Vestibular rehabilitation in detail according to standard textbook of ent
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, detailed content from both major ENT textbooks. Let me compile the full detailed answer.
Vestibular Rehabilitation (VR)
(Based on Cummings Otolaryngology Head and Neck Surgery and Scott-Brown's Otorhinolaryngology Head & Neck Surgery)
1. Definition and Rationale
Vestibular rehabilitation is a supervised exercise-based programme designed to facilitate the natural process of vestibular compensation and to address the functional deficits, dizziness, and postural instability arising from central or peripheral vestibular disorders.
A unique feature of the central nervous system is its capacity to adjust to asymmetries in peripheral vestibular inputs. This adjustment - called vestibular compensation - occurs naturally after most vestibular insults, provided the patient resumes an active lifestyle. It requires active neuronal changes in the cerebellum and brainstem nuclei in response to sensory conflicts produced by vestibular pathology. In most cases, compensation reliably relieves vestibular symptoms provided the lesion is stable or only gradually progressive. The underlying physiologic components of this process form the foundations of VR. - Cummings Otolaryngology, p. 3264
2. Neurophysiological Basis
At least four distinct components of vestibular compensation are recognized:
a) Static Compensation
- Occurs within 24-72 hours of an acute vestibular insult, regardless of movement
- Mediated by tonic rebalancing of resting activity in the vestibular nuclei
- Minimizes side-to-side discrepancies in tonic firing rates of second-order neurons
- Provides relief from intense vertigo and vomiting but does not address dynamic (movement-related) symptoms
- Results in continued motion-provoked vertigo until dynamic compensation is achieved
b) Adaptation
- The process of VOR improvement through exposure to retinal slip
- The vestibulo-ocular reflex (VOR) maintains fixation during head movement by producing compensatory eye movements equal and opposite to head velocity (VOR gain = eye velocity/head velocity = 1.0)
- In peripheral vestibular disorders, VOR gain is reduced, causing retinal image slip and visual blurring during head rotations
- Retinal image slip acts as an error signal that drives VOR improvement
- Recent evidence shows that compensatory saccades also contribute to VOR gain improvement, particularly in more severe hypofunction
- Adaptation exercises incorporate gaze fixation with head movement to simulate retinal slip
c) Habituation
- A decrease in the magnitude of response to repetitive sensory stimuli
- The classical Cawthorne-Cooksey exercises (1940s-50s) were based on this principle
- Involves repeating the provoking movement at regular intervals until symptoms cease
- Modern evidence supports customized VR programmes focusing on individual deficits rather than generic habituation alone
d) Sensory Reweighting / Substitution
- The CNS's ability to adapt its relative reliance on specific sensory modalities depending on environmental conditions and task demands
- When a sensory input is reduced or absent, other sensory inputs are centrally upregulated
- A patient with unilateral/bilateral vestibular failure develops increased postural responses to visual motion stimulation
- VR exercises in environments with altered sensory information promote sensory reweighting
- Sensory substitution exercises (gaze shifting, remembered targets) are used for patients with poor/absent vestibular function (e.g. bilateral vestibular hyporeactivity)
Structural changes - including grey matter volume changes in specific brain areas - have been documented after functional recovery from vestibular neuritis, supporting the neuroplastic basis of VR. - Scott-Brown's Vol. 2, p. 907
3. Patient Selection Criteria (Primary, Adjunctive, and Therapeutic Trial)
Vestibular Rehabilitation as a Primary Treatment
VR is well-established as primary treatment for:
- BPPV - Particle repositioning maneuvers (Epley, Semont, etc.) with identification of the affected canal; effective in >90% of cases. Recurrence in up to 30%.
- Unilateral vestibular hypofunction (e.g. vestibular neuritis, labyrinthitis, post-surgical ablation)
- Bilateral vestibular hypofunction
- Concussion/mild TBI with persistent vestibular symptoms (Level 2-3 evidence)
- Multiple sclerosis - pilot data shows promise with gaze and postural stability exercises
Vestibular Rehabilitation as an Adjunctive Modality
VR supplements other treatments in:
- Endolymphatic hydrops / Meniere's disease (combined with medical/surgical management)
- Acoustic neuroma post-resection
- Post-ablative procedures (gentamicin labyrinthectomy, vestibular nerve section)
Vestibular Rehabilitation as a Therapeutic Trial
- In cases of diagnostic uncertainty (e.g. mixed central and peripheral pathology after head injury), a supervised 4-6 week course of VR has diagnostic value:
- Outstanding progress suggests poor compensation for a stable lesion
- Failure to improve or worsening makes an unstable lesion considerably more likely (raises suspicion of perilymph fistula, posttraumatic endolymphatic hydrops)
- Cummings Otolaryngology, p. 3254
4. Clinical Assessment Before VR
A thorough assessment is required prior to initiating VR:
Bedside vestibular function testing:
- Spontaneous, gaze-evoked and positional nystagmus
- Dynamic visual acuity (DVA)
- Head thrust test (video or clinical)
- Vestibular/Ocular Motor Screening (VOMS) - 5 domains: smooth pursuit, horizontal and vertical saccades, near point of convergence, horizontal VOR, visual motion sensitivity
Validated outcome questionnaires:
| Measure | Purpose |
|---|---|
| Dizziness Handicap Inventory (DHI) | Subjective dizziness and functional ability (0=no handicap, 100=severe) |
| Activities-specific Balance Confidence scale (ABC) | Confidence in gait without falling (<85% = potential faller) |
| Vertigo Symptom Scale | Symptom severity and frequency |
| Situational Characteristic Questionnaire | Visual dependency assessment |
Functional/objective balance tests:
| Test | Significance |
|---|---|
| Dynamic Gait Index (DGI) | <19/24 predicts falls in community-dwelling elderly |
| Functional Gait Assessment (FGA) | ≤22/30 = 100% sensitivity for predicting prospective falls |
| Timed Up and Go (TUG) | >11 seconds = increased fall risk in vestibular population |
| Balance Evaluation Systems Test (BEST) | Identifies specific impaired systems underlying balance |
| 10-metre walk test (gait speed) | <0.6 m/s = poor health/function; >1.0 m/s = healthier aging |
| Modified CTSIB | Static and dynamic balance on various sensory conditions |
The Vestibular Evidence Database to Guide Effectiveness (VEDGE) provides a full list of validated VR outcome measures.
Treatment goal setting includes:
- Improve functional balance, gait, and daily activities
- Decrease falls risk
- Decrease symptom severity
- Improve VOR function
- Improve sensory integration and reweighting
- Patient education
5. Vestibular Rehabilitation: Common Techniques
The VR therapist designs a customized programme addressing the individual patient's specific deficits. General exercise categories include:
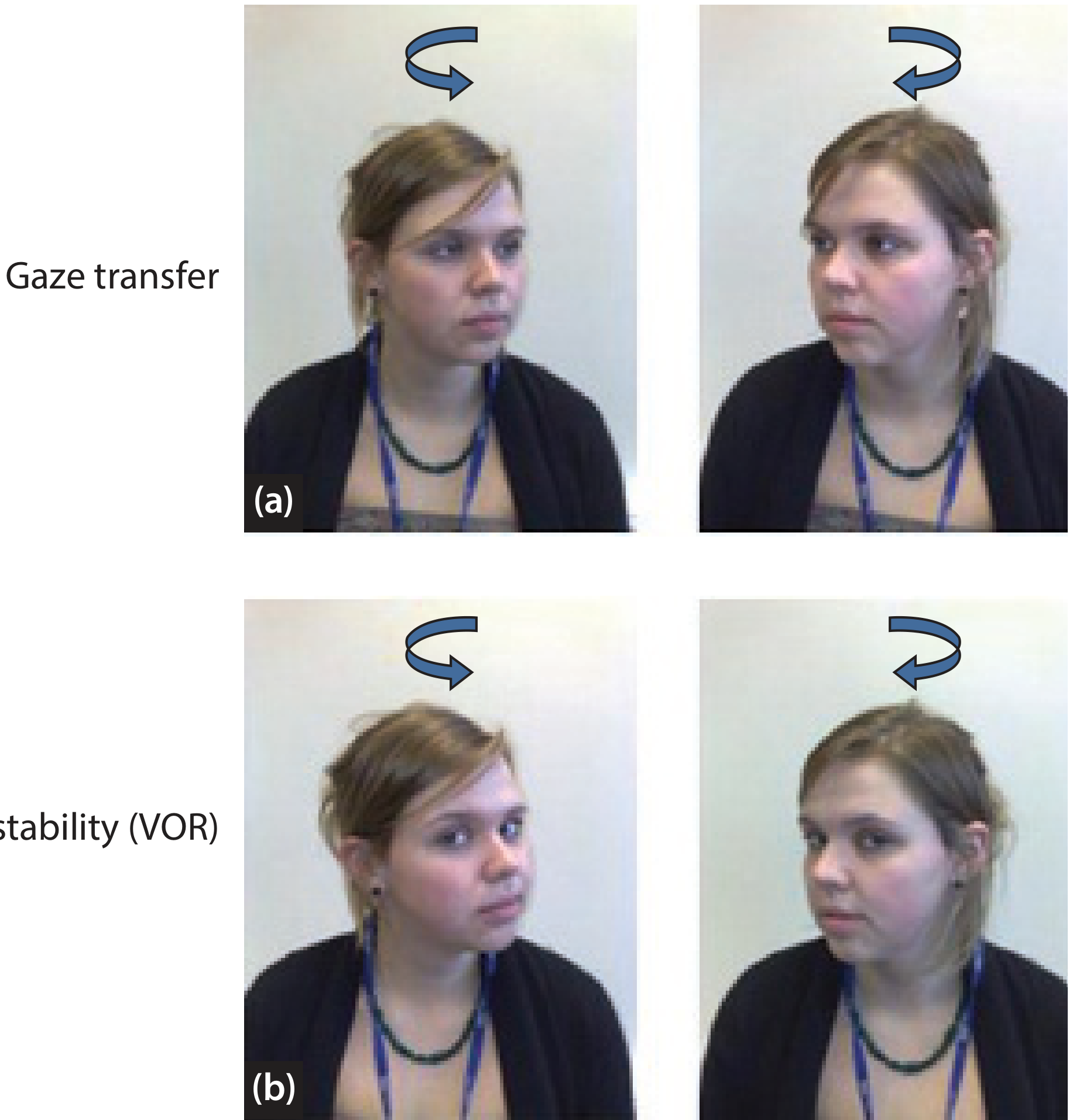
a) Gaze Stability Exercises (Adaptation Exercises)
- Principal goal: improvement in functional VOR performance and gaze stability for those with a VOR deficit
- ×1 viewing exercise (VOR ×1): Patient fixes gaze on a stationary target while moving the head side-to-side or up-and-down. Speed is gradually increased.
- ×2 viewing exercise (VOR ×2): Target moves in the direction opposite to head movement. Promotes greater retinal slip and more aggressive VOR adaptation.
- Gaze transfer exercises: patient practices the normal head-and-eye movement for transferring gaze between two objects
b) Habituation Exercises
- Designed for motion-provoked symptoms
- Patient repeats the symptom-provoking head movement or position change at regular intervals
- Symptoms should initially be provoked (mild-moderate) and gradually habituate
- Classical Cawthorne-Cooksey protocol based on this mechanism
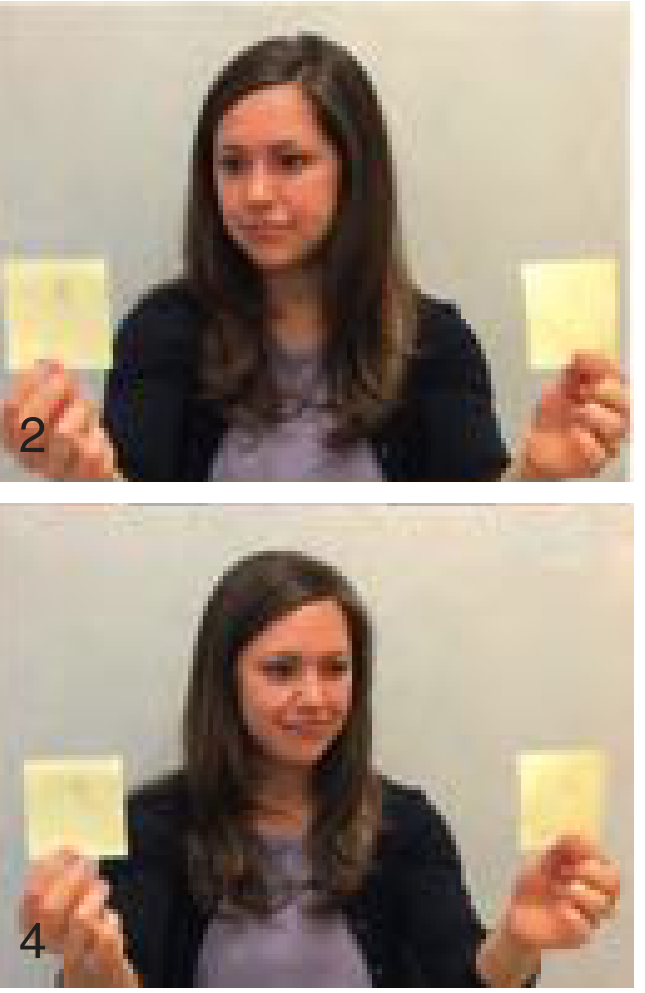
c) Sensory Substitution Exercises
- Used for patients with poor to absent vestibular function (bilateral vestibular hyporeactivity)
- Gaze shifting and remembered target exercises: Patient maintains clear visual image on a fixed target (e.g. letter X), turns head toward it, then shifts fixation to another target (letter Z) and turns head toward Z. Can be progressed to eyes-closed (remembered target) head turns
d) Postural and Balance Exercises (Vestibulospinal Reflex Training)
- Aimed at improving postural stability and gait
- Static balance exercises: narrowing the base of support, tandem standing, single-leg stance
- Exercises progressively vary:
- Surface: firm → foam → tilt boards → moving platforms
- Vision: eyes open → eyes closed → visual conflict domes
- Head position: head still → head moving during balance tasks
- Dynamic balance: weight shifting, stepping responses, multidirectional stepping
- Fall prevention strategies in elderly patients
e) Sensory Strategy Retraining
- Addresses disruption in appropriate sensory selection for postural stability
- Somatosensory over-reliance: exercises on foam, tilt boards, or compliant surfaces to reduce dependence on proprioception
- Visual dependency (visual vertigo): exercises with conflicting or absent visual input to learn reliance on proprioceptive and vestibular cues
- Optokinetic stimulation using rotating drums, computers, or YouTube videos promotes desensitization to visual motion; shown to improve postural stability, visually-induced dizziness, and psychological state (depression, anxiety)
f) Gait Exercises
- Walking with deliberate horizontal/vertical head turns
- Walking on varying surfaces and in complex visual environments
- Functional Gait Assessment tasks
g) Dual-Task Training
- Vestibular patients show decreased attentional resources during simultaneous cognitive and postural tasks, with deviation from linear gait path
- Progressive balance exercises (tandem standing, walking) combined with secondary cognitive tasks (counting backwards by 3s, recounting daily activities)
- Attention can be directed at one or both tasks
h) Particle Repositioning Maneuvers (for BPPV)
- Epley maneuver (canalith repositioning) for posterior SCC canalithiasis
- Semont maneuver
- Barbecue roll for horizontal SCC canalithiasis
- Use of infrared goggles to block fixation and improve canal identification via nystagmus patterns
6. Novel and Supplementary Techniques
Virtual Reality (VR) Systems
- Full-field immersive VR (grocery store models), head-mounted devices, Nintendo Wii Fit Plus have all been studied
- Two RCTs found no significant between-group differences comparing customized VR vs. VR-based rehabilitation for gait speed, posturography, or symptoms
- This is attributed to the fact that both small- and large-field optokinetic stimulation shows similar visual-vestibular interactions - sensory reweighting occurs independently of visual field size, frequency, velocity, and texture

Vestibular Balance Rehabilitation Therapy (VBRT)
- A specific programme combining habituation and behavioural modification (analogous to graded exercise therapy in fibromyalgia/chronic fatigue syndrome)
- Encourages "avoidance of avoidance"
- Effective against hypersensitivity to motion, improves confidence, reduces avoidance behaviour
- Early trials combining VBRT with CBT show positive effects on disability but not on core symptoms of vertigo, anxiety, or depression
- Patients must experience symptoms during exposure for compensation to occur
Optokinetic Stimulation
- Induces adaptation of VOR reflex gain
- Clinical optokinetic drums, computer screens, accessible YouTube visual stimulation
- Particularly beneficial for visual vertigo - desensitizes patients to visual motion
- Exposure should be gradual and progressive
7. General Principles and Programme Characteristics
Key features of any VR programme:
- Specificity - exercises target documented deficits
- Repetition - consistent practice (typically 2-3 times per day at home)
- Progression - exercises are made progressively more difficult
- Patient education - explain that symptoms may initially worsen before improving; improvement is uneven
Patients should stop and seek advice if they experience:
- Neck pain
- Loss of consciousness or vision
- Numbness, weakness or tingling in face/limbs
- Increased migraine frequency
8. Role of Medication
- Vestibular suppressant medications (e.g. antihistamines, benzodiazepines) and other centrally acting agents have been shown to delay the time course of recovery during vestibular rehabilitation
- Whenever possible, these should be tapered or discontinued
- However, if essential for complicating medical conditions or symptom relief during the programme, their continued use does not appear to dramatically reduce the chances of a satisfactory ultimate outcome
- Cummings Otolaryngology, p. 3265
9. Expected Results and Evidence
| Population | Evidence |
|---|---|
| Unilateral vestibular hypofunction | Cochrane review: moderate to strong evidence for symptom reduction and functional improvement |
| BPPV | >90% success with particle repositioning; 30% recurrence |
| Post-surgical ablation | Highly beneficial; similar results to vestibular neuritis |
| Bilateral vestibular hypofunction | Beneficial but prognosis is guarded |
| Concussion/mild TBI | Level 2-3 evidence (no Level 1 RCTs in systematic review) |
| Multiple sclerosis | Promising pilot data for gaze and postural exercises |
| Migraine-associated vestibular symptoms | Effective when combined with treatment of primary migraine disorder |
Factors predicting poorer prognosis:
- Severe bilateral peripheral lesions
- Combined central and peripheral vestibular deficits
- Headache syndromes after head injury
- Established long-term disability
- Elderly patients with multisensory dysfunction (vision, hearing, proprioception impairment)
Overall: Studies consistently demonstrate significant evidence supporting VR as a major management tool for patients with vestibular and balance disorders.
Summary Table: VR Mechanisms and Corresponding Exercises
| Mechanism | Exercise Type | Example |
|---|---|---|
| Adaptation (VOR) | Gaze stability | VOR ×1, VOR ×2 exercises with head movement |
| Habituation | Repetitive provocation | Cawthorne-Cooksey, head-movement sequences |
| Sensory substitution | Remembered target, gaze shifting | Eyes-closed head-turn to remembered target |
| Sensory reweighting | Balance on altered surfaces | Foam, tilt board, optokinetic exposure |
| Static postural control | Standing exercises | Narrow stance, tandem, single-leg with/without vision |
| Dynamic/gait stability | Walking with head turns | DGI-type tasks, obstacle courses |
| Dual-task | Cognitive-motor training | Counting while tandem walking |
| BPPV | Particle repositioning | Epley, Semont, Barbecue roll maneuvers |
Sources: Cummings Otolaryngology Head and Neck Surgery, Chapter 170 (pp. 3253-3265); Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, Chapter 68 (pp. 905-910)
This is a shared conversation. Sign in to Orris to start your own chat.