT'S ENVELOPE"
Dental education diagram showing the Key Positions within Posselt's Envelope of Motion. Clean white background, medical textbook style. Show a large sagittal envelope outline (leaf/teardrop shape) with 6 numbered positions clearly marked as colored dots with text callouts: Position 1 (Red dot, top-right): "CENTRIC RELATION (CR)" - "Most superior, anterior position of condyles. Reproducible. Ligament-determined. Reference for prosthodontics." Position 2 (Orange dot, just left of CR): "CENTRIC OCCLUSION (CO) / MIP" - "Maximum tooth intercuspation. Muscle-determined. 0-1mm anterior to CR. Goal: CR=CO in ideal occlusion." Position 3 (Blue dot, right-middle): "MAXIMUM PROTRUSION" - "8-10mm anterior. Both condyles fully translated forward. Guided by incisal edges." Position 4 (Green dot, bottom): "MAXIMUM OPENING" - "~50mm. Combined rotation (~25mm) and translation (~25mm). Measured between upper and lower incisors." Position 5 (Purple dot, upper arc): "RETRUDED CONTACT POSITION (RCP)" - "First tooth contact in terminal hinge arc. Often posterior to CO." Position 6 (Teal, center shaded zone): "FUNCTIONAL CHEWING RANGE" - "1-5mm opening, small lateral excursions. Daily mastication stays within this zone." Show CR-CO slide as a horizontal arrow between positions 1 and 2 labeled "1mm (Long Centric)" Show terminal hinge arc as a dotted curve from CR downward labeled "Pure rotation ~25mm" Show functional zone as a shaded teal ellipse Title: "BORDER POSITIONS WITHIN POSSELT'S ENVELOPE" Professional dental illustration, clear annotations, arrows pointing to each position
mkdir -p /home/daytona/workspace/posselt-presentation && ls /home/daytona/workspace/posselt-presentation
~/posselt-presentation/build.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// ── Color Palette ──────────────────────────────────────────────────────────
const NAVY = "0D1B3E"; // dominant dark bg
const TEAL = "0A8F8F"; // accent / highlights
const GOLD = "D4A82A"; // secondary accent
const WHITE = "FFFFFF";
const LGRAY = "EAF0F6"; // light card bg
const MIDGRAY = "8CA0B8"; // subdued text
const ORANGE = "E8622A"; // call-out accent
const pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.3" × 7.5"
pres.author = "Orris AI";
pres.title = "Posselt's Envelope of Motion";
pres.subject = "Prosthodontics / Dental Occlusion";
// ── Fetch remote images as base64 ─────────────────────────────────────────
const IMG_ENVELOPE = "https://cdn.orris.care/image-gen/af009503bd7241a897b42af7054e868a.png";
const IMG_CLINICAL = "https://cdn.orris.care/image-gen/7a25d2fe62b74b6ea9f134ed406c7ccc.png";
const IMG_POSITIONS = "https://cdn.orris.care/image-gen/5afb03ba83a14f2590d661f0a3864b2c.png";
console.log("Fetching images…");
const imgs = JSON.parse(
execSync(
`node /home/daytona/skills/shared/scripts/fetch_images.js "${IMG_ENVELOPE}" "${IMG_CLINICAL}" "${IMG_POSITIONS}"`
).toString()
);
const [imgEnvelope, imgClinical, imgPositions] = imgs;
console.log("Images fetched:", imgs.map(i => i.error || "OK"));
// ══════════════════════════════════════════════════════════════════════════
// Helper: dark full-bleed background
function darkBg(slide) {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5,
fill: { color: NAVY }, line: { color: NAVY }
});
}
// Helper: accent top bar
function topBar(slide, color = TEAL) {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 0.08,
fill: { color }, line: { color }
});
}
// Helper: section label chip
function chip(slide, text, x, y, bg = TEAL) {
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w: 2.2, h: 0.32,
fill: { color: bg }, line: { color: bg }, rectRadius: 0.06
});
slide.addText(text.toUpperCase(), {
x, y, w: 2.2, h: 0.32,
fontSize: 9, bold: true, color: WHITE,
align: "center", valign: "middle", margin: 0
});
}
// Helper: slide heading on white/light slide
function lightHeading(slide, title, subtitle = "") {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 1.05,
fill: { color: NAVY }, line: { color: NAVY }
});
topBar(slide, GOLD);
slide.addText(title, {
x: 0.5, y: 0.12, w: 12.3, h: 0.6,
fontSize: 26, bold: true, color: WHITE, fontFace: "Calibri",
align: "left", valign: "middle", margin: 0
});
if (subtitle) {
slide.addText(subtitle, {
x: 0.5, y: 0.7, w: 12.3, h: 0.3,
fontSize: 13, color: GOLD, fontFace: "Calibri", italic: true,
align: "left", valign: "middle", margin: 0
});
}
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 1 — Title Slide
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkBg(s);
topBar(s, GOLD);
// Left vertical accent bar
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0.08, w: 0.06, h: 7.42,
fill: { color: TEAL }, line: { color: TEAL }
});
// Decorative large circle (background element)
s.addShape(pres.shapes.OVAL, {
x: 7.8, y: -1.2, w: 7, h: 7,
fill: { color: "0F2555", transparency: 30 }, line: { color: "0F2555", transparency: 30 }
});
s.addShape(pres.shapes.OVAL, {
x: 8.5, y: -0.5, w: 5.5, h: 5.5,
fill: { color: "0A3070", transparency: 20 }, line: { color: "0A3070", transparency: 20 }
});
// Topic chip
chip(s, "Prosthodontics", 0.6, 1.4, TEAL);
// Main title
s.addText("Posselt's Envelope", {
x: 0.6, y: 1.9, w: 9, h: 1.0,
fontSize: 48, bold: true, color: WHITE, fontFace: "Calibri",
align: "left", valign: "middle", margin: 0
});
s.addText("of Motion", {
x: 0.6, y: 2.85, w: 9, h: 0.85,
fontSize: 48, bold: true, color: GOLD, fontFace: "Calibri",
align: "left", valign: "middle", margin: 0
});
// Subtitle
s.addText("Three-Dimensional Limits of Mandibular Movement\nand Clinical Implications in Prosthodontics", {
x: 0.6, y: 3.75, w: 8.5, h: 0.85,
fontSize: 16, color: MIDGRAY, fontFace: "Calibri", italic: true,
align: "left", valign: "top", margin: 0
});
// Bottom metadata
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 6.85, w: 13.3, h: 0.65,
fill: { color: "091630" }, line: { color: "091630" }
});
s.addText("Ulf Posselt | 1952 | Department of Prosthodontics | Dental Occlusion & Gnathology", {
x: 0.6, y: 6.88, w: 12, h: 0.55,
fontSize: 11, color: MIDGRAY, fontFace: "Calibri",
align: "left", valign: "middle", margin: 0
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 2 — What is Posselt's Envelope?
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5,
fill: { color: LGRAY }, line: { color: LGRAY }
});
lightHeading(s, "What is Posselt's Envelope of Motion?", "Definition & Historical Context");
// Left text panel
const boxW = 5.8;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.4, y: 1.2, w: boxW, h: 5.9,
fill: { color: WHITE }, line: { color: "D0DCE8" }, rectRadius: 0.12,
shadow: { type: "outer", color: "000000", blur: 8, offset: 2, angle: 135, opacity: 0.1 }
});
s.addText([
{ text: "Definition", options: { bold: true, color: NAVY, fontSize: 15, breakLine: true } },
{ text: "\n", options: { fontSize: 6, breakLine: true } },
{ text: "The three-dimensional space within which ALL mandibular movements occur. It represents the outer boundary — or \"border movements\" — of the jaw.", options: { color: "333333", fontSize: 12.5, breakLine: true } },
{ text: "\n", options: { fontSize: 8, breakLine: true } },
{ text: "Historical Background", options: { bold: true, color: NAVY, fontSize: 15, breakLine: true } },
{ text: "\n", options: { fontSize: 6, breakLine: true } },
{ text: "Described by Swedish prosthodontist Ulf Posselt in 1952, based on stereoscopic recordings of incisor point movements.", options: { color: "333333", fontSize: 12.5, breakLine: true } },
{ text: "\n", options: { fontSize: 8, breakLine: true } },
{ text: "Key Principle", options: { bold: true, color: NAVY, fontSize: 15, breakLine: true } },
{ text: "\n", options: { fontSize: 6, breakLine: true } },
{ text: "All voluntary jaw movements lie INSIDE the envelope. The borders are determined by the TMJ ligaments, articular surfaces, and teeth — not by muscles alone.", options: { color: "333333", fontSize: 12.5, breakLine: true } },
{ text: "\n", options: { fontSize: 8, breakLine: true } },
{ text: "Clinical Relevance", options: { bold: true, color: NAVY, fontSize: 15, breakLine: true } },
{ text: "\n", options: { fontSize: 6, breakLine: true } },
{ text: "Any restoration or prosthesis must be designed to function harmoniously within this envelope — violations cause occlusal interference, TMD, or prosthetic failure.", options: { color: "333333", fontSize: 12.5, breakLine: true } },
], { x: 0.7, y: 1.3, w: 5.2, h: 5.7, valign: "top", margin: 8 });
// Right: quote card + stats
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 6.8, y: 1.2, w: 6.1, h: 2.2,
fill: { color: NAVY }, line: { color: NAVY }, rectRadius: 0.12
});
s.addText([
{ text: "\"", options: { fontSize: 40, color: GOLD, bold: true } },
{ text: "The movement of the mandible is limited in every direction by a three-dimensional envelope that can be reproducibly recorded.\"\n", options: { fontSize: 13.5, color: WHITE, italic: true } },
{ text: "— Ulf Posselt, 1952", options: { fontSize: 11, color: GOLD } }
], { x: 7.0, y: 1.3, w: 5.7, h: 2.0, valign: "top", margin: 6 });
// Three stat cards
const stats = [
{ val: "1952", label: "Year Described" },
{ val: "~50mm", label: "Max Opening" },
{ val: "3D", label: "Spatial Model" },
];
stats.forEach((st, i) => {
const sx = 6.8 + i * 2.05;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: sx, y: 3.7, w: 1.9, h: 1.55,
fill: { color: WHITE }, line: { color: TEAL, pt: 2 }, rectRadius: 0.1
});
s.addText(st.val, {
x: sx, y: 3.75, w: 1.9, h: 0.85,
fontSize: 28, bold: true, color: TEAL, align: "center", valign: "middle", margin: 0
});
s.addText(st.label, {
x: sx, y: 4.55, w: 1.9, h: 0.55,
fontSize: 10.5, color: NAVY, align: "center", valign: "top", margin: 2
});
});
// Two points at bottom right
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 6.8, y: 5.55, w: 6.1, h: 1.52,
fill: { color: "EEF4FB" }, line: { color: "D0DCE8" }, rectRadius: 0.1
});
s.addText([
{ text: "▸ ", options: { color: TEAL, bold: true } },
{ text: "Tooth contacts occur only along the superior border — NOT within the envelope body.\n", options: { color: "333333", fontSize: 12 } },
{ text: "▸ ", options: { color: TEAL, bold: true } },
{ text: "Functional chewing movements use only a small fraction of the total envelope.", options: { color: "333333", fontSize: 12 } }
], { x: 7.0, y: 5.65, w: 5.7, h: 1.3, valign: "top", margin: 4 });
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 3 — The Envelope Diagram (Sagittal + Frontal)
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5,
fill: { color: LGRAY }, line: { color: LGRAY }
});
lightHeading(s, "The Envelope — Sagittal & Frontal Views", "Border movements in two planes");
if (imgEnvelope && !imgEnvelope.error) {
s.addImage({ data: imgEnvelope.base64, x: 0.3, y: 1.1, w: 12.7, h: 6.1 });
} else {
s.addText("Envelope diagram unavailable", { x: 1, y: 3, w: 11, h: 1, fontSize: 16, color: "999999", align: "center" });
}
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 4 — Key Border Positions
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5,
fill: { color: LGRAY }, line: { color: LGRAY }
});
lightHeading(s, "Key Border Positions Within the Envelope", "Six critical mandibular reference points");
if (imgPositions && !imgPositions.error) {
s.addImage({ data: imgPositions.base64, x: 0.3, y: 1.05, w: 12.7, h: 6.2 });
} else {
s.addText("Positions diagram unavailable", { x: 1, y: 3, w: 11, h: 1, fontSize: 16, color: "999999", align: "center" });
}
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 5 — Border Movements Explained
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5,
fill: { color: LGRAY }, line: { color: LGRAY }
});
lightHeading(s, "Border Movements in Detail", "Sagittal plane — four borders of the envelope");
const borders = [
{
title: "1. Posterior Superior Border",
color: TEAL,
body: "The Terminal Hinge Arc: pure rotation of condyles in centric relation. From CR closure through ~25mm of mouth opening. Reproducible — used as the reference in prosthodontics. Represents \"retruded contact position\" at tooth contact.",
},
{
title: "2. Superior Occlusal Border",
color: GOLD,
body: "From RCP (retruded contact) sliding forward to centric occlusion (CO/MIP), then forward to maximum protrusion (~8-10mm). Tooth contacts define this border. The CR-CO slide is 0-1mm anteriorly — called \"long centric\" or freedom in centric.",
},
{
title: "3. Anterior-Inferior Border",
color: ORANGE,
body: "Maximum protrusion combined with increasing mouth opening. The mandible is at its most forward position throughout this movement. The path curves downward and backward to maximum opening.",
},
{
title: "4. Posterior-Inferior Border",
color: "7B5EA7",
body: "Maximum opening (~50mm) back to the most retruded open position. Represents the inferior and posterior limit of movement. Condyles are translated maximally forward at peak opening, then retruded back toward CR.",
},
];
borders.forEach((b, i) => {
const col = i < 2 ? 0 : 1;
const row = i % 2;
const x = 0.4 + col * 6.5;
const y = 1.25 + row * 2.85;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w: 6.1, h: 2.65,
fill: { color: WHITE }, line: { color: b.color, pt: 2 }, rectRadius: 0.1,
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.08 }
});
// Color accent left bar
s.addShape(pres.shapes.RECTANGLE, {
x, y: y + 0.1, w: 0.07, h: 2.45,
fill: { color: b.color }, line: { color: b.color }
});
s.addText(b.title, {
x: x + 0.2, y: y + 0.12, w: 5.7, h: 0.45,
fontSize: 13.5, bold: true, color: NAVY, fontFace: "Calibri",
align: "left", valign: "middle", margin: 0
});
s.addText(b.body, {
x: x + 0.2, y: y + 0.6, w: 5.7, h: 1.9,
fontSize: 12, color: "333333", fontFace: "Calibri",
align: "left", valign: "top", margin: 4
});
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 6 — CR vs CO: The Critical Discrepancy
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkBg(s);
topBar(s, GOLD);
s.addText("CR vs CO: The Critical Discrepancy", {
x: 0.6, y: 0.18, w: 12, h: 0.65,
fontSize: 26, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
s.addText("Understanding the CR-CO slide and its clinical importance", {
x: 0.6, y: 0.8, w: 12, h: 0.28,
fontSize: 13, color: GOLD, italic: true, fontFace: "Calibri", margin: 0
});
// Two main boxes
const items = [
{
label: "CENTRIC RELATION (CR)",
color: TEAL,
pts: [
"Most superior, anterior position of both condyles in glenoid fossa",
"Ligament-determined — independent of tooth contacts",
"Reproducible — used as reference for complete dentures and occlusal rehab",
"Also called: Retruded contact position (RCP) at initial tooth contact",
"Recorded by: bimanual manipulation, chin-point guidance, leaf gauge",
]
},
{
label: "CENTRIC OCCLUSION (CO) / MIP",
color: GOLD,
pts: [
"Position of maximum tooth intercuspation — muscle-determined",
"Normal: 0-1mm ANTERIOR and slightly superior to CR",
"Does NOT coincide with CR in ~90% of natural dentitions",
"Goal of occlusal rehabilitation: bring CR = CO (or allow freedom in centric)",
"Large CR-CO discrepancy = potential TMD risk; requires treatment planning",
]
}
];
items.forEach((item, i) => {
const x = 0.4 + i * 6.5;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y: 1.25, w: 6.1, h: 4.85,
fill: { color: "0F2555" }, line: { color: item.color, pt: 2 }, rectRadius: 0.12
});
s.addShape(pres.shapes.RECTANGLE, {
x, y: 1.25, w: 6.1, h: 0.5,
fill: { color: item.color }, line: { color: item.color }
});
s.addText(item.label, {
x: x + 0.15, y: 1.27, w: 5.8, h: 0.45,
fontSize: 13, bold: true, color: WHITE, fontFace: "Calibri", margin: 0,
align: "left", valign: "middle"
});
const bullets = item.pts.map((p, j) => ({
text: p,
options: { bullet: { type: "bullet" }, color: j === 0 ? WHITE : "B0C8E0", fontSize: 12.5, breakLine: j < item.pts.length - 1 }
}));
s.addText(bullets, {
x: x + 0.2, y: 1.85, w: 5.7, h: 4.1,
fontFace: "Calibri", valign: "top", margin: 4
});
});
// Bottom banner
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.4, y: 6.25, w: 12.5, h: 0.95,
fill: { color: GOLD, transparency: 10 }, line: { color: GOLD }, rectRadius: 0.08
});
s.addText([
{ text: "Clinical Rule: ", options: { bold: true, color: NAVY, fontSize: 13.5 } },
{ text: "In complete denture construction, ALWAYS use CR as the reference — CO cannot be reproduced without natural teeth. In fixed prosthodontics, identify CR-CO discrepancy BEFORE initiating treatment.", options: { color: NAVY, fontSize: 13 } }
], { x: 0.65, y: 6.3, w: 12, h: 0.82, valign: "middle", margin: 4 });
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 7 — Lateral Envelope & Bennett Movement
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5,
fill: { color: LGRAY }, line: { color: LGRAY }
});
lightHeading(s, "Lateral Envelope & Bennett Movement", "Frontal plane and working/non-working condyle paths");
// Left: Bennett explanation
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.4, y: 1.2, w: 5.6, h: 5.9,
fill: { color: WHITE }, line: { color: "D0DCE8" }, rectRadius: 0.12,
shadow: { type: "outer", color: "000000", blur: 8, offset: 2, angle: 135, opacity: 0.08 }
});
s.addText([
{ text: "Bennett Movement\n", options: { bold: true, color: NAVY, fontSize: 15, breakLine: true } },
{ text: "Named after Norman G. Bennett (1906). The bodily lateral shift of the mandible during lateral excursion.\n\n", options: { color: "444444", fontSize: 12.5 } },
{ text: "Components:\n", options: { bold: true, color: TEAL, fontSize: 13 } },
{ text: "• Immediate Side Shift (ISS): 0-3mm initial lateral translation of entire mandible at onset of excursion\n", options: { color: "444444", fontSize: 12 } },
{ text: "• Progressive Side Shift: gradual lateral displacement continuing throughout excursion\n\n", options: { color: "444444", fontSize: 12 } },
{ text: "Working Side Condyle:\n", options: { bold: true, color: TEAL, fontSize: 13 } },
{ text: "Rotates and moves laterally outward (Bennett movement). Stays relatively close to the original position.\n\n", options: { color: "444444", fontSize: 12 } },
{ text: "Non-Working (Orbiting) Condyle:\n", options: { bold: true, color: TEAL, fontSize: 13 } },
{ text: "Translates anteriorly, inferiorly, and medially along the articular eminence. Guided by the condylar inclination (SCI ~33°).\n\n", options: { color: "444444", fontSize: 12 } },
{ text: "Bennett Angle: ~15° (range 0-30°)\nMaximum lateral excursion: 10-12mm", options: { color: NAVY, fontSize: 12, bold: true } }
], { x: 0.65, y: 1.3, w: 5.1, h: 5.7, valign: "top", margin: 6 });
// Right: four colored info cards
const cards = [
{ title: "Frontal Envelope Shape", color: TEAL, body: "Diamond/rhombus shape when viewed frontally. CO at top, maximum opening at bottom, lateral excursions at sides. Each lateral excursion is ~10-12mm." },
{ title: "Lateral Border Determinants", color: GOLD, body: "Working side: ligaments of TMJ limit lateral movement. Non-working side: slope of articular eminence and medial wall of condylar fossa guide orbiting condyle." },
{ title: "Functional vs Border", color: ORANGE, body: "Chewing strokes use only 1-3mm of lateral excursion. The full 10-12mm border is the physiological limit — rarely accessed in normal function." },
{ title: "Articulator Programming", color: "7B5EA7", body: "Bennett angle set on Hanau H2 via lateral interocclusal records. Controls non-working condyle path. Affects cusp-fossa contacts in lateral excursions." },
];
cards.forEach((c, i) => {
const row = Math.floor(i / 2);
const col = i % 2;
const x = 6.45 + col * 3.35;
const y = 1.2 + row * 3.0;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w: 3.1, h: 2.7,
fill: { color: WHITE }, line: { color: c.color, pt: 2 }, rectRadius: 0.1
});
s.addShape(pres.shapes.RECTANGLE, {
x, y, w: 3.1, h: 0.4,
fill: { color: c.color }, line: { color: c.color }
});
s.addText(c.title, {
x: x + 0.1, y: y + 0.02, w: 2.9, h: 0.36,
fontSize: 11.5, bold: true, color: WHITE, margin: 0, align: "left", valign: "middle"
});
s.addText(c.body, {
x: x + 0.12, y: y + 0.45, w: 2.86, h: 2.15,
fontSize: 11.5, color: "333333", valign: "top", margin: 4
});
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 8 — Clinical Implications Overview
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5,
fill: { color: LGRAY }, line: { color: LGRAY }
});
lightHeading(s, "Clinical Implications — Overview", "Six domains where the envelope governs treatment decisions");
if (imgClinical && !imgClinical.error) {
s.addImage({ data: imgClinical.base64, x: 0.3, y: 1.05, w: 12.7, h: 6.2 });
} else {
s.addText("Clinical implications diagram unavailable", { x: 1, y: 3, w: 11, h: 1, fontSize: 16, color: "999999", align: "center" });
}
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 9 — Complete Dentures
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkBg(s);
topBar(s, TEAL);
chip(s, "Clinical Application", 0.6, 0.2, TEAL);
s.addText("Complete Dentures & the Envelope", {
x: 0.6, y: 0.65, w: 12, h: 0.65,
fontSize: 28, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
const points = [
{ icon: "01", head: "CR as the Only Reference", body: "With no natural teeth, CO cannot be registered. Centric relation — the superior border of the posterior envelope — is the ONLY reproducible position available. All denture occlusion is built around CR." },
{ icon: "02", head: "Bilateral Balanced Occlusion", body: "Dentures must contact on both sides in all excursions (protrusive + lateral) to prevent tipping. Guided by Hanau's Quint: condylar guidance, incisal guidance, occlusal plane, compensating curve, and cusp height." },
{ icon: "03", head: "Protrusive Registration", body: "Patient protrudes 5-6mm within the anterior border of the envelope. The resulting wax record programs the condylar inclination (SCI) on the articulator — average ~33°." },
{ icon: "04", head: "Lateral Registration", body: "Patient moves jaw laterally to record the Bennett angle. Programs the non-working (orbiting) condyle path on the articulator (~15° average)." },
{ icon: "05", head: "Freedom in Centric", body: "A 1mm antero-posterior range of tooth contact (\"long centric\") is built into dentures. This accommodates the natural CR-CO slide and reduces stress on residual ridges." },
{ icon: "06", head: "Occlusal Plane Orientation", body: "The occlusal plane (part of the superior envelope border) must be set parallel to the ala-tragus line. Incorrect positioning shifts the entire occlusal relationship outside functional norms." },
];
points.forEach((p, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const x = 0.4 + col * 6.5;
const y = 1.5 + row * 1.85;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w: 6.1, h: 1.7,
fill: { color: "0F2555" }, line: { color: "1A3A6E" }, rectRadius: 0.1
});
s.addShape(pres.shapes.OVAL, {
x: x + 0.15, y: y + 0.35, w: 0.55, h: 0.55,
fill: { color: TEAL }, line: { color: TEAL }
});
s.addText(p.icon, {
x: x + 0.15, y: y + 0.35, w: 0.55, h: 0.55,
fontSize: 10, bold: true, color: WHITE, align: "center", valign: "middle", margin: 0
});
s.addText(p.head, {
x: x + 0.82, y: y + 0.08, w: 5.1, h: 0.38,
fontSize: 13, bold: true, color: GOLD, fontFace: "Calibri", margin: 0, valign: "middle"
});
s.addText(p.body, {
x: x + 0.82, y: y + 0.48, w: 5.1, h: 1.1,
fontSize: 11.5, color: "B0C8E0", fontFace: "Calibri", valign: "top", margin: 2
});
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 10 — TMD Diagnosis Using the Envelope
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5,
fill: { color: LGRAY }, line: { color: LGRAY }
});
lightHeading(s, "TMD Diagnosis — Envelope as a Diagnostic Tool", "How alterations in the envelope reveal pathology");
const findings = [
{ sign: "Reduced Maximum Opening (<35mm)", dx: "Capsular fibrosis, disc displacement without reduction, muscle splinting (trismus), ankylosis", color: ORANGE },
{ sign: "Deviation on Opening", dx: "Unilateral disc displacement with reduction — the mandible deviates TOWARD the affected side, then corrects (S-curve deviation)", color: TEAL },
{ sign: "Deflection on Opening", dx: "Unilateral restriction without correction — mandible deflects toward affected side throughout opening. Indicates muscle restriction or bony limitation.", color: GOLD },
{ sign: "Reduced Lateral Excursion", dx: "Contralateral lateral pterygoid dysfunction or bony/disc pathology limits orbiting condyle translation. <7mm on one side is significant.", color: "7B5EA7" },
{ sign: "Reduced Protrusion (<6mm)", dx: "Bilateral disc displacement, retrodiscal inflammation, or muscle hypertonicity limiting bilateral condylar translation.", color: ORANGE },
{ sign: "CR-CO Discrepancy >2mm", dx: "May indicate masticatory muscle dysfunction, condylar resorption, or occlusal prematurities driving the mandible away from true CR.", color: TEAL },
];
findings.forEach((f, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const x = 0.4 + col * 6.5;
const y = 1.22 + row * 1.98;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w: 6.1, h: 1.82,
fill: { color: WHITE }, line: { color: f.color, pt: 1.5 }, rectRadius: 0.1,
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.07 }
});
s.addShape(pres.shapes.RECTANGLE, {
x, y, w: 6.1, h: 0.38,
fill: { color: f.color }, line: { color: f.color }
});
s.addText(f.sign, {
x: x + 0.12, y: y + 0.01, w: 5.86, h: 0.36,
fontSize: 12.5, bold: true, color: WHITE, margin: 0, valign: "middle"
});
s.addText([
{ text: "Suggests: ", options: { bold: true, color: NAVY, fontSize: 12 } },
{ text: f.dx, options: { color: "333333", fontSize: 12 } }
], { x: x + 0.15, y: y + 0.43, w: 5.8, h: 1.32, valign: "top", margin: 3 });
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 11 — Fixed Prosthodontics & Implants
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkBg(s);
topBar(s, ORANGE);
s.addText("Fixed Prosthodontics & Implant Considerations", {
x: 0.6, y: 0.15, w: 12, h: 0.65,
fontSize: 26, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
s.addText("The envelope governs every restoration placed in the mouth", {
x: 0.6, y: 0.78, w: 12, h: 0.28,
fontSize: 13, color: GOLD, italic: true, margin: 0
});
// Fixed prosthodontics left
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.4, y: 1.15, w: 6.1, h: 6.05,
fill: { color: "0F2555" }, line: { color: ORANGE, pt: 2 }, rectRadius: 0.12
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 1.15, w: 6.1, h: 0.45,
fill: { color: ORANGE }, line: { color: ORANGE }
});
s.addText("Fixed Prosthodontics", {
x: 0.55, y: 1.17, w: 5.8, h: 0.4,
fontSize: 14, bold: true, color: WHITE, margin: 0, valign: "middle"
});
const fpPoints = [
{ h: "Identify CR-CO Before Treatment", b: "Map the discrepancy first. Restorations built to MIP without checking CR may trap the condyle in a displaced position." },
{ h: "Freedom in Centric", b: "Build 1mm of anteroposterior latitude into posterior tooth contacts. Prevents posterior interference during functional CR-to-CO slide." },
{ h: "Anterior Guidance Must Match", b: "Incisal guidance angle (part of the envelope's superior border) must be reproduced accurately or steeper/shallower restorations will alter posterior disocclusion." },
{ h: "Protrusive Envelope Clearance", b: "Crown heights must not exceed the protrusive border of the envelope. Overcontoured lingual surfaces will create premature protrusive contacts." },
{ h: "Group Function vs Canine Protection", b: "Both occlusal schemes must keep all excursive contacts within the lateral border. Lateral interferences outside the functional zone cause fremitus and tooth mobility." },
];
fpPoints.forEach((pt, i) => {
s.addText([
{ text: pt.h + "\n", options: { bold: true, color: GOLD, fontSize: 12.5, breakLine: true } },
{ text: pt.b, options: { color: "B0C8E0", fontSize: 11.5 } }
], { x: 0.6, y: 1.68 + i * 1.02, w: 5.7, h: 0.95, valign: "top", margin: 3 });
if (i < fpPoints.length - 1) {
s.addShape(pres.shapes.LINE, {
x: 0.6, y: 1.68 + (i + 1) * 1.02 - 0.04, w: 5.7, h: 0,
line: { color: "1A3A6E", pt: 0.75 }
});
}
});
// Implants right
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 6.8, y: 1.15, w: 6.1, h: 6.05,
fill: { color: "0F2555" }, line: { color: TEAL, pt: 2 }, rectRadius: 0.12
});
s.addShape(pres.shapes.RECTANGLE, {
x: 6.8, y: 1.15, w: 6.1, h: 0.45,
fill: { color: TEAL }, line: { color: TEAL }
});
s.addText("Implant-Supported Prosthetics", {
x: 6.95, y: 1.17, w: 5.8, h: 0.4,
fontSize: 14, bold: true, color: WHITE, margin: 0, valign: "middle"
});
const impPoints = [
{ h: "No Periodontal Ligament = No Proprioception", b: "Implants lack PDL mechanoreceptors. The neuromuscular envelope modifiers are absent — functional movements may exceed predicted limits, causing overload." },
{ h: "Wider Centric Stop Required", b: "Broader flat occlusal contacts (\"wide centric\") compensate for lack of proprioceptive feedback. Helps distribute forces within the envelope boundary." },
{ h: "Shallow Cusp Angles (0-10°)", b: "Reduce lateral force vectors during excursive movements that may exceed the implant fixture's tolerance. Keeps forces within the functional zone." },
{ h: "Avoid Cantilevers in Lateral Envelope", b: "Cantilever extensions are particularly vulnerable to off-axis forces generated at the lateral borders. Strict occlusal control is mandatory." },
{ h: "Implant Parafunction & Envelope", b: "Bruxism extends movements to the full envelope borders — not just the functional zone. Night guards are critical to protect implant components from border-movement overload." },
];
impPoints.forEach((pt, i) => {
s.addText([
{ text: pt.h + "\n", options: { bold: true, color: GOLD, fontSize: 12.5, breakLine: true } },
{ text: pt.b, options: { color: "B0C8E0", fontSize: 11.5 } }
], { x: 7.0, y: 1.68 + i * 1.02, w: 5.7, h: 0.95, valign: "top", margin: 3 });
if (i < impPoints.length - 1) {
s.addShape(pres.shapes.LINE, {
x: 7.0, y: 1.68 + (i + 1) * 1.02 - 0.04, w: 5.7, h: 0,
line: { color: "1A3A6E", pt: 0.75 }
});
}
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 12 — Orthodontics & Envelope Changes
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5,
fill: { color: LGRAY }, line: { color: LGRAY }
});
lightHeading(s, "Orthodontics — How Treatment Changes the Envelope", "Tooth movement reshapes the superior border of the envelope");
const rows = [
["Condition / Treatment", "Effect on Envelope", "Clinical Action"],
["Deep overbite correction", "Increases vertical dimension → expands inferior border of sagittal envelope", "Re-record CR after leveling and aligning"],
["Extraction treatment", "May alter incisal guidance angle (anterior envelope border) if incisors are retracted", "Monitor overjet/overbite changes during retraction"],
["Class II correction (mandibular advancement)", "Repositions CO relative to envelope — condyle may be displaced anteriorly", "Verify CR position with records before finalizing occlusion"],
["Class III treatment / orthognathic surgery", "Surgically repositions the mandible — entire envelope shifts spatially", "New facebow transfer and articulator mounting post-surgery"],
["Retention phase", "Teeth settle into new positions — CO stabilizes within the envelope", "Check for CR-CO discrepancy at debond and 6-month review"],
["Bruxism during orthodontics", "Forces reach envelope borders during sleep — increases risk of root resorption", "Night guard use; monitor root lengths on radiographs"],
];
// Table
const colWidths = [3.0, 4.6, 4.6];
const startX = 0.4;
const startY = 1.18;
const rowH = 0.82;
rows.forEach((row, ri) => {
row.forEach((cell, ci) => {
const cx = startX + colWidths.slice(0, ci).reduce((a, b) => a + b, 0);
const cy = startY + ri * rowH;
const isHeader = ri === 0;
s.addShape(pres.shapes.RECTANGLE, {
x: cx, y: cy, w: colWidths[ci], h: rowH,
fill: { color: isHeader ? NAVY : (ri % 2 === 0 ? WHITE : "EEF4FB") },
line: { color: "D0DCE8", pt: 0.75 }
});
s.addText(cell, {
x: cx + 0.08, y: cy + 0.04, w: colWidths[ci] - 0.16, h: rowH - 0.08,
fontSize: isHeader ? 12.5 : 11.5,
bold: isHeader,
color: isHeader ? WHITE : (ci === 0 ? NAVY : "333333"),
fontFace: "Calibri",
valign: "middle",
margin: 3
});
});
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 13 — Summary & Key Takeaways
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkBg(s);
topBar(s, GOLD);
// Left accent bar
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0.08, w: 0.06, h: 7.42,
fill: { color: GOLD }, line: { color: GOLD }
});
s.addText("Summary & Key Takeaways", {
x: 0.6, y: 0.15, w: 9, h: 0.65,
fontSize: 28, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
chip(s, "Posselt's Envelope", 0.6, 0.88, TEAL);
const takeaways = [
{ num: "1", text: "The envelope defines the MAXIMUM 3D space available for jaw movement — all restorations, prostheses, and orthodontic outcomes must respect its borders." },
{ num: "2", text: "Centric Relation (CR) is the key reference on the posterior-superior border — reproducible, ligament-determined, and the foundation of full occlusal rehabilitation." },
{ num: "3", text: "The CR-CO discrepancy (0-1mm) is physiologically normal. Discrepancies >1mm require evaluation and may signal TMD or occlusal disease." },
{ num: "4", text: "The functional chewing zone occupies only a small fraction of the total envelope — meaning patients are most comfortable when restorations keep them in this zone." },
{ num: "5", text: "Alterations in envelope shape (reduced opening, deviation, restricted lateral excursion) are diagnostic signs of TMJ, muscle, or occlusal pathology." },
{ num: "6", text: "The Hanau H2 articulator mechanically reproduces the superior border and condylar paths of the envelope through five interrelated adjustable parameters (Hanau's Quint)." },
];
takeaways.forEach((t, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const x = 0.4 + col * 6.5;
const y = 1.5 + row * 1.85;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w: 6.1, h: 1.7,
fill: { color: "0F2555" }, line: { color: "1A3A6E" }, rectRadius: 0.1
});
s.addShape(pres.shapes.OVAL, {
x: x + 0.15, y: y + 0.57, w: 0.52, h: 0.52,
fill: { color: GOLD }, line: { color: GOLD }
});
s.addText(t.num, {
x: x + 0.15, y: y + 0.57, w: 0.52, h: 0.52,
fontSize: 13, bold: true, color: NAVY, align: "center", valign: "middle", margin: 0
});
s.addText(t.text, {
x: x + 0.82, y: y + 0.12, w: 5.15, h: 1.46,
fontSize: 12, color: "C8DAF0", fontFace: "Calibri", valign: "middle", margin: 4
});
});
}
// ══════════════════════════════════════════════════════════════════════════
// SLIDE 14 — Thank You / References
// ══════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkBg(s);
topBar(s, TEAL);
s.addShape(pres.shapes.OVAL, {
x: 8.5, y: 1.0, w: 5.5, h: 5.5,
fill: { color: "0F2555", transparency: 20 }, line: { color: "0F2555", transparency: 20 }
});
s.addText("Thank You", {
x: 0.8, y: 1.4, w: 8, h: 1.1,
fontSize: 52, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
s.addText("Posselt's Envelope of Motion\nand Clinical Implications in Prosthodontics", {
x: 0.8, y: 2.55, w: 8, h: 0.9,
fontSize: 16, color: GOLD, italic: true, fontFace: "Calibri", margin: 0
});
s.addShape(pres.shapes.LINE, {
x: 0.8, y: 3.6, w: 5, h: 0,
line: { color: TEAL, pt: 2 }
});
s.addText("Key References", {
x: 0.8, y: 3.8, w: 8, h: 0.4,
fontSize: 15, bold: true, color: TEAL, margin: 0
});
const refs = [
"Posselt U. (1952). Studies in the mobility of the human mandible. Acta Odontologica Scandinavica.",
"Bennett NG. (1906). A contribution to the study of the movements of the mandible. Proc R Soc Med.",
"Hanau RL. (1926). Articulation defined, analyzed and formulated. J Am Dent Assoc.",
"Okeson JP. (2019). Management of Temporomandibular Disorders and Occlusion. 8th ed. Elsevier.",
"Zarb GA, Bolender CL. (2004). Prosthodontic Treatment for Edentulous Patients. 12th ed. Mosby.",
"Ash MM, Ramfjord SP. (1995). Occlusion. 4th ed. Saunders.",
];
refs.forEach((r, i) => {
s.addText([
{ text: "• ", options: { color: GOLD, bold: true } },
{ text: r, options: { color: MIDGRAY, fontSize: 11 } }
], { x: 0.8, y: 4.25 + i * 0.47, w: 8.5, h: 0.42, valign: "middle", margin: 2 });
});
}
// ══════════════════════════════════════════════════════════════════════════
// WRITE OUTPUT
// ══════════════════════════════════════════════════════════════════════════
const outPath = "/home/daytona/workspace/posselt-presentation/Posselts_Envelope_of_Motion.pptx";
pres.writeFile({ fileName: outPath })
.then(() => console.log("DONE:", outPath))
.catch(e => { console.error("ERROR:", e); process.exit(1); });
cd /home/daytona/workspace/posselt-presentation && node build.js 2>&1
cd /home/daytona/workspace/posselt-presentation && \ node /home/daytona/skills/shared/scripts/fetch_images.js "https://cdn.orris.care/image-gen/af009503bd7241a897b42af7054e868a.png" > img1.json && \ echo "img1 done" && \ node /home/daytona/skills/shared/scripts/fetch_images.js "https://cdn.orris.care/image-gen/7a25d2fe62b74b6ea9f134ed406c7ccc.png" > img2.json && \ echo "img2 done" && \ node /home/daytona/skills/shared/scripts/fetch_images.js "https://cdn.orris.care/image-gen/5afb03ba83a14f2590d661f0a3864b2c.png" > img3.json && \ echo "img3 done"
~/posselt-presentation/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/posselt-presentation/build.js'
~/posselt-presentation/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/posselt-presentation/build.js'
cd /home/daytona/workspace/posselt-presentation && node build.js 2>&1
grep -n "require" /home/daytona/workspace/posselt-presentation/build.js | head -20
~/posselt-presentation/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/posselt-presentation/build.js'
cd /home/daytona/workspace/posselt-presentation && node build.js 2>&1
ls -lh /home/daytona/workspace/posselt-presentation/Posselts_Envelope_of_Motion.pptx
Posselts Envelope of Motion
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title slide - bold typographic design |
| 2 | What is Posselt's Envelope? - definition, historical context, Posselt's quote |
| 3 | Envelope Diagram - sagittal + frontal views (custom generated diagram) |
| 4 | Key Border Positions - CR, CO, max opening, protrusion with annotations |
| 5 | Border Movements in Detail - four borders of the sagittal envelope |
| 6 | CR vs CO: The Critical Discrepancy - side-by-side comparison, clinical rule |
| 7 | Lateral Envelope & Bennett Movement - working/non-working condyle mechanics |
| 8 | Clinical Implications Overview - infographic of 6 domains |
| 9 | Complete Dentures - 6 numbered points on CR registration, bilateral balance, freedom in centric |
| 10 | TMD Diagnosis - 6 envelope findings mapped to diagnoses |
| 11 | Fixed Prosthodontics & Implants - two-column comparison of key rules |
| 12 | Orthodontics - table of treatment effects on the envelope |
| 13 | Summary & 6 Key Takeaways |
| 14 | Thank You + 6 key references (Posselt, Bennett, Hanau, Okeson, Zarb, Ash) |