Hemangioma
Reading File
Finding Sources
Searching PubMed
hemangioma
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive information from Robbins Pathology, Sabiston Surgery, Schwartz's Surgery, Fitzpatrick's Dermatology, and Sleisenger GI. Let me compile the full answer.
Hemangioma
Definition and Overview
A hemangioma is a benign vascular tumor composed of proliferating endothelial cells that surround blood-filled cavities. They constitute 7% of all benign tumors of infancy and childhood and represent the most common benign tumor of the liver in adults. Unlike vascular malformations (which are structural, do not proliferate, and do not regress), true hemangiomas show active endothelial cell proliferation and - particularly in children - a characteristic growth-then-involution lifecycle.
Key distinction: The old term "cavernous hemangioma" was historically used for both vascular malformations AND true hemangiomas, causing confusion. The 1982 Muliken-Glowacki classification (adopted by ISSVA in 1996) formally separated vascular anomalies into:
- Vascular tumors (with cellular proliferation - hemangiomas)
- Vascular malformations (structural, named by vessel type: capillary, venous, lymphatic, arterial)
(Fitzpatrick's Dermatology, p. 2666)
Classification
Robbins Pathology Classification of Vascular Tumors:
| Benign | Intermediate | Malignant |
|---|---|---|
| Capillary hemangioma | Kaposi sarcoma | Angiosarcoma |
| Cavernous hemangioma | Hemangioendothelioma | |
| Pyogenic granuloma | ||
| Lymphangioma |
(Robbins & Kumar Basic Pathology, Table 8.4)
Types of Hemangioma
1. Capillary Hemangioma (Infantile Hemangioma - IH)
Epidemiology: Occurs in ~4% of children by 1 year of age. The most common type overall.
Sites: Skin, subcutaneous tissues, oral/mucous membranes, liver, spleen, kidneys. Typically localized to the head and neck.
Natural history:
- Absent or barely visible at birth
- Rapid proliferative growth phase in the first few months of life
- Peak size by about 9-12 months
- Spontaneous involution begins by 1-3 years; >90% completely regress by 7 years of age
Histology: Composed of thin-walled capillaries, closely packed, with scant stroma. Active endothelial cell proliferation with mitotic figures. The hallmark marker is GLUT-1 (glucose transporter protein) - positive in all stages of IH, absent in normal cutaneous vasculature and all vascular malformations.
Associations: PHACES syndrome (Posterior fossa defects, Hemangioma, Arterial anomalies, Cardiac defects, Eye abnormalities, Sternal clefting), LUMBAR syndrome.
(Schwartz's Principles of Surgery, p. 2417-2430; Fitzpatrick's Dermatology)
2. Cavernous Hemangioma
Structure: Large, dilated, irregular blood-filled vascular channels separated by thin fibrous septa. Lined by flat endothelial cells. More infiltrative than capillary hemangiomas; frequently involves deep structures.
Key differences from capillary hemangioma:
- Does not spontaneously regress
- More infiltrative, involves deep tissues
- Intravascular thrombosis and dystrophic calcification common
Brain cavernous hemangiomas: A component of von Hippel-Lindau disease (vascular lesions in cerebellum, brainstem, retina, pancreas, liver). Familial forms caused by mutations in CCM1, CCM2, CCM3 tumor suppressor genes. Genetic testing indicated for multiple lesions.
(Robbins & Kumar Basic Pathology, p. 336-337)
3. Pyogenic Granuloma
A capillary proliferation of uncertain etiology. Rapidly growing red pedunculated lesion on skin, gingiva, or oral mucosa. Histologically resembles exuberant granulation tissue. Bleeds easily, often ulcerates. ~25% follow trauma. Curettage and cautery are usually curative. Common in pregnant women (gingiva).
4. Histology images (from Robbins Pathology, Fig. 8.26):
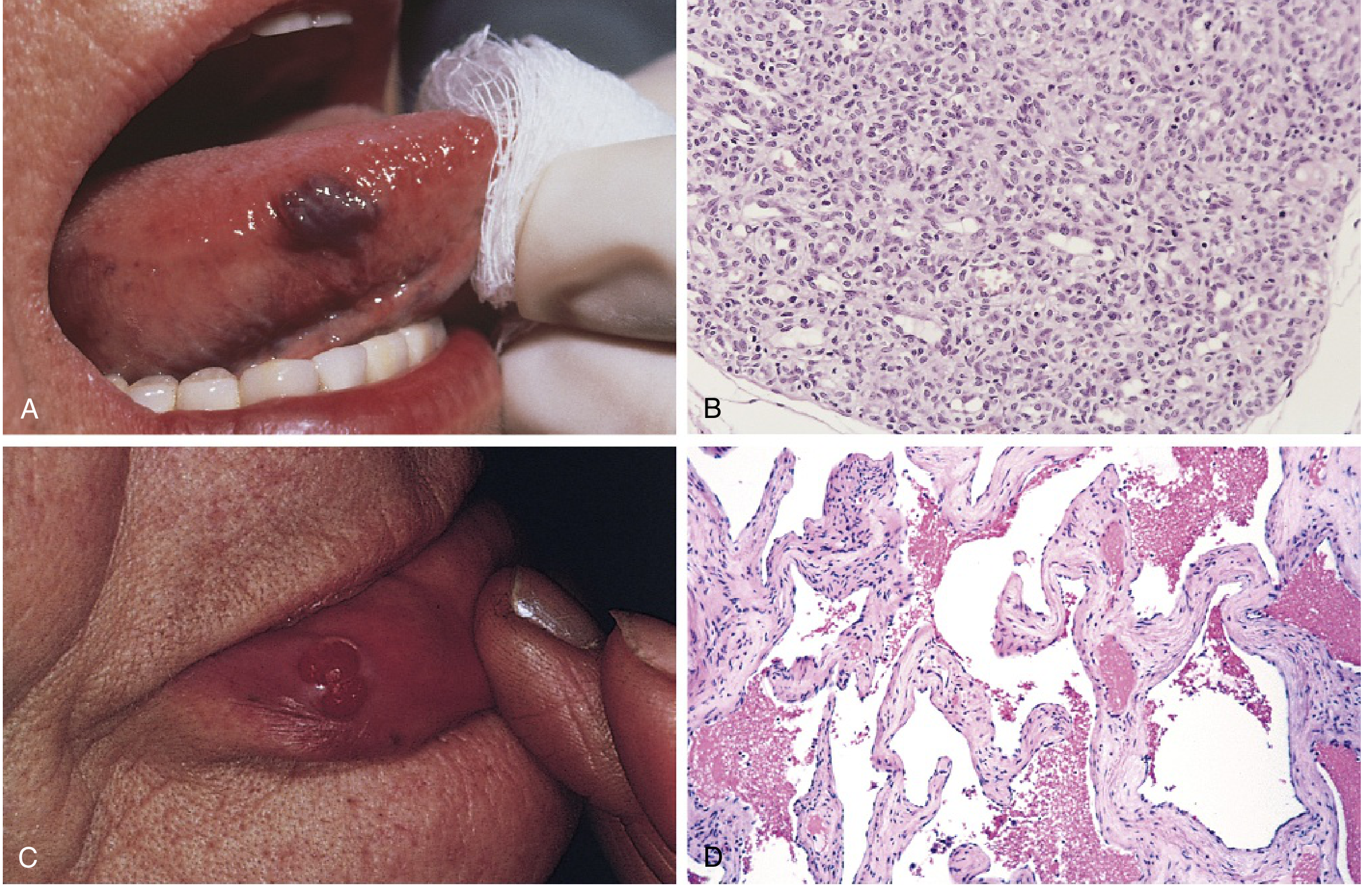
(A) Hemangioma of the tongue. (B) Infantile capillary hemangioma - closely packed endothelial cells. (C) Pyogenic granuloma of the lip. (D) Cavernous hemangioma - large, dilated, blood-filled spaces separated by fibrous stroma.
Liver Hemangioma (Hepatic Cavernous Hemangioma)
- Most common benign tumor of the liver
- F:M ratio = 3:1; mean age ~45 years
- Usually solitary, <5 cm; lesions >5 cm = "giant hemangioma"
- Enlargement by ectasia (dilation), NOT neoplasia
- Never undergoes malignant degeneration
Clinical presentation: Usually asymptomatic; found incidentally on imaging. Large lesions may cause vague upper abdominal discomfort. Spontaneous rupture is exceedingly rare.
Kasabach-Merritt syndrome: Rare but well-described: thrombocytopenia + consumptive coagulopathy associated with large hemangiomas.
Investigations:
- LFTs and tumor markers: normal
- CT/MRI: Characteristic peripheral nodular enhancement (diagnostic in most cases)
- Isotope-labeled RBC scan: accurate but rarely necessary
- Biopsy: NOT recommended - potentially dangerous and inaccurate
CT appearance:
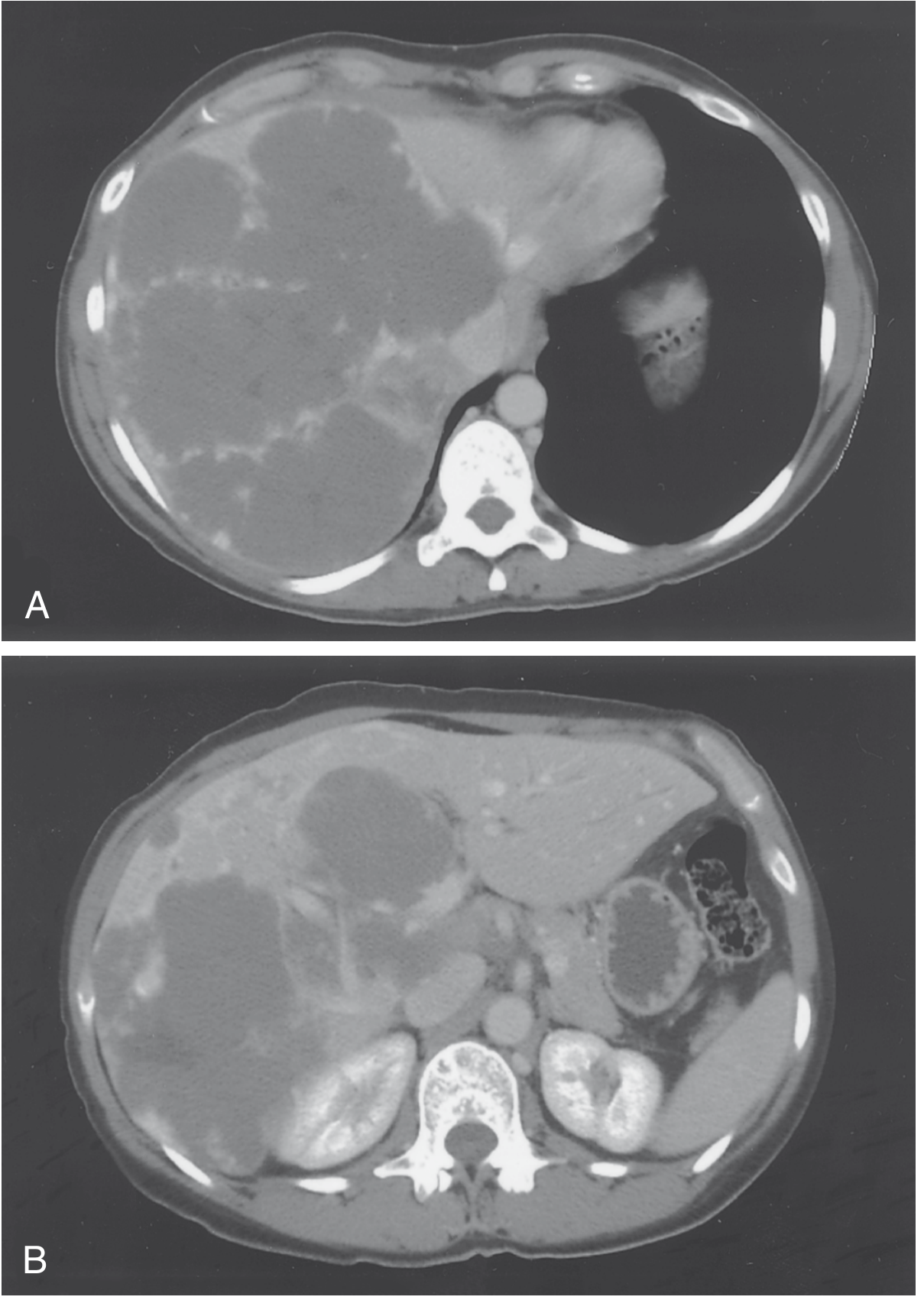
(CT showing large cavernous hemangioma displacing left and middle hepatic veins, abutting left portal vein - required extended right hepatectomy. Sabiston Textbook of Surgery, Fig. 89.32)
Management:
- Asymptomatic + secure diagnosis: observation only
- Symptomatic patients: evaluate for alternative causes first (alternative explanation found in ~50%)
- Indications for resection: symptoms with no other cause found, rupture, significant growth, Kasabach-Merritt syndrome, diagnostic uncertainty
- Preferred technique: enucleation with arterial inflow control (not anatomic resection)
(Sabiston Textbook of Surgery, p. 1895)
GI Tract Hemangioma
- Second most common vascular lesion of the colon (after AVM)
- Types: cavernous, capillary, or mixed - capillary most common in GI tract
- Most are small (few mm to 2 cm); larger lesions occur especially in the rectum
Clinical features:
- Slow occult bleeding → anemia or melena (most common)
- Large cavernous hemangioma of rectum → massive hemorrhage
- Plain films: phleboliths, displacement of rectal air column
- Barium enema: narrowing, rigidity, scalloping of rectal wall, widening of presacral space
- Endoscopy: best diagnostic tool (elevated plum-red nodules)
- CT/MRI: highly accurate for cavernous type; EUS delineates anal canal extension
Treatment:
- Small, solitary, endoscopically accessible: endoscopic ablation
- Large/multiple: surgical resection (segment vs. lesion alone)
- Cavernous rectal hemangioma causing massive bleeding: may ultimately require proctectomy
(Sleisenger & Fordtran's GI and Liver Disease, p. 623)
Infantile Hemangioma - Management
Indications for Treatment
- Functional compromise (airway, vision, feeding, musculoskeletal function)
- High-output cardiac failure (lesion consuming large % of cardiac output)
- Consumptive coagulopathy (Kasabach-Merritt phenomenon)
- Cosmetically significant or ulcerated lesions
First-Line: Propranolol (non-selective beta-blocker)
Mechanism: Discovered by chance in 2008. Causes vasoconstriction, decreased VEGF/bFGF expression, and promotion of apoptosis of proliferating endothelial cells.
Dosing protocol:
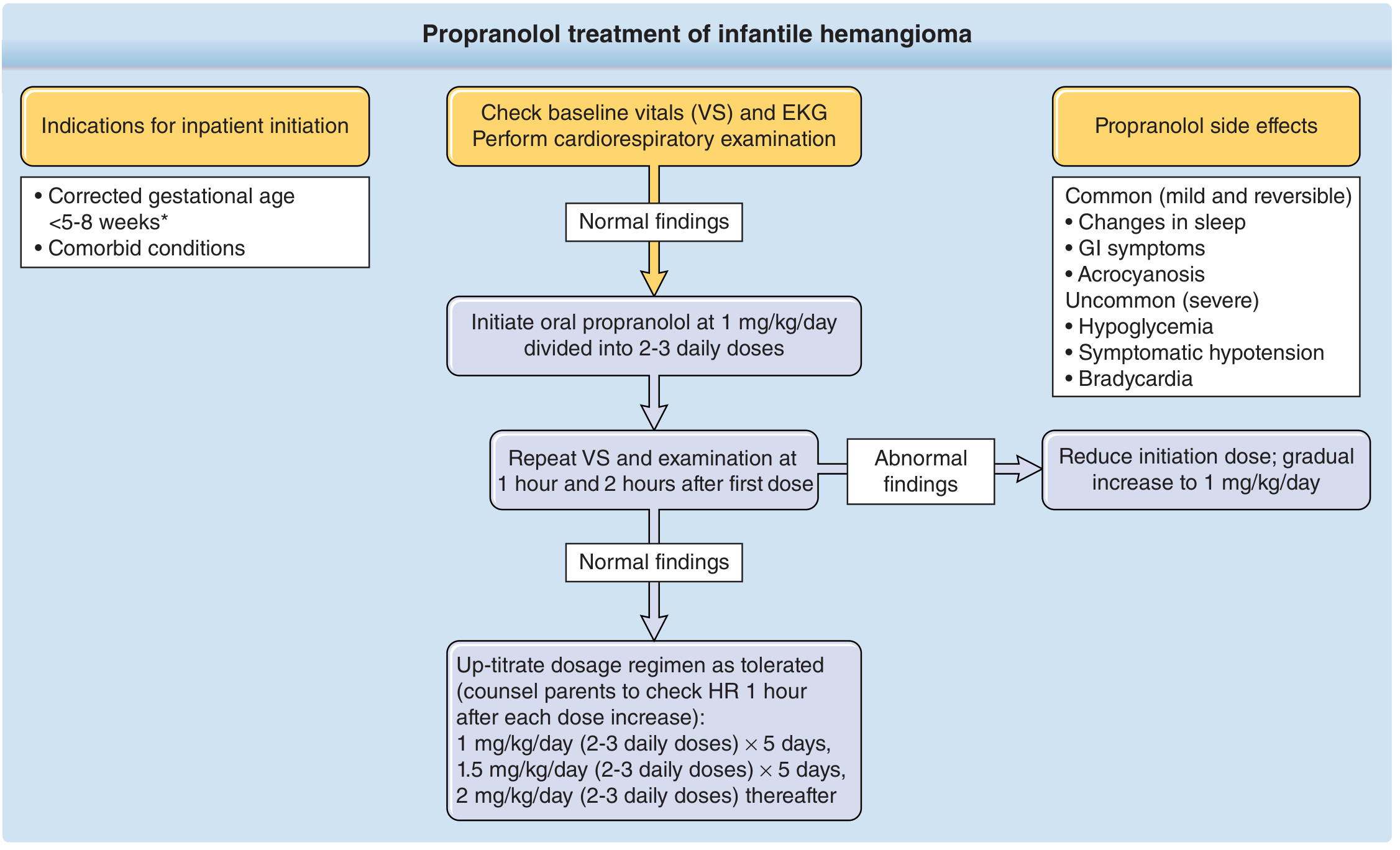
- Initiate: 1 mg/kg/day in 2-3 divided doses
- Up-titrate: 1 → 1.5 → 2 mg/kg/day over ~10 days
- Monitor VS and ECG before initiation; recheck 1-2 hours after first dose
Inpatient initiation indicated for: corrected gestational age <5-8 weeks, significant comorbidities
Side effects:
- Common (mild/reversible): sleep changes, GI symptoms, acrocyanosis
- Serious (uncommon): hypoglycemia, symptomatic hypotension, bradycardia
Other Treatment Options
| Option | Indication |
|---|---|
| Topical timolol maleate | Small, superficial lesions; ulceration |
| Systemic corticosteroids | Refractory or propranolol-intolerant |
| Interferon-α | Impedes tumor progression (less used) |
| Pulsed-dye laser (PDL) | Ulceration, superficial residual lesions |
| Surgical resection | Persistent cosmetic defect in adolescence; functional emergency |
| Preoperative embolization | Before surgical debulking of large lesions |
(Schwartz's Principles of Surgery; Fitzpatrick's Dermatology, p. 2083)
Associated Syndromes
| Syndrome | Association |
|---|---|
| Kasabach-Merritt | Large hemangioma + thrombocytopenia + consumptive coagulopathy |
| von Hippel-Lindau | Cavernous hemangiomas (cerebellum, brainstem, retina, liver) |
| PHACES | Segmental facial IH + posterior fossa defects, arterial anomalies, cardiac, eye, sternal |
| Klippel-Trenaunay | Capillary-lymphatic-venous malformation + limb hypertrophy |
| Sturge-Weber | Port-wine stain (capillary malformation) + leptomeningeal angioma + seizures |
| Diffuse intestinal hemangiomatosis | Numerous cavernous hemangiomas throughout GI tract + skin/soft tissue |
Key Facts Summary
| Feature | Capillary/Infantile HM | Cavernous HM |
|---|---|---|
| Size of vessels | Small, thin-walled capillaries | Large, dilated channels |
| Regression | Yes (>90% by age 7) | No |
| GLUT-1 | Positive | Negative |
| Main site | Skin, head/neck | Liver, brain, skin |
| Malignant potential | None | None (rare exception: radiation tx) |
| Biopsy of liver lesion | Dangerous - avoid | Dangerous - avoid |
Sources: Robbins & Kumar Basic Pathology; Sabiston Textbook of Surgery; Schwartz's Principles of Surgery; Sleisenger & Fordtran's GI and Liver Disease; Fitzpatrick's Dermatology
Hemangioma according to 2nd MBBS pathology textbook
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed for a complete, exam-focused 2nd MBBS pathology answer. Let me compile it.
Hemangioma
As per Robbins Pathology (2nd MBBS Standard)
Definition
Hemangiomas are common benign tumors composed of blood-filled vessels arising from endothelial cell proliferation. They are the most common tumor of infancy and childhood, occurring in approximately 1 in 10 individuals (Robbins Pathologic Basis of Disease, p. 489).
Classification of Vascular Tumors (Robbins, Table 11.5)
| Category | Tumors |
|---|---|
| Benign | Hemangioma (capillary, cavernous, pyogenic granuloma), Lymphangioma, Glomus tumor, Vascular ectasias |
| Intermediate-grade | Kaposi sarcoma, Hemangioendothelioma |
| Malignant | Angiosarcoma |
Types of Hemangioma
1. Capillary Hemangioma
Incidence: Most common type of hemangioma.
Sites: Skin, subcutaneous tissues, mucous membranes (oral cavity, lips), liver, spleen, kidneys.
Morphology:
- Composed of thin-walled capillaries with scant stroma
- Endothelial cells are closely packed
- Well circumscribed but unencapsulated
- Lobular architecture with a central feeding vessel
Special form - Juvenile (Strawberry) Hemangioma:
- Extremely common (1 in 200 births); can be multiple
- Present at/shortly after birth
- Rapid growth for a few months then:
- Begin to involute by 1-3 years of age
- Completely regress by 7 years in most cases
- Malignant transformation is rare
(Robbins Pathologic Basis of Disease, p. 489-490)
2. Cavernous Hemangioma
Sites: Any tissue, but liver is a common site (most common benign liver tumor). Also brain, skin.
Differences from capillary hemangioma:
| Feature | Capillary | Cavernous |
|---|---|---|
| Vessel size | Small, thin-walled | Large, dilated channels |
| Depth | Superficial | Deep structures involved |
| Regression | Spontaneous (in children) | Does NOT regress |
| Infiltration | Less | More infiltrative |
Morphology (Gross):
- Discrete red-blue soft nodule, usually <2 cm in the liver, subcapsular location
- Sharply delineated but unencapsulated
Morphology (Microscopic):
- Large, cavernous blood-filled vascular spaces separated by connective tissue stroma
- Lined by flat endothelial cells
- Intravascular thrombosis with dystrophic calcification is common
Clinical significance:
- Most are asymptomatic - found incidentally on imaging
- Can be locally destructive
- Brain hemangiomas: compression of adjacent tissue, risk of rupture
- Must be distinguished radiographically from metastatic tumors (liver)
- Associated with von Hippel-Lindau disease (vascular lesions in cerebellum, brainstem, retina, pancreas, liver); familial cerebral cavernous hemangiomas caused by mutations in CCM1, CCM2, CCM3 genes
(Robbins Pathologic Basis of Disease, p. 490; Robbins Basic Pathology, p. 336-337)
3. Pyogenic Granuloma
Definition: A capillary hemangioma/proliferation presenting as a rapidly growing red pedunculated lesion.
Sites: Skin, gingiva, oral mucosa.
Features:
- ~25% follow trauma; reach 1-2 cm within weeks
- Bleeds easily, often ulcerated
- Microscopically resembles exuberant granulation tissue
- Commonly seen in 2nd and 3rd decades
- Pregnancy tumor (Granuloma gravidarum): occurs in gingiva of pregnant females (1% of patients); may regress after delivery
Treatment: Curettage and cautery (usually curative); occasionally surgical excision.
(Robbins Pathologic Basis of Disease, p. 490)
Histopathology Images (Robbins Figures)
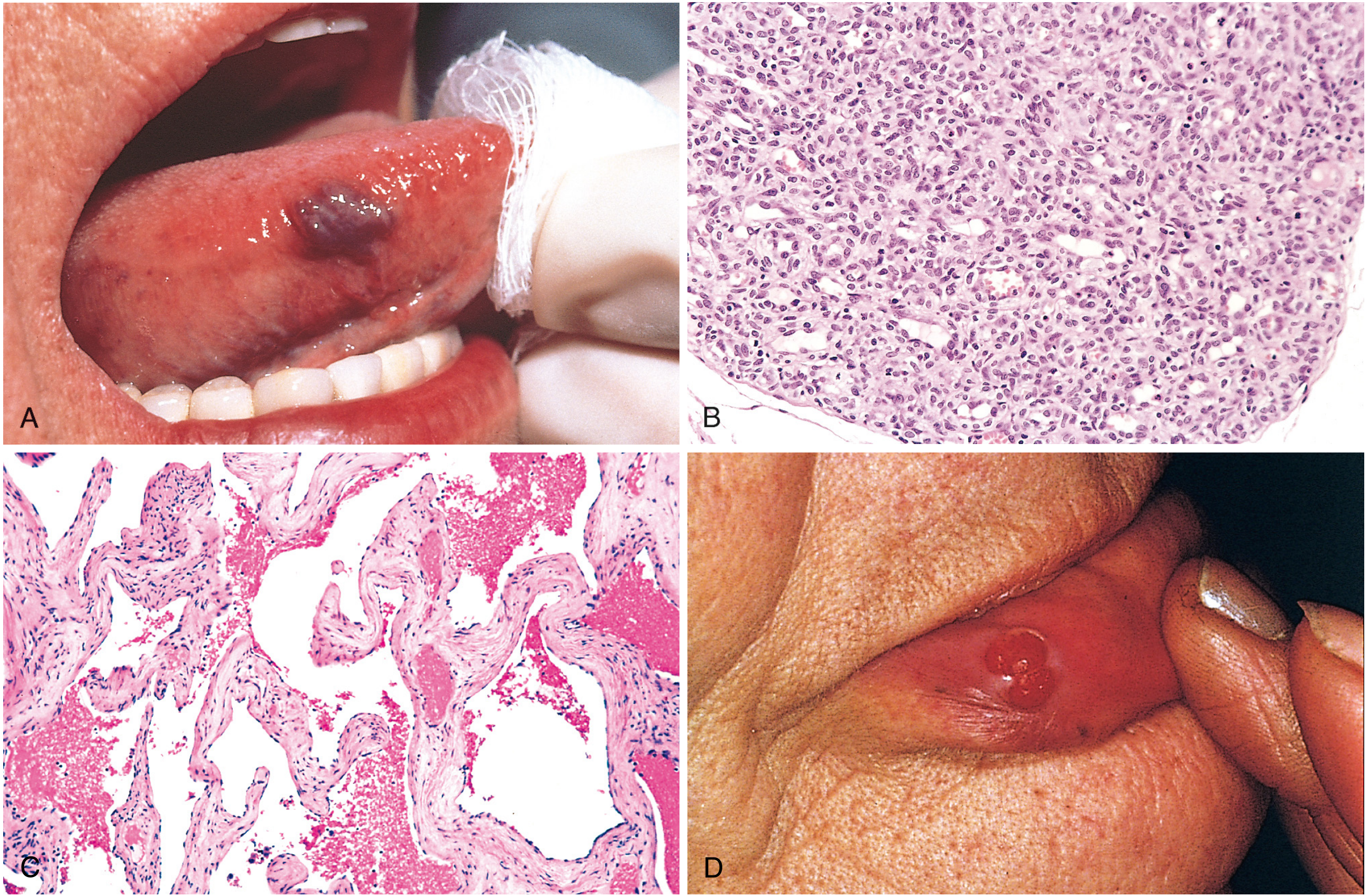
Fig. 11.29 (Robbins Pathologic Basis of Disease)
- (A) Hemangioma of the tongue
- (B) Histology of juvenile capillary hemangioma - closely packed endothelial cells, small capillary lumina, scant stroma
- (C) Histology of cavernous hemangioma - large, dilated, blood-filled spaces with fibrous septa
- (D) Pyogenic granuloma of the lip - pedunculated vascular lesion
Hepatic Cavernous Hemangioma (Liver Pathology)
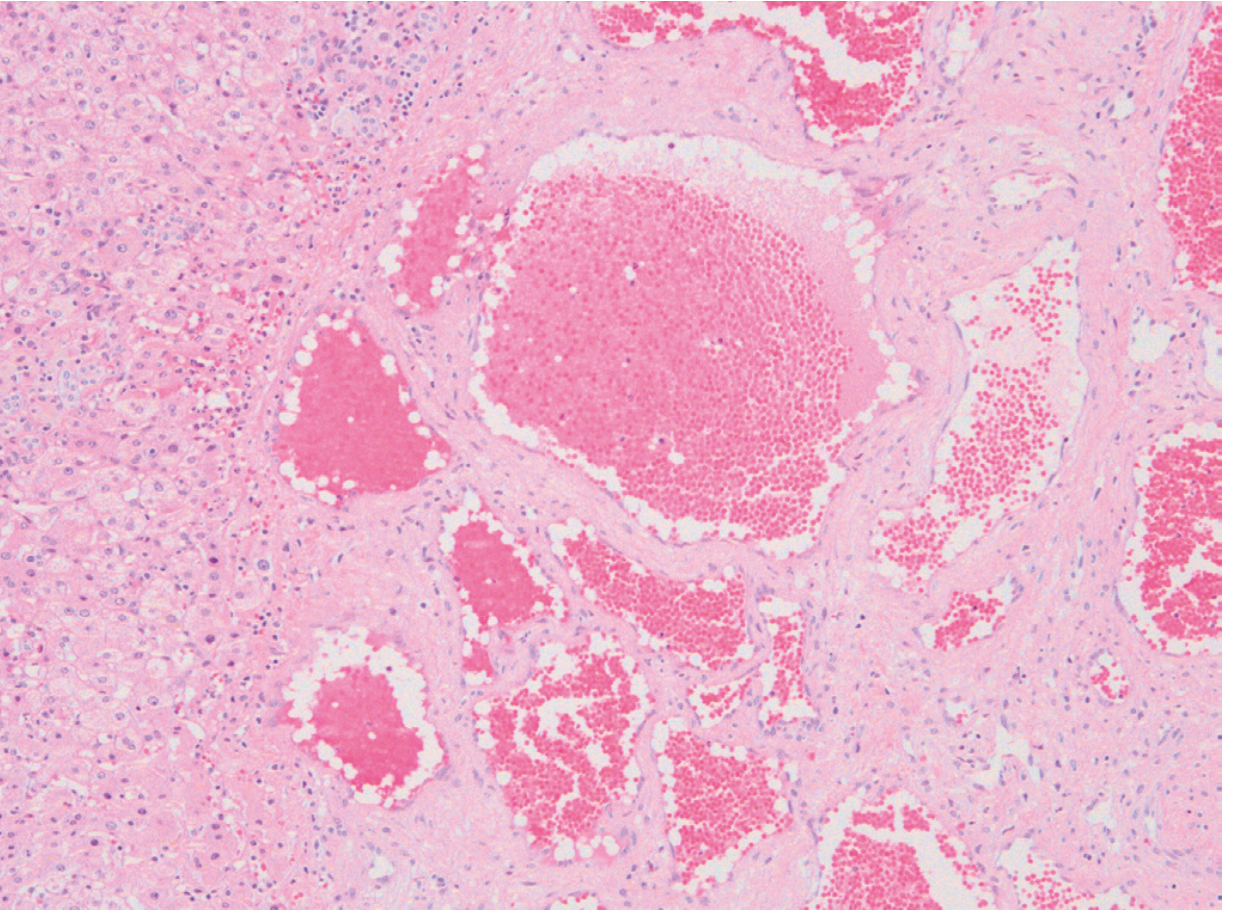
Fig. 18.50 (Robbins Pathologic Basis of Disease) - Cavernous hemangioma: dilated thin-walled blood-filled vascular channels separated by dense fibrous stroma within liver parenchyma.
- Most common benign liver tumor
- Usually <2 cm, subcapsular
- Most are asymptomatic, found incidentally
- Chief clinical significance: must be distinguished from metastatic tumors radiographically or intraoperatively
How to Distinguish Benign vs. Malignant Vascular Tumors (Robbins)
| Feature | Benign (Hemangioma) | Malignant (Angiosarcoma) |
|---|---|---|
| Vascular channels | Well-formed, obvious | Poorly organized |
| Cellularity | Low - monolayer of bland ECs | Solidly cellular, proliferative |
| Cytologic atypia | Absent | Present |
| IHC | Not required | CD31 / von Willebrand factor to confirm endothelial origin |
Summary Points for Exam
- Most common vascular tumor in infancy/childhood = Hemangioma
- Most common type = Capillary hemangioma
- Juvenile/strawberry hemangioma → regresses by age 7 in most cases
- Cavernous hemangioma = large vascular channels, no spontaneous regression, intravascular thrombosis + dystrophic calcification
- Most common benign liver tumor = Cavernous hemangioma
- Pyogenic granuloma = capillary hemangioma variant; pedunculated; bleeds easily; post-trauma or pregnancy
- Von Hippel-Lindau disease = associated with cavernous hemangiomas (cerebellum, brainstem, retina, liver, pancreas)
- Malignant transformation is rare in all hemangiomas
Sources: Robbins & Kumar Basic Pathology (9780323790185); Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
This is a shared conversation. Sign in to Orris to start your own chat.