Can you give me the different variants of dexamethasone suppression test and how these are used to distinguish between the differentials?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the complete answer.
Dexamethasone Suppression Test (DST) - Variants and Differential Diagnosis
The DST exploits the principle that dexamethasone - a potent synthetic glucocorticoid with ~100x the activity of cortisol - suppresses CRH and ACTH via negative feedback at hypothalamic-pituitary glucocorticoid receptors, thereby reducing endogenous cortisol. Critically, immunoassays for cortisol do not cross-react with dexamethasone, so only endogenous cortisol is measured. When this negative feedback is bypassed (by an autonomous tumor), cortisol fails to suppress.
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Schwartz's Principles of Surgery, 11th Edition
The Three Main Variants
1. Overnight 1 mg DST (Low-Dose Screening Test)
Protocol: 1 mg dexamethasone orally at 11 PM; plasma cortisol drawn at 8 AM the following morning (8-9 hours later). In children: 0.3 mg/m².
Interpretation:
| Result | Meaning |
|---|---|
| Cortisol < 1.8 µg/dL (< 50 nmol/L) | Normal suppression - Cushing syndrome essentially ruled out |
| Cortisol > 1.8 µg/dL | Abnormal - Cushing syndrome suspected (>95% sensitive) |
| Cortisol > 5 µg/dL (> 140 nmol/L) | Higher threshold; specificity rises to >95% |
Purpose: A pure screening test - does not distinguish the type of Cushing syndrome. Detects loss of the normal HPA feedback axis.
False positives (pseudo-Cushing / "escape"): depression, anxiety, alcoholism, obesity, acute illness, oral contraceptives/estrogen therapy (increase cortisol-binding globulin), medications that accelerate dexamethasone metabolism (phenytoin, phenobarbital, rifampicin), and chronic kidney disease.
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Schwartz's Principles of Surgery, 11th Edition
2. Standard 2-Day Low-Dose DST (Liddle Test - Confirmatory)
Protocol: 0.5 mg dexamethasone orally every 6 hours for 48 hours (total 2 mg over 2 days). 24-hour urine free cortisol (UFC) is collected on day 2.
Interpretation:
- UFC suppressed to < 50% of baseline → Cushing syndrome ruled out
- UFC not suppressed (≥ 50% of baseline) → Cushing syndrome confirmed
Purpose: Confirmatory test when the overnight 1 mg DST is abnormal or equivocal. More robust than the overnight test. Requires hospitalization in some centers.
A variant uses 0.25 mg instead of 0.5 mg to increase sensitivity for mild/subclinical Cushing (threshold AM cortisol > 7.6 µg/dL for positivity).
3. High-Dose DST (Differential Diagnostic Test)
This test is only applied after Cushing syndrome is confirmed - its purpose is to distinguish the etiology.
Two equivalent protocols:
- Standard: 2 mg dexamethasone every 6 hours for 48 hours (total 8 mg), with 24-hour UFC collected on day 2
- Overnight: Single dose of 8 mg at 11 PM, plasma cortisol measured at 8 AM next morning
Interpretation:
| Cause | Low-Dose DST | High-Dose DST | Plasma ACTH |
|---|---|---|---|
| Normal | Suppressed | Suppressed | Normal |
| Cushing disease (pituitary adenoma) | No suppression | Suppressed (UFC falls ≥ 50% from baseline) | Normal to elevated (15-500 pg/mL) |
| Ectopic ACTH syndrome | No suppression | No suppression | Markedly elevated (>300 pg/mL, sometimes >1000 pg/mL) |
| Adrenal tumor (ACTH-independent) | No suppression | No suppression | Suppressed (< 5-10 pg/mL) |
| Exogenous steroids | No suppression | No suppression | Suppressed |
Rationale by etiology:
-
In Cushing disease (pituitary adenoma): the adenoma retains some glucocorticoid receptor sensitivity - it has a raised set-point, not complete resistance. High doses of dexamethasone can still eventually suppress it.
-
In ectopic ACTH (e.g., small cell lung cancer, bronchial carcinoid, thymoma): the tumor secretes ACTH autonomously, completely outside pituitary control, and is not suppressible by any dose of dexamethasone.
-
In adrenal tumors: cortisol secretion is autonomous and ACTH-independent; ACTH is already suppressed by the high cortisol, and dexamethasone has no additional effect.
-
Scott-Brown's Otorhinolaryngology, Vol 1
-
Robbins, Cotran & Kumar Pathologic Basis of Disease
-
Schwartz's Principles of Surgery, 11th Edition
-
Katzung's Basic and Clinical Pharmacology, 16th Edition
Important caveat: The high-dose DST is imperfect. As noted by Scott-Brown's, 10-20% of ACTH-secreting pituitary adenomas do not suppress on high dose, and ~50% of ACTH-secreting bronchial carcinoid tumors do show some suppression, mimicking Cushing disease. Therefore, additional evidence (pituitary MRI, IPSS) is needed before concluding etiology.
4. Combined Dexamethasone-CRH Test (Pseudo-Cushing Differentiation)
Protocol: Low-dose dexamethasone 0.5 mg every 6 hours for 2 days, then CRH 1 µg/kg IV 2 hours after the last dexamethasone dose.
Interpretation:
- Plasma cortisol > 1.4 µg/dL (38 nmol/L) at 15 or 30 minutes post-CRH → true Cushing syndrome (high specificity)
- Suppressed cortisol post-CRH → pseudo-Cushing (e.g., depression, alcoholism, obesity)
Rationale: Sustained dexamethasone renders the normal pituitary temporarily unresponsive to CRH. In true Cushing disease, however, the pituitary adenoma "escapes" suppression and still responds to CRH. In pseudo-Cushing states (where the HPA axis is merely dysregulated, not truly autonomous), dexamethasone successfully silences the pituitary's CRH response.
False negatives occur in Cushing disease when the pituitary has a raised set-point for negative feedback.
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Katzung's Basic and Clinical Pharmacology, 16th Edition
Diagnostic Algorithm
The flowchart below from Tietz (7th Edition) summarizes how these tests work in sequence:
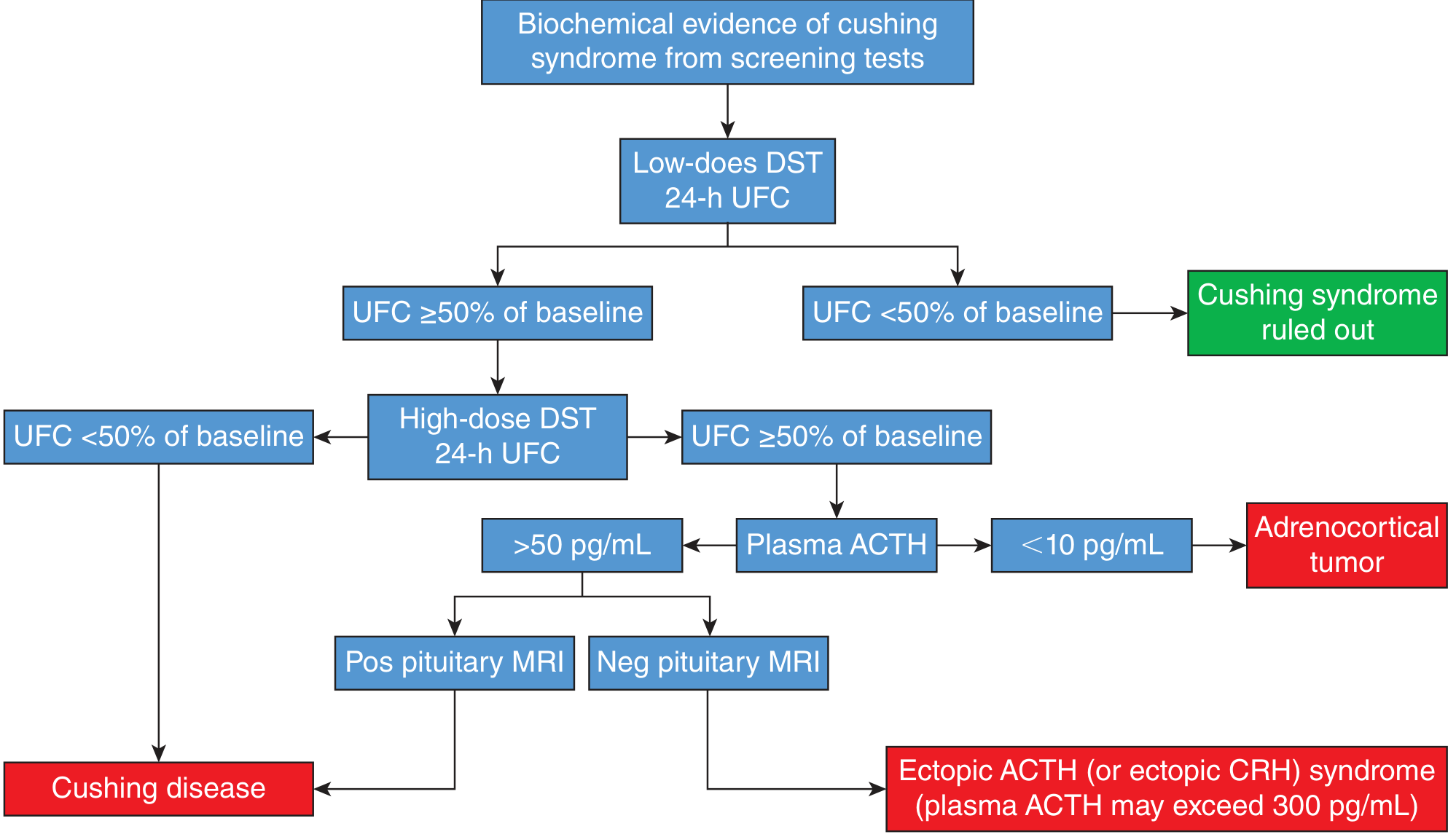
Step-by-step algorithm:
- Screening (overnight 1 mg DST + UFC): if suppressed → Cushing ruled out. If not suppressed →
- High-dose DST + UFC:
- UFC < 50% of baseline → Cushing disease (pituitary source)
- UFC ≥ 50% of baseline → measure plasma ACTH:
- ACTH < 10 pg/mL → adrenocortical tumor (primary adrenal)
- ACTH > 50 pg/mL → pituitary MRI
- Positive MRI → Cushing disease
- Negative MRI → ectopic ACTH/CRH syndrome (plasma ACTH may exceed 300 pg/mL) → consider bilateral inferior petrosal sinus sampling (BIPSS) as gold standard
Inferior Petrosal Sinus Sampling (BIPSS) - The Gold Standard
When DST results are ambiguous (especially since 10-20% of pituitary adenomas fail to suppress and some carcinoids do suppress), BIPSS provides definitive localization. CRH is administered IV, and ACTH is sampled simultaneously from both inferior petrosal sinuses and peripheral blood. A petrosal sinus to peripheral ACTH ratio > 3 after CRH stimulation is diagnostic of a pituitary microadenoma. Sensitivity rises to ~95% when combined with CRH stimulation.
Summary Table
| Test | Dose | Duration | Primary Purpose |
|---|---|---|---|
| Overnight 1 mg DST | 1 mg at 11 PM | Single dose | Screen for Cushing syndrome |
| 2-day low-dose DST | 0.5 mg q6h | 48 hours | Confirm Cushing syndrome |
| 2-day high-dose DST (Liddle) | 2 mg q6h | 48 hours | Differentiate pituitary vs. ectopic vs. adrenal |
| Overnight high-dose DST | 8 mg at 11 PM | Single dose | Differentiate (rapid alternative to Liddle) |
| Low-dose DST + CRH | 0.5 mg q6h → CRH bolus | 2 days + CRH | Distinguish true Cushing from pseudo-Cushing |
How about the midnight serum and salivary cortisol levels? Aren't those also used in screening?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I have everything needed. Here is the complete answer:
Yes, you're absolutely right - midnight cortisol measurements are one of the three first-line Endocrine Society-endorsed screening tests for Cushing syndrome, alongside the 1 mg overnight DST and 24-hour urinary free cortisol (UFC). They actually exploit a different physiological principle than the DST.
The Physiological Basis: Diurnal Variation
Cortisol secretion follows a strict circadian rhythm: it peaks around 7-8 AM (driven by ACTH surge before waking) and reaches its nadir around midnight during sleep. This nadir is a feature of normal HPA regulation.
In all forms of Cushing syndrome - pituitary, adrenal, or ectopic - the most consistent biochemical abnormality is loss of this nocturnal nadir. Notably, morning cortisol levels in Cushing patients can sometimes be within the normal range, making the midnight measurement particularly sensitive for catching early or mild disease. The key insight: even when cortisol is only mildly elevated overall, the failure to suppress at night is almost always present.
- Campbell-Walsh-Wein Urology, 3-Volume Set
Midnight Serum Cortisol
Normal: Serum cortisol falls to a trough around midnight. A single elevated midnight serum cortisol is highly suggestive of Cushing syndrome.
Cut-off values:
- In a sleeping patient (ideally inpatient): cortisol > 1.8 µg/dL is abnormal (very sensitive threshold)
- In an awake patient: cortisol > 7.5 µg/dL is used (higher threshold because wakefulness itself raises cortisol via stress)
Practical limitation: This test is clinically impractical in an outpatient setting - it requires the patient to be asleep (to avoid the stress-related cortisol surge from being awoken) and therefore usually requires inpatient admission for a reliable result. This makes it a second-line test in most algorithms, used when initial screening is abnormal or discordant.
- Campbell-Walsh-Wein Urology
- Textbook of Family Medicine, 9th Edition
Late-Night Salivary Cortisol (LNSC)
This is the practical, outpatient-friendly alternative that has become increasingly popular and is now a first-line Endocrine Society-recommended test.
Why saliva?
Salivary cortisol measures only the free (unbound) fraction of cortisol - the biologically active form. Since it is not affected by cortisol-binding globulin (CBG), it avoids the false positives seen with serum cortisol in patients on estrogens or oral contraceptives (which raise CBG, elevating total serum cortisol without true hypercortisolism). The concentration of salivary cortisol is also independent of saliva production rate.
Protocol: Patient collects saliva at home using a swab or tube at 11 PM to midnight on two separate nights (two samples required to account for variability).
Cut-off: When measured by ELISA:
- Normal: < 0.14 µg/dL (< 4 nmol/L) at midnight
- Abnormal (suggestive of Cushing): > 0.14 µg/dL on two separate occasions
Normal salivary cortisol for reference: 0.14-1.0 µg/dL at 7 AM; 0.07-0.21 µg/dL at 10 PM.
Accuracy: Reported to be similar to 24-hour UFC overall. However, false positives can occur in patients with hypertension and diabetes mellitus.
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Smith and Tanagho's General Urology, 19th Edition
How They Fit Into the Screening Algorithm
The three first-line tests are considered complementary, not interchangeable - the Endocrine Society recommends confirming an abnormal result with a second different test before proceeding to differential workup:
| Test | What it measures | Outpatient? | Main advantage | Main pitfall |
|---|---|---|---|---|
| Overnight 1 mg DST | Intact HPA feedback | Yes | Simple, single blood draw | False positives with phenytoin, estrogens, depression |
| 24-hour UFC | Total free cortisol excretion | Yes | Integrated over 24h, not affected by CBG | Insensitive in mild/subclinical disease; invalid in renal failure |
| Late-night salivary cortisol | Free cortisol at nadir | Yes (home collection) | Convenient, unaffected by CBG, good sensitivity | False positives in HTN, DM; needs two samples |
| Midnight serum cortisol | Total cortisol at nadir | No (inpatient required) | Very sensitive if done in sleeping patient | Impractical; stress of venipuncture can elevate result |
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Quick Compendium of Clinical Pathology, 5th Edition
Key Clinical Points
-
All screening tests - DST, UFC, and midnight cortisol - tell you only that Cushing syndrome is present (or absent). None of them alone distinguish the type (pituitary vs. adrenal vs. ectopic). That differentiation requires plasma ACTH and the high-dose DST as discussed previously.
-
Cyclic Cushing syndrome is an important pitfall: cortisol secretion can be intermittently normal and intermittently elevated. UFC and salivary cortisol, which must be repeated on multiple occasions, tend to catch this better than a single overnight DST.
-
Subclinical Cushing syndrome (autonomous cortisol secretion without overt clinical features, often found in adrenal incidentalomas) - the UFC is specifically not recommended by the Endocrine Society for this indication because it lacks sufficient sensitivity. The 1 mg overnight DST and LNSC are preferred for this population.
- Campbell-Walsh-Wein Urology, 3-Volume Set
- Current Surgical Therapy, 14th Edition
This is a shared conversation. Sign in to Orris to start your own chat.