Give a short note like flow chart to explain the japanese encephalitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Excellent - I now have rich, detailed information from Goldman-Cecil Medicine and Bradley-Daroff's Neurology. Let me now compile a clear flowchart-style note.
Japanese Encephalitis - Flowchart Note
1. AGENT & TRANSMISSION
Causative Agent
└── Japanese Encephalitis Virus (JEV)
├── Family: Flaviviridae, Genus: Flavivirus
└── RNA virus (same family as Dengue, Zika, West Nile)
Vector
└── Culex tritaeniorhynchus mosquito
├── Ground-dwelling; breeds in flooded rice fields
└── Peak biting: dusk to dawn (outdoors)
Transmission Cycle
Amplifying Hosts ──────────────────────────────────────────────┐
(Pigs + Wading Birds/Ducks) │
↑ ↓ │
Culex mosquito ← bites ← Pig/Bird (high viremia) │
│ │
↓ bites human (DEAD-END HOST) │
Human (low viremia - cannot amplify)
2. PATHOGENESIS
Infected Mosquito Bite
│
▼
Virus replicates in SKIN
│
▼
Spreads to Draining Lymph Nodes + Spleen
│
▼
PRIMARY VIREMIA
(usually sub-clinical - most infections stop here → asymptomatic)
│
▼ (in ~0.5% of infections)
SECONDARY VIREMIA
│
▼
End-Organ Invasion
├── Brain (thalamus, basal ganglia, midbrain, cerebellum)
└── Spinal Cord
│
▼
Apoptotic cell death + Inflammatory immune response
│
▼
ENCEPHALITIS / MENINGOENCEPHALITIS
Only 1 in 200 infections results in severe disease. The majority are asymptomatic.
3. CLINICAL SPECTRUM
Incubation Period: 6-16 days
│
▼
┌──────────────────────────────────────────────────────────────┐
│ CLINICAL SPECTRUM │
├──────────────────────────────────────────────────────────────┤
│ ASYMPTOMATIC ──── Most common (>99% of infections) │
│ │
│ MILD FEBRILE ILLNESS │
│ └── Fever, headache, nausea, vomiting, abdominal pain │
│ │
│ ASEPTIC MENINGITIS │
│ └── Meningismus without brain parenchymal involvement │
│ │
│ ENCEPHALITIS (Severe, ~0.5%) │
│ ├── Prodrome (2-4 days): Fever, headache, drowsiness │
│ ├── Excitability / Delirium │
│ ├── Seizures (common, especially in children) │
│ ├── Hyperthermia │
│ ├── Expressionless facies + Axial rigidity │
│ ├── Limb tremors + Myoclonus │
│ ├── Erratic eye movements + Cranial nerve palsies │
│ ├── Ataxia (cerebellar) │
│ ├── Limb paresis (LMN-type weakness) │
│ └── Coma → Death │
└──────────────────────────────────────────────────────────────┘
4. DIAGNOSIS
Clinical Suspicion (endemic area + encephalitis)
│
▼
┌─────────────────────────────────────────┐
│ INVESTIGATIONS │
├─────────────────────────────────────────┤
│ Blood: │
│ └── JEV-specific IgM ELISA (serum) │
│ Detectable by Day 7 of illness │
│ │
│ Lumbar Puncture (CSF): │
│ ├── Pleocytosis: 10-500 WBC/μL │
│ │ (early: PMN; late: lymphocytes) │
│ ├── Protein: 50-100 mg/dL (elevated) │
│ ├── Glucose: NORMAL │
│ └── JEV IgM ELISA in CSF │
│ Sensitivity 65-70%, Spec 90-100% │
│ │
│ MRI Brain: │
│ └── T2 hyperintensity in THALAMUS │
│ (also: basal ganglia, midbrain, │
│ cerebellum) │
│ │
│ Gold Standard: │
│ └── Plaque Reduction Neutralization │
│ Test (PRNT) │
│ OR 4-fold rise in IgG titer │
│ │
│ Early disease: │
│ └── RT-PCR (blood/CSF - detects │
│ virus before antibody appears) │
└─────────────────────────────────────────┘
5. TREATMENT
NO SPECIFIC ANTIVIRAL THERAPY AVAILABLE
(Interferon alfa-2a failed in RCT - no benefit on mortality or sequelae)
SUPPORTIVE CARE ONLY:
├── Control seizures (anticonvulsants)
├── Manage raised intracranial pressure
├── Airway and respiratory support (if comatose)
└── Prevention of secondary infections
6. PROGNOSIS
Case Fatality Rate: 20-30%
│
├── Poor prognosis: prolonged fever, seizures, coma,
│ high CNS viral load
│
└── Survivors (30-50% have long-term neurological sequelae):
├── Parkinsonism
├── Seizure disorders
├── Paresis / Paralysis
├── Cognitive impairment / Mental retardation
└── Neuropsychiatric disorders
7. PREVENTION & CONTROL
PRIMARY PREVENTION
├── VACCINATION (most effective)
│ ├── Live-attenuated vaccine
│ ├── Recommended: Children 1-15 years (endemic areas)
│ ├── Travelers: 2 doses at Day 0 and Day 28
│ └── Highly efficacious even after first dose
│
├── VECTOR CONTROL
│ ├── Larvivorous fish in breeding sites
│ ├── Outdoor fogging with malathion (outbreaks)
│ └── NOT indoor residual spray (vectors are outdoor resters)
│
└── PERSONAL PROTECTION
├── Bed nets (dusk to dawn)
├── Protective clothing (full body cover)
└── Keep pigs away from human dwellings
SECONDARY PREVENTION
├── Early diagnosis and case management
├── Sentinel surveillance at tertiary hospitals
└── Health education / community awareness
QUICK SUMMARY TABLE
| Feature | Detail |
|---|---|
| Virus | Flavivirus (RNA) |
| Vector | Culex tritaeniorhynchus |
| Amplifying hosts | Pigs + wading birds |
| Incubation | 6-16 days |
| % progressing to encephalitis | ~0.5% (1 in 200) |
| CSF glucose | Normal |
| Key MRI finding | T2 hyperintensity in thalamus |
| Diagnosis (first-line) | JEV-specific IgM ELISA (serum/CSF) |
| Treatment | Supportive only (no antiviral) |
| CFR | 20-30% |
| Neurological sequelae | 30-50% of survivors |
| Vaccine | Live-attenuated, 2-dose regimen |
Sources: Goldman-Cecil Medicine; Bradley and Daroff's Neurology in Clinical Practice; Park's Textbook of Preventive and Social Medicine
Give a note on rabies
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent - I have all the information needed plus the pathogenesis diagram. Now let me compile the full comprehensive note.
RABIES - A Comprehensive Note
1. AGENT & EPIDEMIOLOGY
| Feature | Detail |
|---|---|
| Causative Agent | Rabies virus |
| Family | Rhabdoviridae |
| Genus | Lyssavirus |
| Morphology | Bullet-shaped, single-stranded RNA virus |
| Annual Cases | ~55,000 deaths/year worldwide |
| Distribution | Endemic in Africa, Asia, Latin America, Eastern Europe |
| Main reservoir (developing world) | Domestic dog (most human cases) |
| Main reservoir (USA/developed) | Bats (most human cases) |
| Other reservoirs | Skunks, foxes, raccoons, coyotes, wolves |
2. TRANSMISSION
ANIMAL (infected) ──bite──► HUMAN
OR
──scratch──► HUMAN (if saliva contacts wound)
OR
──mucous membrane exposure──► HUMAN
OR
──organ/tissue transplant──► HUMAN (rare)
OR
──aerosol (lab/cave exposure)──► HUMAN (very rare)
❌ Human-to-human transmission is NOT documented (except organ transplant)
⚠️ Bat bites may be unrecognized (tiny puncture wounds)
3. PATHOGENESIS
The pathogenesis diagram below (from Harrison's, 22nd Ed.) summarizes the viral journey:
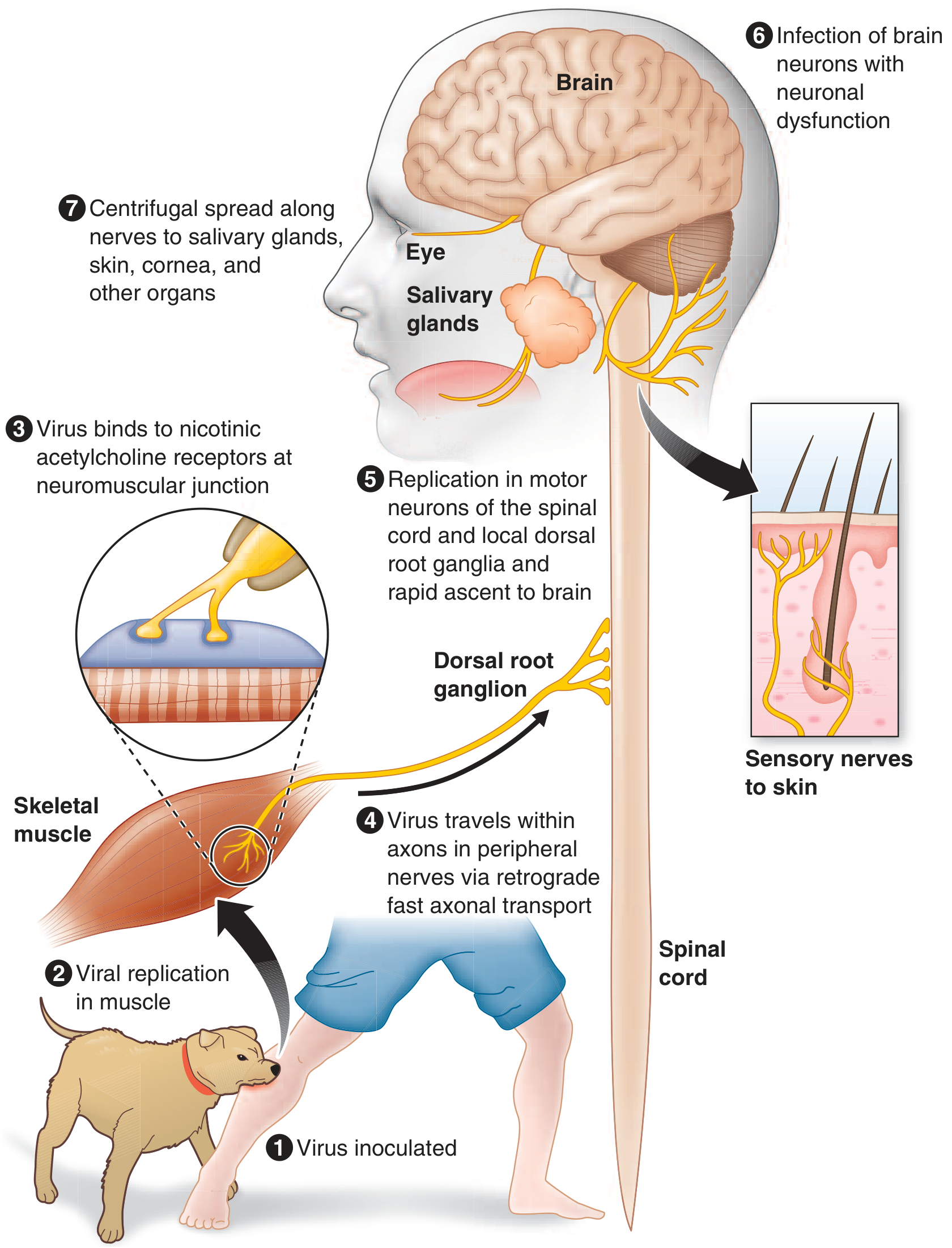
① Virus inoculated at bite site (skin/subcutaneous tissue)
│
▼
② Viral replication in MUSCLE (days to weeks, near the bite site)
│
▼
③ Virus binds nicotinic acetylcholine receptors
at neuromuscular junctions
│
▼
④ Retrograde fast axonal transport along peripheral nerves
(centripetal spread, ~250 mm/day; 12-hr delay at each synapse)
│
▼
⑤ Replication in spinal cord motor neurons +
Dorsal root ganglia → rapid ascent to brain
│
▼
⑥ Brain infection → Neuronal dysfunction
(brainstem, limbic system maximally affected)
│
▼
⑦ Centrifugal spread along autonomic/sensory nerves
→ Salivary glands, skin, cornea, heart, adrenal glands
→ Virus shed in SALIVA (enables transmission)
Key concept: The long incubation period is because the virus stays near the bite site for most of the incubation period - this is the window for effective PEP.
Pathological findings:
- Negri bodies - eosinophilic cytoplasmic inclusions in neurons (especially Purkinje cells of cerebellum and pyramidal cells of hippocampus) - pathognomonic
- Babes nodules - microglial nodules in CNS parenchyma
- Surprisingly mild degenerative neuronal changes despite fatal outcome
- Neuronal dysfunction (not death) drives clinical disease
4. CLINICAL STAGES
┌────────────────────────────────────────────────────────────────┐
│ STAGE 1: INCUBATION PERIOD │
│ Duration: Usually 20-90 days (range: days to >1 year) │
│ Symptoms: NONE │
│ Shorter with: multiple bites, facial bites, deep wounds │
└─────────────────────────┬──────────────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────────────┐
│ STAGE 2: PRODROME │
│ Duration: 2-10 days │
│ ├── Fever, malaise, headache, anorexia, nausea, vomiting │
│ ├── Anxiety / agitation │
│ └── PATHOGNOMONIC: Paresthesias, pain, or PRURITUS │
│ at/near the BITE SITE (50-80% of patients) │
│ (due to infection of dorsal root/cranial sensory ganglia) │
└─────────────────────────┬──────────────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────────────┐
│ STAGE 3: ACUTE NEUROLOGICAL PHASE │
│ │
│ TWO FORMS: │
│ │
│ A. ENCEPHALITIC / FURIOUS RABIES (~80%) │
│ ├── Agitation, hyperexcitability, combativeness │
│ ├── Hallucinations, confusion, seizures │
│ ├── Fever (may reach 105-107°F) │
│ ├── HYDROPHOBIA - involuntary painful contraction of │
│ │ pharynx/larynx/diaphragm on swallowing water │
│ │ (due to brainstem dysfunction) │
│ ├── AEROPHOBIA - same spasms triggered by a draft of air │
│ ├── "Foaming at the mouth" (hypersalivation + pharyngeal │
│ │ dysfunction) │
│ ├── Autonomic hyperactivity: │
│ │ ├── Hypersalivation, gooseflesh │
│ │ ├── Cardiac arrhythmias, priapism │
│ │ └── SIADH or Diabetes insipidus │
│ └── Episodes of lucidity between hyperexcitability │
│ (become shorter as disease progresses) │
│ │
│ B. PARALYTIC / DUMB RABIES (~20%) │
│ ├── Flaccid muscle weakness (LMN type) │
│ ├── Begins in bitten limb → spreads to quadriparesis │
│ ├── Facial weakness common │
│ ├── Sphincter involvement │
│ ├── NO hydrophobia / aerophobia │
│ ├── Mimics Guillain-Barré syndrome │
│ └── Survives a few days longer than encephalitic form │
└─────────────────────────┬──────────────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────────────┐
│ STAGE 4: COMA │
│ ├── Cardiopulmonary failure │
│ ├── Noncardiogenic pulmonary edema │
│ ├── GI hemorrhage │
│ └── DEATH (virtually 100% fatal once symptoms appear) │
└────────────────────────────────────────────────────────────────┘
5. DIAGNOSIS
CLINICAL SUSPICION
(encephalitis + animal bite history + hydrophobia/aerophobia)
│
▼
┌────────────────────────────────────────────────────────────────┐
│ INVESTIGATIONS │
├────────────────────────────────────────────────────────────────┤
│ CSF: │
│ ├── Mild mononuclear pleocytosis (<100 WBC/μL) in >50% │
│ ├── Mildly elevated protein │
│ └── Glucose: NORMAL │
│ (Severe pleocytosis >1000 → look for alternate diagnosis) │
│ │
│ Imaging (CT/MRI): │
│ ├── CT head: Usually NORMAL │
│ └── MRI: T2/FLAIR signal in brainstem, basal ganglia, │
│ thalamus, midbrain (variable; nonspecific) │
│ │
│ Specific Tests: │
│ ├── RT-PCR: saliva, CSF, skin biopsy, brain tissue │
│ ├── Skin biopsy (nape of neck): Rabies antigen in │
│ │ sensory nerve endings (immunofluorescence/ │
│ │ immunohistochemistry) │
│ ├── Serum/CSF IgM/IgG antibodies │
│ │ (not detectable until 2nd week; patient may die first) │
│ └── Brain biopsy/autopsy: Negri bodies (H&E stain); │
│ immunofluorescence (more sensitive) │
└────────────────────────────────────────────────────────────────┘
6. POST-EXPOSURE PROPHYLAXIS (PEP)
PEP is effective when started promptly BEFORE symptoms develop.
EXPOSURE OCCURS
│
▼
STEP 1: WOUND CARE (IMMEDIATE - most important first step)
├── Wash wound thoroughly with soap and water (≥15 min)
├── Apply povidone-iodine or alcohol
└── Do NOT suture primarily (if possible)
│
▼
STEP 2: ASSESS RISK (Was the animal rabid? Vaccine status?)
│
▼
STEP 3: PASSIVE IMMUNIZATION
└── Rabies Immunoglobulin (RIG)
├── Human RIG (HRIG): 20 IU/kg
└── Equine RIG (ERIG): 40 IU/kg
Inject as much as possible INTO and AROUND wound
Remainder given IM at distant site
Given ONLY on Day 0 (with 1st vaccine dose)
│
▼
STEP 4: ACTIVE IMMUNIZATION (Rabies Vaccine)
└── 4-dose regimen (post-2010):
Day 0 → Day 3 → Day 7 → Day 14
(Previously 5-dose; 4-dose is now standard)
IM into deltoid (NOT gluteal region)
⚠️ Previously vaccinated individuals:
→ Give vaccine on Day 0 and Day 3 ONLY
→ NO RIG needed
7. PRE-EXPOSURE PROPHYLAXIS (PrEP)
For: Veterinarians, animal handlers, travelers to endemic areas, lab workers
3 doses: Day 0 → Day 7 → Day 21 or Day 28
Even after PrEP, if exposed: still need 2 booster doses (Day 0 + Day 3)
NO RIG required after pre-exposure vaccination
8. TREATMENT (Once Symptomatic)
NO PROVEN SPECIFIC TREATMENT
Antiviral attempts (ribavirin, interferon-alpha): FAILED
Milwaukee Protocol (therapeutic coma): 1 survivor reported;
subsequent attempts → fatal outcome
Management = PALLIATIVE / SUPPORTIVE CARE only:
├── Seizure control
├── Sedation for agitation
├── Airway management
├── Cardiovascular support
└── Minimize patient suffering
9. PREVENTION (Public Health)
├── DOG VACCINATION (mass campaigns) - single most effective measure
├── Animal bite surveillance and stray dog control
├── Pre-exposure vaccination of high-risk groups
├── Post-exposure prophylaxis for ALL exposures
├── Public health education: seek care after animal bites
└── Avoid handling wild animals / bats
QUICK REFERENCE SUMMARY
| Feature | Key Point |
|---|---|
| Virus | Lyssavirus (Rhabdoviridae), RNA, bullet-shaped |
| Transmission | Bite/scratch/mucous membrane (mainly dog, bat) |
| Incubation | 20-90 days (up to 1 year+) |
| Pathognomonic prodrome sign | Pain/pruritus at bite site |
| Pathognomonic brain finding | Negri bodies |
| Clinical forms | Furious (80%) vs Paralytic (20%) |
| Hallmark clinical signs | Hydrophobia, aerophobia |
| Paralytic rabies mimics | Guillain-Barré syndrome |
| CSF glucose | Normal |
| MRI | T2 signal in brainstem / basal ganglia |
| Best diagnostic test | RT-PCR (saliva/CSF) + skin biopsy (nape) |
| Treatment | Supportive only - virtually 100% fatal |
| PEP vaccine doses | 4 doses: Day 0, 3, 7, 14 |
| RIG dose (human) | 20 IU/kg |
| Mortality once symptomatic | ~100% |
Sources: Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.