
Give short note on this topic, make point-wise answer giving sub-topic, don't make too much long answer, don't give too much short answer. Also add some additional point if it is missing here.
sclerotic dentin definition mechanism clinical significance dentistry
SCLEROTIC DENTIN
1. Definition
- Also called transparent dentin or dentinal sclerosis
- A type of protective/defensive dentin (not reparative) formed in response to stimuli such as caries, attrition, abrasion, erosion, and aging
2. Mechanism of Formation
- Stimuli (caries, wear, aging) trigger a protective response in odontoblasts
- Apatite crystals are deposited into the dentinal tubules, causing peritubular dentin mineralization
- The tubule lumen is gradually obliterated (occluded), making dentin less permeable
- The source of calcium is believed to be the dental lymph (fluid) within the tubules
3. Types
- Physiologic sclerosis - occurs as part of normal aging; begins after adolescence
- Pathologic sclerosis - occurs under carious lesions, attrition, abrasion, or non-carious cervical lesions (NCCL)
4. Microscopic / Optical Features
- Transmitted light - appears transparent/translucent (tubules filled with mineral have same refractive index as surrounding dentin)
- Reflected light - appears dark
- More radiopaque than normal dentin (due to increased mineralization)
- More commonly seen in older individuals (elderly)
5. Clinical Significance
- Reduced permeability - blocks the pathway for bacterial toxins and irritants, thus protecting the pulp and prolonging pulp vitality
- Harder than normal dentin - sclerotic dentin under carious lesions is harder and more highly calcified than adjacent normal dentin
- Slows caries progression - the mineral barrier reduces advancement of carious lesions
- Resistant to acid etching - the hypermineralized surface layer resists phosphoric acid, so penetration of dentin adhesives is limited and bonding is compromised
- Bonding challenge - mineralized casts occlude tubules, preventing resin tag formation; requires additional conditioning (e.g., phosphoric acid pre-etching, air abrasion) for better adhesive bond strength
6. Additional Points
- Not the same as root translucency - age-related root translucency (apical end) is a separate phenomenon used in forensic age estimation; sclerotic dentin in the crown is due to pathological stimuli
- Surface hypermineralized zone - in NCCL, a thick surface layer of hypermineralized dentin further impairs adhesive penetration
- Self-etch adhesives perform poorly on sclerotic dentin compared to total-etch systems due to the dense mineral layer
- MDP-containing adhesives (10-methacryloyloxydecyl dihydrogen phosphate) may provide better chemical bonding to the mineral component of sclerotic dentin
In short: Sclerotic dentin is a mineralization-based defense mechanism that seals dentinal tubules, reduces permeability, protects the pulp, and slows caries - but it poses a clinical challenge for adhesive dentistry due to its resistance to etching and poor resin tag formation.
can you please make a bit more short answer, short sentence, don't make too much long, long sentence.
SCLEROTIC DENTIN
1. Definition
- Also called transparent dentin or dentinal sclerosis
- A protective response of dentin to stimuli (caries, abrasion, aging)
- Tubules become obliterated by mineral deposits
2. Mechanism
- Stimuli trigger odontoblasts to deposit apatite crystals into tubules
- Tubule lumen gradually occluded → dentin becomes less permeable
- Calcium source = dental lymph within tubules
3. Types
- Physiologic - due to normal aging
- Pathologic - due to caries, attrition, abrasion, NCCL
4. Microscopic Features
- Transmitted light → appears transparent
- Reflected light → appears dark
- More radiopaque than normal dentin
- Common in elderly
5. Clinical Significance
- Reduces permeability → protects pulp, prolongs pulp vitality
- Harder than normal dentin
- Slows caries progression
- Resistant to acid etching → limits adhesive penetration
- Poor resin tag formation → weak bonding
- Needs extra conditioning (phosphoric acid / air abrasion) for better bond
6. Extra Points
- Different from root translucency (forensic aging sign)
- MDP-containing adhesives bond better chemically to sclerotic dentin
- Self-etch adhesives perform poorly compared to total-etch systems
Give me proper sketch diagram, color diagram.
A detailed color diagram of sclerotic dentin (dentinal sclerosis) for dental students. Show a cross-section of a tooth with: 1. Left side labeled "NORMAL DENTIN" - showing open dentinal tubules with odontoblastic processes inside, pulp chamber on the left, enamel on the right, tubules are hollow/open, light pink dentin background 2. Right side labeled "SCLEROTIC DENTIN" - showing the same tubules but filled/obliterated with apatite crystals (shown as dark brown/orange mineral deposits), tubule lumen completely blocked 3. A zoomed inset circle showing a close-up of: one open normal tubule vs one obliterated sclerotic tubule side by side, with labels "Open tubule lumen", "Odontoblastic process", "Peritubular dentin", "Apatite crystal deposits (obliterated lumen)" 4. Arrows showing the progression: Stimuli (caries/abrasion/aging) → Apatite crystal deposition → Tubule obliteration → Less permeable dentin 5. Bottom section showing clinical significance labels: "Transparent in transmitted light", "Dark in reflected light", "Reduced permeability", "Protects pulp" 6. Color coding: normal dentin in light yellow, sclerotic dentin in amber/dark orange, crystals in bright white/gold, pulp in pink, enamel in light blue 7. Clean, professional medical textbook style illustration with clear labels and arrows, white background
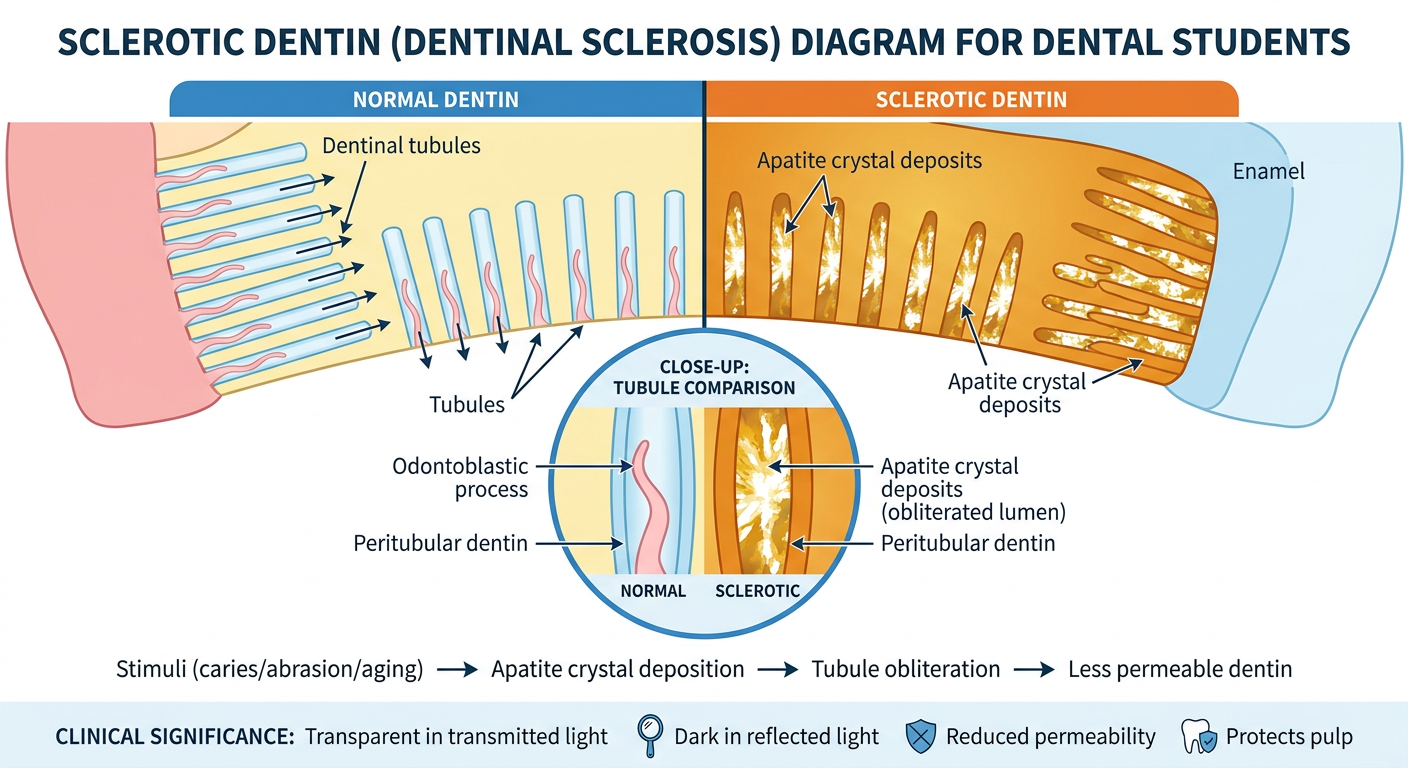
- Left side - Normal dentin with open tubule lumens and odontoblastic processes
- Right side - Sclerotic dentin with tubules obliterated by apatite crystal deposits (amber/dark color)
- Zoomed inset - Close-up comparison of open vs occluded tubule
- Progression arrows - Stimuli → Crystal deposition → Obliteration → Reduced permeability
- Bottom labels - Key clinical features (transparent in transmitted light, dark in reflected light, protects pulp)
No, no, hand diagram, sketch hand diagram, and colors will be also of hand, like notewise diagram.
A hand-drawn sketch style diagram of sclerotic dentin, like a medical student's handwritten notes on white paper. The style should look like it was drawn with colored pens and markers by hand - rough edges, hand lettering, imperfect lines, just like real student notes. Content to include: 1. Title at top in large hand-written bold text: "SCLEROTIC DENTIN" underlined with a red marker 2. Left box sketch labeled "NORMAL DENTIN" - hand drawn parallel lines (tubules) going vertically, small dots inside tubes representing odontoblastic processes, labeled with handwritten arrows: "open tubule lumen", "odontoblastic process" 3. Right box sketch labeled "SCLEROTIC DENTIN" - same parallel tubes but filled in solid with orange/brown hatching, cross-hatched filling showing mineral obliteration, arrow label: "apatite crystals fill tubule", "obliterated lumen" 4. A curved hand-drawn arrow between the two boxes pointing right, labeled "Stimuli (caries/abrasion/aging)" 5. Below, a small tooth cross-section sketch showing: enamel (blue hatching), dentin (yellow), pulp (pink), with a small region shaded in orange labeled "sclerotic zone" 6. Handwritten bullet points at bottom with colored pens: - "Transparent in transmitted light" (blue pen) - "Dark in reflected light" (black pen) - "Reduces permeability → protects pulp" (green pen) - "Resistant to acid etching" (red pen) - "Common in elderly" (purple pen) 7. Overall look: college notebook style, hand-drawn, warm white/cream paper background, colored ink markers (blue, red, green, black, orange), slightly messy but clear and educational
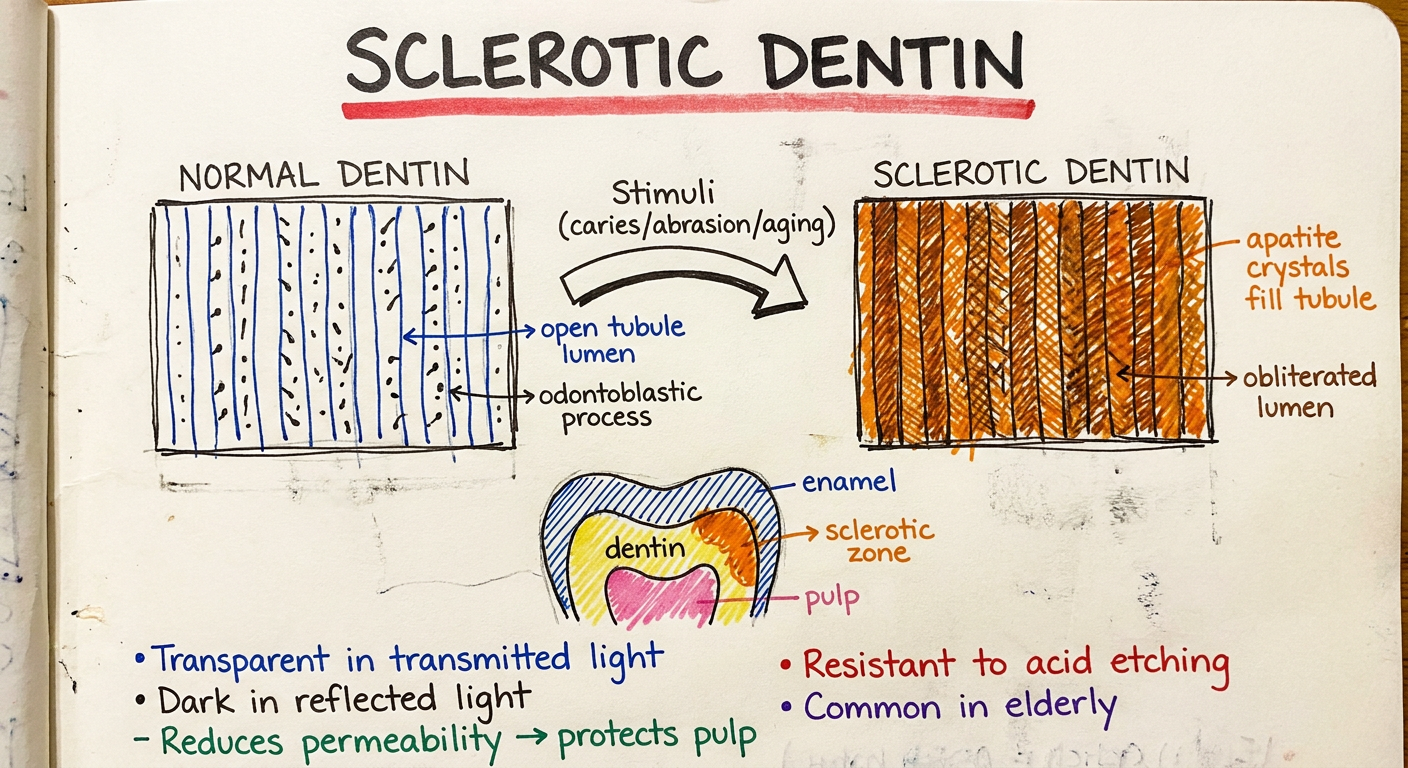
- Normal vs Sclerotic tubules side by side with hand-drawn lines and hatching
- Colored marker labels - red, blue, green, black, orange
- Tooth cross-section sketch with enamel, dentin, pulp, and sclerotic zone
- Handwritten bullet points for clinical significance at the bottom
- College notebook style - rough lines, colored ink, cream paper feel