Explain hyperthermia malignant pathophysiology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"malignant hyperthermia"[MeSH Terms] AND pathophysiology
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have all the content needed. Here is the full answer.
Malignant Hyperthermia - Pathophysiology
Overview
Malignant hyperthermia (MH) is a pharmacogenetic clinical syndrome - a life-threatening hypermetabolic crisis of skeletal muscle triggered by a gene-environment interaction. It is not present at baseline; susceptible individuals appear phenotypically normal until exposed to a triggering agent. The disorder is fundamentally one of dysregulation of excitation-contraction coupling (ECC), driven by uncontrolled release of Ca²⁺ from the sarcoplasmic reticulum (SR).
Step 1 - Normal Excitation-Contraction Coupling (The Baseline)
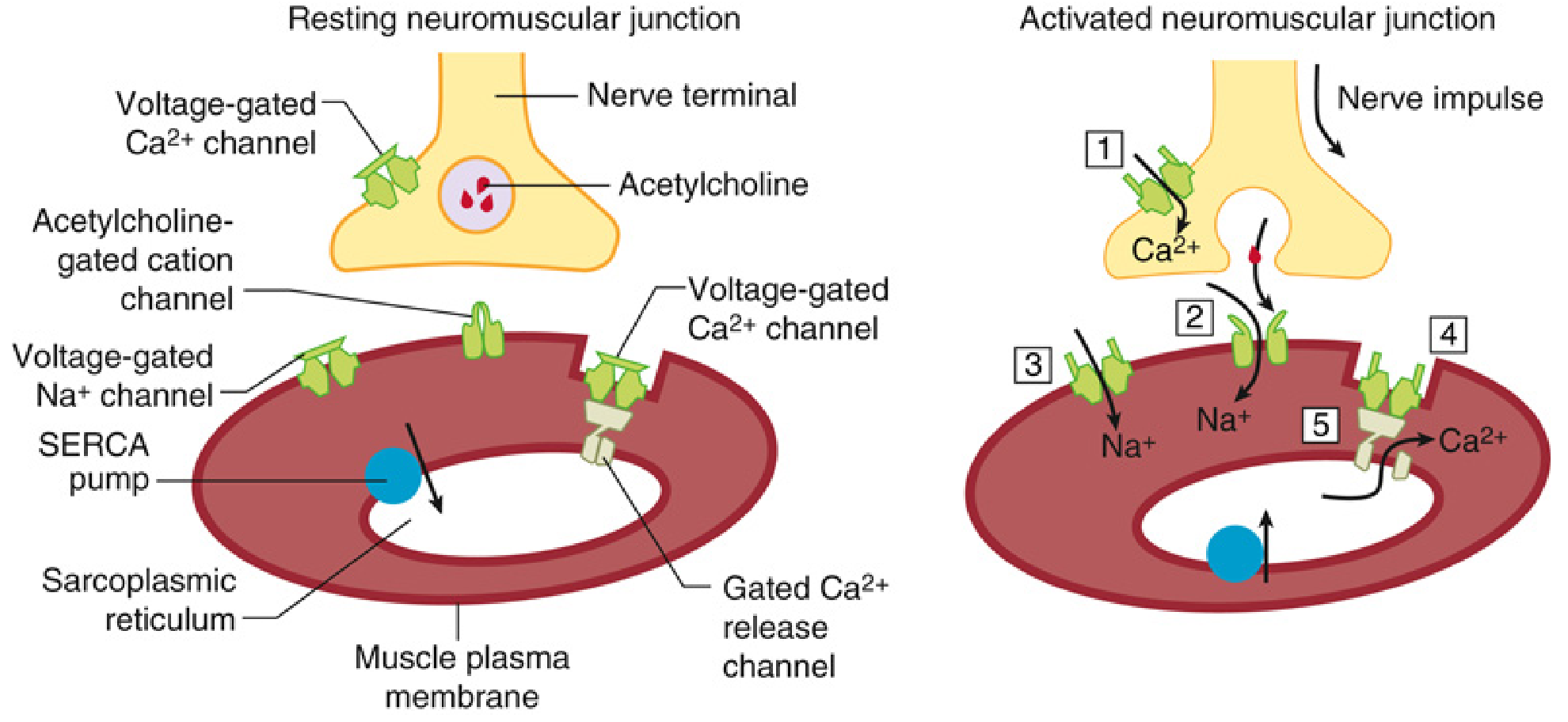
Understanding the crisis requires understanding normal ECC:
- A nerve impulse reaches the motor end plate and triggers acetylcholine (ACh) release.
- ACh binds nicotinic receptors (nAChR), depolarizing the sarcolemma.
- The action potential propagates along the sarcolemma and travels down transverse tubules (T tubules) - invaginations that form triad junctions with the SR terminal cisternae.
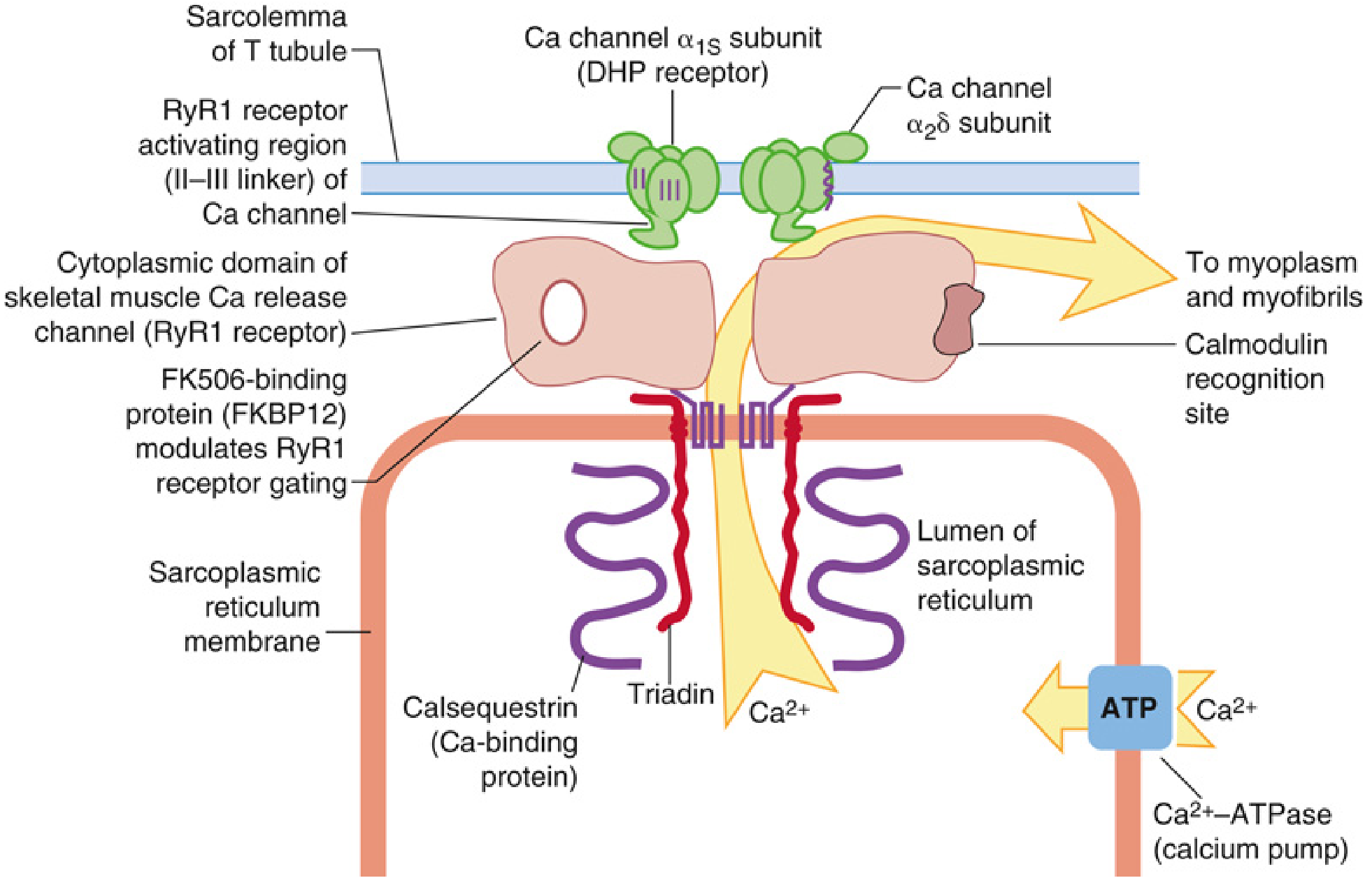
- The depolarization is sensed by Cav1.1 (the dihydropyridine receptor, DHPR) - the voltage-gated Ca²⁺ channel in the T tubule membrane.
- Cav1.1 physically communicates - via conformational change, mediated by the adaptor protein STAC3 - with the Type 1 Ryanodine Receptor (RyR1), the Ca²⁺ release channel on the SR membrane.
- RyR1 opens, releasing a large bolus of Ca²⁺ from the SR lumen into the sarcoplasm.
- Ca²⁺ binds troponin C, displaces tropomyosin, and exposes actin's myosin-binding sites → muscle contraction.
- SERCA pumps (SR Ca²⁺-ATPases) then actively re-sequester Ca²⁺ back into the SR. When sarcoplasmic Ca²⁺ drops below 10⁻⁶ M, the muscle relaxes; the resting level is restored to ~10⁻⁷ M.
Both contraction and SERCA-driven relaxation consume ATP, generating heat as a byproduct.
Step 2 - The Molecular Defect: RyR1 Mutations
The core defect in MH susceptibility is a gain-of-function mutation - most commonly in RYR1 (50-80% of cases), with a small subset (~1%) in CACNA1S (encoding Cav1.1).
RyR1 - Structure and Function
RyR1 is a homotetramer of four ~5,000 amino acid subunits, making it the largest ion channel in mammals (>2 megadaltons). It is regulated by Ca²⁺, Mg²⁺, ATP, calmodulin, FK506-binding protein (FKBP12), and signals from Cav1.1.
Pathogenic RYR1 mutations cluster in three hot-spot regions:
- Region 1 (N-terminal): amino acids 35-614
- Region 2 (Central/sarcoplasmic foot): amino acids 2129-2458
- Region 3 (C-terminal transmembrane/pore): amino acids 3916-4942
These mutations lock RyR1 in an "intermediate" pathological conformation resembling the open channel, making it aberrantly sensitive to activating signals - including volatile halogenated anesthetics (halothane, isoflurane, sevoflurane, desflurane) and succinylcholine.
Step 3 - The Triggering Event and Ca²⁺ Cascade
When a susceptible individual is exposed to a triggering agent:
- The mutant RyR1 channel opens uncontrollably - it cannot be adequately suppressed by normal inhibitory signals (Mg²⁺, calmodulin).
- Ca²⁺ floods out of the SR into the sarcoplasm in a sustained, unregulated manner.
- Sarcoplasmic Ca²⁺ rises far above the contractile threshold (10⁻⁶ M) and cannot be normalized.
Two additional mechanisms amplify this Ca²⁺ overload:
- Excitation-coupled Ca²⁺ entry (ECCE): MH mutations enhance entry of extracellular Ca²⁺ into the cell, not just release from SR stores.
- Store-operated Ca²⁺ entry (SOCE): SR Ca²⁺ depletion activates additional sarcolemmal channels to import more extracellular Ca²⁺, further worsening the crisis.
Step 4 - The Hypermetabolic Cascade
The sustained intracellular Ca²⁺ overload drives a vicious hypermetabolic cycle:
| Pathological Process | Mechanism |
|---|---|
| Sustained muscle contracture / rigidity | Ca²⁺ remains above the contractile threshold; muscle cannot relax |
| Massively increased ATP consumption | SERCA pumps work maximally trying (and failing) to re-sequester Ca²⁺; sustained actin-myosin cycling also consumes ATP |
| Heat production (hyperthermia) | ATP hydrolysis and futile Ca²⁺ cycling generate enormous heat - temperatures can rise at 1°C per 5 minutes |
| Increased O₂ consumption and CO₂ production | Aerobic and anaerobic metabolism surge to regenerate ATP; early sign is rising PaCO₂ |
| Metabolic acidosis | Lactate accumulates from anaerobic glycolysis; CO₂ retention adds a respiratory component |
| Rhabdomyolysis | Sustained Ca²⁺ activates Ca²⁺-dependent proteases (calpains), phospholipases, and eventually leads to sarcomere destruction; CK peaks on day 2-3 |
| Hyperkalemia | Massive release of intracellular K⁺ from damaged myocytes; compounded by rhabdomyolysis |
| Hypocalcemia | Ca²⁺ is sequestered into damaged cells and precipitates with phosphate from lysed muscle |
Step 5 - Systemic Complications
The downstream consequences of unchecked rhabdomyolysis and metabolic derangement:
- Acute kidney injury - from myoglobinuria (myoglobin precipitates in renal tubules, especially in an acid environment)
- Cardiac arrhythmias / arrest - from hyperkalemia, acidosis, and hyperthermia
- Disseminated intravascular coagulopathy (DIC) - released thromboplastins from lysed muscle activate the coagulation cascade
- Multi-organ failure - if not treated promptly
Genetics Summary
| Gene | Protein | % of MHS cases |
|---|---|---|
| RYR1 | Type 1 Ryanodine Receptor | 50-80% |
| CACNA1S | Cav1.1 (α1s subunit of DHPR) | ~1% |
| Unknown loci | - | ~20-50% |
Inheritance is autosomal dominant in most families (e.g., Evans myopathy), though with variable penetrance influenced by sex, age, and environmental modifiers. Males are more susceptible than females. The pediatric population accounts for ~52% of all MH reactions.
Related conditions sharing the same molecular defect include Central Core Disease (CCD) and King-Denborough Syndrome (KDS), both linked to RYR1 mutations.
Non-Anesthetic Triggers
Susceptible individuals can also develop attacks outside the OR:
- Vigorous exercise in a hot environment (exertional heat stroke variant)
- Neuroleptic agents - trigger a clinically similar syndrome (neuroleptic malignant syndrome) by raising myoplasmic Ca²⁺ via a different mechanism; occurs in ~0.2% of patients receiving neuroleptics
Why Dantrolene Works
Dantrolene acts directly on RyR1, stabilizing it in the closed conformation and reducing aberrant Ca²⁺ release from the SR. This interrupts the Ca²⁺ overload cascade at its source. Dantrolene has reduced MH mortality from ~60% to less than 1.4%.
Sources:
- Miller's Anesthesia, 10e, pp. 4525-4536 - primary molecular and pathophysiological detail
- Katzung's Basic & Clinical Pharmacology, 16e, p. 704
- Goldman-Cecil Medicine
- DiMaio's Forensic Pathology, 3e, p. 416
A recent 2024 review in Critical Care Medicine (PMID: 39171998) provides an updated clinical summary consistent with the above pathophysiology. A 2025 review in Progress in Lipid Research (PMID: 40680894) explores the emerging role of the endocannabinoid system in modulating RyR1 activity in MH - a developing area not yet incorporated into standard textbooks.
Search for recent clinical guidelines on MH diagnosis and management
Searching PubMed
"malignant hyperthermia" AND (guidelines OR management OR diagnosis)
Searching the Web
malignant hyperthermia clinical guidelines 2023 2024 2025 MHAUS EMHG diagnosis management
Finding Sources
Searching PubMed
"malignant hyperthermia" AND ("European Malignant Hyperthermia Group" OR EMHG OR dantrolene OR "clinical grading scale")
Reading Web Page
malignant hyperthermia diagnosis management guidelines dantrolene dosing
Reading Article
Reading Article
Reading Article
Finding Sources
Reading File
Reading Web Page
MH investigation susceptibility testing contracture test genetic testing 2025 EMHG guidelines
I now have all the content needed for a thorough answer. Let me compile it.
Recent Clinical Guidelines on MH Diagnosis and Management
Three major guideline documents have been published or updated in 2024-2026, representing the current international standard of care.
Key Guideline Documents (2024-2026)
| Guideline | Body | Published | Focus |
|---|---|---|---|
| Recognition and management of an MH crisis | European MH Group (EMHG) | Jan 2025 (BJA) | Acute crisis management |
| Investigation of MH susceptibility | EMHG | Feb 2026 (BJA) | Diagnostic pathways, contracture testing, genetics |
| JSA Guideline for MH management 2025 | Japanese Society of Anesthesiologists | 2025 (PMC) | Comprehensive perioperative management |
| Expert Review: MH in the ICU | Pinyavat et al., Critical Care Medicine | Dec 2024 | ICU-focused management |
Part 1 - Diagnosis
Clinical Recognition: Pattern-Based, Not Single-Sign
The 2024 EMHG guideline stresses identifying a pattern of signs rather than waiting for any single hallmark. The 2025 EMHG investigation guideline has also introduced for the first time a consensus definition of a clinical MH event.
Early signs (minutes):
- Sudden, inappropriate rise in end-tidal CO₂ (ETCO₂) - often the first sign
- Increased O₂ consumption
- Mixed metabolic and respiratory acidosis
- Tachycardia
- Profuse sweating and skin mottling
Late signs:
- Rapidly rising core temperature (can reach +1°C per 5 min)
- Severe hyperkalemia
- Muscle rigidity (may include masseter spasm after succinylcholine)
- Elevated CK and myoglobin
- Dark/cola-colored urine (myoglobinuria)
- Ventricular arrhythmias, cardiac arrest
- DIC
MH Clinical Grading Scale (CGS)
A validated scoring tool used to quantify MH likelihood. Scores are summed across six processes:
| Process | Finding | Points |
|---|---|---|
| I - Muscle Rigidity | Generalized rigidity | 15 |
| Masseter rigidity | 15 | |
| II - Myonecrosis | CK >20,000 (post-succinylcholine) | 15 |
| CK >10,000 (no succinylcholine) | 15 | |
| Cola-colored urine | 10 | |
| Myoglobin in urine >60 mg/L | 5 | |
| Serum K⁺ >6 mEq/L | 3 | |
| III - Respiratory Acidosis | PETCO₂ >55 mmHg (controlled ventilation) | 15 |
| PaCO₂ >60 mmHg (controlled ventilation) | 15 | |
| Inappropriate hypercarbia | 15 | |
| Inappropriate tachypnea | 10 | |
| IV - Temperature Increase | Rapid temperature rise | 15 |
| Perioperative temperature >38.8°C | 10 | |
| V - Cardiac Involvement | Inappropriate tachycardia | 3 |
| Ventricular tachycardia or fibrillation | 3 | |
| VI - Family History | Positive family history | 15 |
Score interpretation: <20 = almost never; 20-34 = unlikely; 35-49 = somewhat less than likely; 50-64 = somewhat greater than likely; 65-74 = very likely; ≥75 = almost certain.
(Barash Clinical Anesthesia, 9e, Table 24-9)
Differential Diagnosis
Important conditions to distinguish from MH before committing to treatment (though treatment should start empirically when probability is high):
- Inadequate anesthesia / analgesia
- Sepsis / malignant hyperpyrexia from infection
- Anaphylaxis
- Thyroid storm
- Pheochromocytoma
- Neuroleptic malignant syndrome (similar mechanism, different trigger)
- Serotonin syndrome
- Recreational drug toxicity (MDMA)
- Equipment malfunction (faulty CO₂ analyzer, rebreathing)
Confirmatory Testing (Post-Crisis)
All suspected MH reactions should be followed up at a specialized MH testing center. The 2025 EMHG investigation guideline (PMID: 41478797) comprehensively revised the diagnostic framework, introducing a new designation - the "MH genotype" - alongside the traditional contracture test classification.
In Vitro Contracture Test (IVCT) / Caffeine-Halothane Contracture Test (CHCT)
- Gold standard for confirming susceptibility
- Requires fresh skeletal muscle biopsy from a specialized center
- Muscle is exposed to caffeine and halothane; an abnormal contracture response at sub-threshold concentrations indicates susceptibility
- Classified as MHS (susceptible), MHE (equivocal), or MHN (normal)
- Must be done at an EMHG-accredited center
- A negative result does not definitively rule out MH (sensitivity is not 100%)
Genetic Testing
- Focused on RYR1 variants (identified in ~50-70% of susceptible individuals) and CACNA1S variants (<1%)
- The 2025 EMHG guideline introduces an updated curation system for classifying genetic variants by their pathogenic relevance to MH
- Negative genetic testing cannot rule out susceptibility
- Positive for a known pathogenic variant = MH genotype designation (new 2025 category)
- Important for family screening after a clinical event
Elevated resting CK
- Persistently elevated CK (>3x upper limit of normal) without other explanation should raise suspicion, particularly in patients with a family history of anesthetic deaths
Part 2 - Acute Management
Immediate Steps (First Minutes) - 2024 EMHG Protocol
The 2024 EMHG guideline (Glahn et al., Br J Anaesth 2025;134:221-223) and the 2025 JSA guideline converge on the following stepwise response:
1. Cease all triggering agents immediately
- Remove volatile anesthetics (turn off vaporizer, disconnect from machine)
- Discontinue succinylcholine if still infusing
- Notify the surgical team; complete or abort surgery as quickly and safely as possible
2. Ventilate with 100% O₂ at high flow
- Set flow rate ≥10 L/min
- Double to triple normal minute ventilation to reduce anesthetic circuit concentrations and treat CO₂ elevation
3. Declare an emergency and call for help
- Coordinated multidisciplinary team response required
- In the US: call MHAUS hotline (1-800-MH-HYPER) for real-time expert guidance
4. Switch to TIVA (Total Intravenous Anesthesia)
- Propofol-based anesthesia is safe; benzodiazepines, opioids, non-depolarizing NMBAs are also safe
5. Place activated charcoal filters (NEW in 2024 EMHG)
- Place on both inspiratory and expiratory limbs of the anesthesia breathing circuit
- Reduces residual volatile agent concentrations rapidly; now recommended as routine during suspected MH
Dantrolene - The Specific Antidote
Dantrolene stabilizes RyR1 in the closed conformation, directly blocking the aberrant Ca²⁺ release that drives the crisis.
| Parameter | EMHG 2024 / International Standard | JSA 2025 |
|---|---|---|
| Initial dose | 2-2.5 mg/kg IV | 1-2 mg/kg IV (per Japanese package insert) |
| Repeat dosing | Repeat 2-2.5 mg/kg every 10 minutes if symptoms persist | Repeat every 10 min, evaluate each time |
| Maximum dose | Up to 10 mg/kg or more if still effective; no absolute ceiling | No upper limit set; 7 mg/kg per Japanese package insert but continue if effective |
| Stop criterion | PaCO₂ <6 kPa (45 mmHg), decreasing temperature, improving rigidity | Same |
| Formulation | Dantrolene 20 mg vials dissolved in 60 mL sterile water; Ryanodex (nanosuspension, faster preparation) available | 20 mg/60 mL sterile water |
| Stock requirement | 36 vials immediately accessible + 24 additional within 1 hour (EMHG) | Flexible, institution-determined |
| Prophylactic use | NOT recommended preoperatively | NOT recommended |
Key note: A new formulation, Ryanodex (dantrolene nanosuspension), has improved solubility and allows much faster reconstitution, critical when every minute counts.
Supportive Care
| Complication | Management |
|---|---|
| Hyperthermia | Chilled IV normal saline (up to 50-60 mL/kg); surface cooling with ice packs, cooling blankets; cool peritoneal/bladder lavage in extremis; stop cooling once temperature <38°C to avoid overshoot |
| Acidosis | Hyperventilation to normalize PaCO₂; IV sodium bicarbonate if pH <7.2 |
| Hyperkalemia | Glucose-insulin therapy; calcium gluconate (to stabilize myocardium); sodium bicarbonate; avoid calcium channel blockers with dantrolene (risk of cardiac arrest) |
| Arrhythmias | Amiodarone, magnesium; beta-blockers (esmolol) for persistent tachycardia; avoid calcium channel blockers |
| Rhabdomyolysis / AKI | Aggressive IV crystalloid hydration; forced diuresis with furosemide; target urine output 1-3 mL/kg/hr to flush myoglobin from renal tubules |
| Monitoring | Arterial line for blood gas monitoring; urinary catheter; temperature probe |
Part 3 - Perioperative Management of Known MH-Susceptible Patients
(Barash Clinical Anesthesia, 9e; JSA 2025)
- Avoid all triggering agents: all volatile halogenated anesthetics (halothane, isoflurane, sevoflurane, desflurane) and succinylcholine
- Safe agents: propofol, benzodiazepines, opioids, non-depolarizing NMBAs (e.g., rocuronium, vecuronium), nitrous oxide, local anesthetics, regional/neuraxial anesthesia
- Machine preparation: remove or close vaporizers; replace all disposable circuit components; OR use activated charcoal filters on both circuit limbs (now the preferred, faster method)
- Dantrolene availability: must be on hand before starting anesthesia; do not give prophylactically (causes muscle weakness)
- Preoperative counseling: document MH susceptibility clearly; inform patient, family, and all future healthcare providers; wear MedAlert identification
Part 4 - Post-Crisis Follow-Up
- All suspected MH reactions must be reported to the North American MH Registry (NAMHR) or equivalent national registry
- Refer patient and first-degree relatives to an EMHG-accredited testing center for CHCT/IVCT and/or genetic testing
- Elevated baseline CK levels warrant workup for underlying myopathy
- The 2024 Critical Care Medicine review (PMID: 39171998) specifically highlights that increasing use of inhaled anesthetics in ICU sedation makes MH awareness critical outside the OR setting as well
Summary of What's New (2024-2026)
- Consensus definition of a clinical MH event (EMHG 2025 - first ever)
- MH genotype as a new formal diagnostic designation, separate from CHCT result
- Updated EMHG variant curation system for RYR1/CACNA1S genetic variants
- Activated charcoal filters now routinely recommended during suspected MH (not just for susceptible patients)
- Flexibility in treatment protocols based on local resources (EMHG 2024)
- Specific hyperkalemia management protocols added
- ICU MH awareness emphasized given increasing inhaled anesthetic use in ICU sedation
This is a shared conversation. Sign in to Orris to start your own chat.