Vagus nerve detail discuss
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full detailed answer.
The Vagus Nerve (Cranial Nerve X) - Detailed Overview
1. Etymology and Overview
The vagus nerve takes its name from the Latin word "vagi" meaning "roaming" or "wandering," reflecting its remarkable course from the cranium all the way to the abdomen. It is the 10th cranial nerve (CN X), the longest cranial nerve in the body, and the nerve of the fourth branchial arch. It is a mixed nerve carrying four types of fibers:
| Fiber Type | Function |
|---|---|
| General somatic afferent | Sensation from external ear/meatus (via Arnold's nerve) |
| General visceral afferent | Sensation from thoracic and abdominal viscera (>50% of all fibers) |
| Branchial (special visceral) efferent | Motor to striated muscles of palate, pharynx, larynx, upper esophagus |
| General visceral efferent (parasympathetic) | Preganglionic parasympathetic to thoracic and abdominal organs |
Key fact: More than half of all vagal fibers are sensory (afferent), making it primarily a sensory nerve in terms of fiber composition.
2. Nuclei (Central Connections)
The vagus nerve has four associated nuclei in the medulla oblongata:
Motor Nuclei
- Dorsal motor nucleus of the vagus (DMV): Located on the floor of the fourth ventricle, lateral to the hypoglossal nucleus. Gives rise to preganglionic parasympathetic fibers innervating the pharynx, esophagus, trachea, bronchi, lungs, heart, stomach, small intestine, ascending and transverse colon, liver, and pancreas.
- Nucleus ambiguus: Located in the reticular formation of the medulla, medial to the spinal tract of CN V. Provides branchial motor fibers to all striated musculature of the soft palate, pharynx, and larynx - except tensor veli palatini (CN V) and stylopharyngeus (CN IX). The caudal fibers of the nucleus ambiguus also travel through the cranial root of the accessory nerve (CN XI) and join the vagus to provide motor innervation to all visceral striated muscle.
Sensory Nuclei
- Nucleus solitarius (NTS): Receives taste fibers (from epiglottis, hard/soft palate, pharynx) and general visceral afferents from the nodose ganglion. Afferents from the NTS project widely to the nucleus ambiguus and dorsal motor nucleus, influencing motor output.
- Spinal (descending) nucleus of the trigeminal nerve: Receives exteroceptive sensation from the concha of the ear (carried by the jugular ganglion of CN X).
Cortical control: Motor centers for vagal function are in the lower precentral gyri, with supranuclear innervation predominantly crossed but bilateral - which is why unilateral hemispheric lesions rarely cause vagal dysfunction.
3. Ganglia
The vagus nerve bears two sensory ganglia:
| Ganglion | Location | Cell Bodies For |
|---|---|---|
| Superior (jugular) ganglion | Just inferior to jugular foramen | Afferent fibers of the meningeal and auricular branches; exteroceptive sensation from the ear |
| Inferior (nodose) ganglion | Lower in the neck | Taste from epiglottis, palates, pharynx; general visceral afferents from thoracic/abdominal organs |
4. Course and Branches
Origin
The vagus exits the lateral medulla as multiple rootlets between the olive and inferior cerebellar peduncle, converging into a single trunk that exits the skull through the middle compartment of the jugular foramen alongside CN IX and CN XI.
In the Neck
The vagus runs posteriorly within the carotid sheath, between and posterior to the internal jugular vein (IJV) and common carotid artery. Branches given off in the neck:
1. Auricular branch (Arnold's nerve)
Passes between the mastoid and tympanic plate; provides sensory supply to the tympanic membrane, skin of the posterior pinna, and posterior ear canal. Stimulating this branch (e.g., ear syringing) can trigger cough or even vasovagal syncope. It is a mechanism for referred otalgia from laryngeal/pharyngeal pathology.
2. Meningeal branch
Cell bodies in the superior (jugular) ganglion; supplies the dura mater of the posterior cranial fossa.
3. Carotid body branches
Small branches supplementing glossopharyngeal nerve supply to the carotid body chemoreceptors.
4. Pharyngeal branch
These fibers actually derive from spinal accessory fibers that join the vagus before branching off as the pharyngeal branch. They cross the internal carotid artery to join the pharyngeal plexus, providing motor innervation to the pharyngeal constrictors and soft palate (in combination with CN IX and sympathetic trunk).
5. Superior laryngeal nerve (SLN)
Given off high in the neck; passes inferior to the internal carotid artery and then travels anteroinferiorly. At the level of the hyoid it divides into:
- Internal laryngeal nerve: Pierces the thyrohyoid membrane superior to the superior laryngeal artery. Provides sensory innervation to the laryngeal and piriform fossa mucosa above the vocal folds, with some motor contribution to the interarytenoid muscle plus motor and sensory supply to the cervical esophagus and trachea.
- External laryngeal nerve: Much smaller; runs with the superior thyroid artery along the sidewall of the inferior constrictor before piercing it to supply motor innervation to the cricothyroid muscle - the only intrinsic laryngeal muscle not supplied by the recurrent laryngeal nerve. A normal variant called the communicating nerve (~45% of individuals) provides additional thyroarytenoid motor supply and subglottic sensory supply.
6. Cardiac branches (cervical)
Leave the vagus low in the neck to contribute to the cardiac plexus, providing parasympathetic slowing to the heart (negative chronotropy and dromotropy).
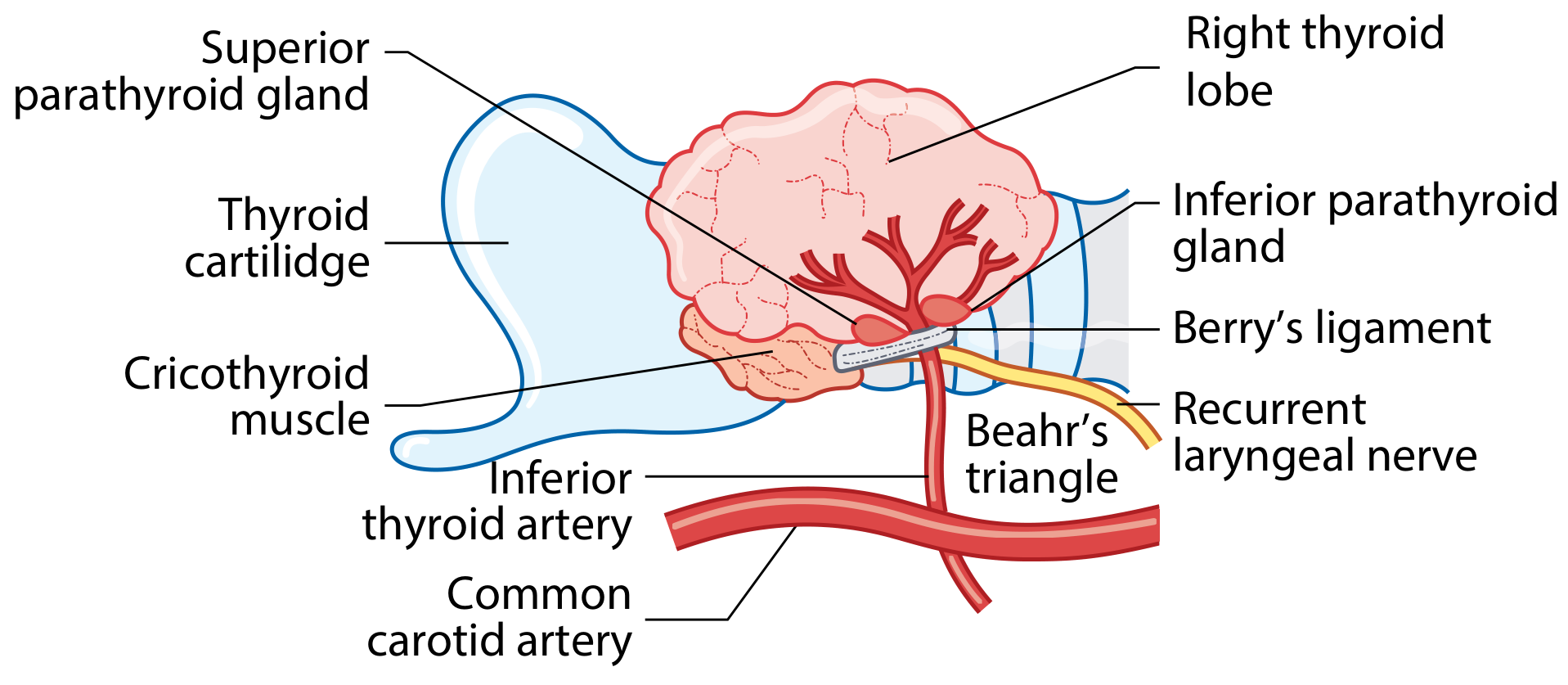
7. Recurrent laryngeal nerve (RLN)
The course is asymmetric due to embryological development (nerve of the 6th branchial arch):
- Right RLN: Has a more variable path but usually hooks around the right subclavian artery before ascending medially toward the tracheoesophageal groove. In ~1% of individuals it takes a non-recurrent course (a clinically important surgical variant). The relationship to the inferior thyroid artery is variable (may run deep, superficial, or between branches).
- Left RLN: Leaves the vagus in the lower neck/thorax, loops around the ligamentum arteriosum and arch of the aorta, then ascends in the tracheoesophageal groove back into the neck.
Both RLNs provide motor innervation to all intrinsic laryngeal muscles except cricothyroid and sensory supply to laryngeal mucosa below the vocal folds. The Beahr's triangle (common carotid artery laterally, inferior thyroid vessels and RLN) is the key surgical landmark for identifying the nerve during thyroidectomy.
In the Thorax
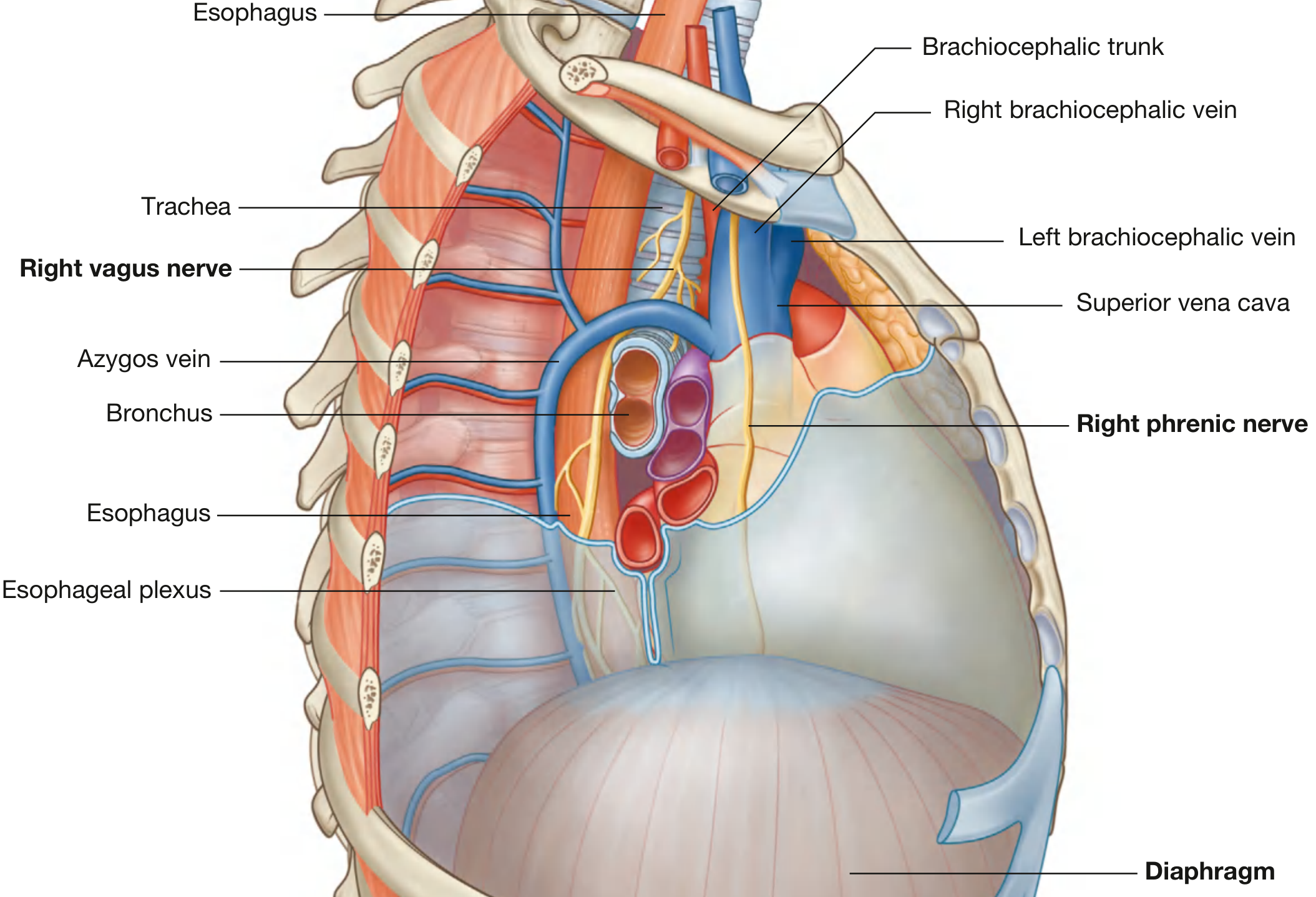
Right vagus: Enters the superior mediastinum between the right brachiocephalic vein and the brachiocephalic trunk. Descends posteriorly toward the trachea, crosses its lateral surface, is crossed by the arch of the azygos vein, then passes posterior to the root of the right lung to reach the esophagus.
Left vagus: Enters posterior to the left brachiocephalic vein, between the left common carotid and subclavian arteries. Crosses the left side of the arch of the aorta, gives off the left recurrent laryngeal nerve at the inferior margin of the arch (lateral to the ligamentum arteriosum), then passes posterior to the root of the left lung.
In the posterior mediastinum, both vagus nerves give off branches to the:
- Cardiac plexus
- Pulmonary plexus (around the lung roots)
- Esophageal plexus (both nerves intertwine forming plexuses around the esophagus)
In the Abdomen
The esophageal plexus reconstitutes into anterior and posterior vagal trunks as the esophagus passes through the esophageal hiatus:
- Left vagus → anterior vagal trunk (in front of esophagus)
- Right vagus → posterior vagal trunk (behind esophagus)
Anterior vagal trunk divides into: hepatic branch, gastric branches, pyloric branches, and celiac branches.
Posterior vagal trunk gives off branches to the celiac plexus and gastric branches.
The vagal sensory neurons innervate the GI tract up to the right (splenic) flexure of the colon - beyond which parasympathetic innervation comes from the pelvic splanchnic nerves (S2-S4).
5. Parasympathetic Functions (Summary by Organ)
| Organ | Vagal Effect |
|---|---|
| Heart | Decreases rate (negative chronotropy), slows AV conduction |
| Lungs | Bronchoconstriction, increases secretions |
| Esophagus | Promotes peristalsis |
| Stomach | Stimulates secretion (HCl, pepsin), promotes motility |
| Small intestine | Increases motility and secretions |
| Large intestine (to splenic flexure) | Increases motility |
| Liver/Gallbladder | Stimulates bile secretion |
| Pancreas | Stimulates enzyme and insulin secretion |
6. Sensory/Afferent Functions
Visceral afferents relay information on normal physiological processes and reflex activities - they do not transmit pain sensation directly. Key afferent roles:
- Satiety regulation: Vagal afferents in the gut respond to cholecystokinin (CCK) released by duodenal enteroendocrine cells post-meal, activating CCK-A receptors on vagal afferents to reduce meal size and initiate satiation.
- Metabolic regulation: Vagal afferents are important regulators of energy balance, appetite, and liver gluconeogenesis; alterations are observed in obesity.
- Aortic baroreceptors: Vagal afferents from the aortic arch contribute to blood pressure regulation.
- Cough reflex: Afferents from the larynx, trachea, and bronchi mediate the cough reflex.
- The sensory cell bodies reside in the nodose ganglion and project centrally to the NTS in the medulla.
7. Clinical Evaluation
Testing Vagal Function
- Soft palate/uvula: At rest and with phonation - should elevate symmetrically; uvula should remain midline.
- Gag reflex: Afferent = CN IX; efferent = CN IX + CN X.
- Voice quality: Hoarseness, "nasal twang," or weak voice suggests vagal dysfunction.
- Swallowing: Dysphagia, particularly with liquids diverted nasally, suggests palatal/pharyngeal weakness.
8. Clinical Lesions and Syndromes
Unilateral Vagal Palsy
- Ipsilateral palatal flattening; on phonation, ipsilateral palate fails to elevate, uvula deviates to the contralateral (normal) side
- Dysphagia and dysarthria ("nasal twang")
- Ipsilateral vocal cord assumes the cadaveric position (midway between adduction and abduction)
- Hoarseness; impaired voluntary cough (but little dyspnea)
- Ipsilateral gag reflex depression (efferent arc interrupted)
Bilateral Vagal Palsy
- Bilateral palatal droop; profound dysphagia (worse for liquids, which enter the nasal cavity)
- Severely hoarse, weak voice; ineffective cough; significant respiratory compromise
Supranuclear Lesions
- Unilateral hemispheric lesions rarely cause vagal dysfunction (bilateral cortical innervation)
- Pseudobulbar palsy with bilateral UMN lesions: spastic dysarthria, dysphagia, emotional lability, exaggerated gag
Nuclear/Brainstem Lesions
- Wallenberg syndrome (lateral medullary ischemia): Affects nucleus ambiguus - dysphagia, hoarseness, decreased gag reflex, ipsilateral facial sensory loss, limb ataxia, ipsilateral Horner syndrome, contralateral body pain/temperature loss (spinothalamic tract), and vertigo
- Palatopharyngeal paralysis of Avellis: Only the rostral nucleus ambiguus is injured - laryngeal function spared, only palatal/pharyngeal paralysis
- Other causes: syringobulbia, motor neuron disease, demyelination, tumors
Peripheral Lesions
- Recurrent laryngeal nerve injury: Most commonly from thyroid surgery, esophageal surgery, or mediastinal pathology (lung cancer, lymphoma, aortic aneurysm - especially for the left RLN). Results in unilateral or bilateral vocal cord paralysis.
- Superior laryngeal nerve injury: Seen in high neck dissections, carotid endarterectomy; loss of cricothyroid function alters voice pitch and projection.
- Jugular foramen lesions (tumors, thrombosis): May affect CN IX, X, and XI together (Vernet's syndrome).
- Herpes zoster, paragangliomas, neoplasms: Can affect peripheral vagal branches.
- Parkinson's disease: Peripheral involvement especially of the superior laryngeal nerve contributes to dysphagia.
9. Vagus Nerve Stimulation (VNS)
VNS is a neurostimulation technique with proven therapeutic roles:
- Epilepsy: FDA-approved (1997) for refractory focal-onset seizures in patients ≥12 years. Reduces seizure frequency by ~24-28% short-term, rising to ~52% reduction at 12 years. Seizure freedom achieved in <10% of patients. The mechanism involves approximately 80% of vagal fibers being afferent, projecting to the NTS with widespread central projections; VNS increases thalamic blood flow (correlating with seizure control) and reduces amygdala/hippocampal perfusion.
- Depression: FDA-approved for chronic/recurrent depression unresponsive to antidepressants.
- Device: A generator implanted under the left clavicle; electrodes wrap around the left vagus nerve in the neck. Standard settings: 30 seconds ON / 5 minutes OFF; titrated by current intensity (steps of 0.25 mA). A magnet allows on-demand stimulation to abort seizures. Newer models offer responsive stimulation based on ictal tachycardia detection.
10. Key Surgical Points
- The vagus lies posteriorly within the carotid sheath, between the IJV and common carotid - inadvertent inclusion in mass ligations during neck surgery can cause vagal injury.
- Beahr's triangle (carotid artery laterally, inferior thyroid vessels and RLN) is the key landmark for safe thyroid surgery.
- The right non-recurrent laryngeal nerve (~1% of individuals) arises directly from the vagus in the neck and can be transected if not anticipated during thyroid surgery.
- Left RLN is particularly vulnerable to mediastinal pathology - a left RLN palsy without prior surgery warrants chest imaging to exclude lung cancer, aortic aneurysm, or mediastinal lymphadenopathy.
Sources:
- Localization in Clinical Neurology, 8e - Anatomy of Cranial Nerve X and Clinical Evaluation, pp. 867-869
- Bradley and Daroff's Neurology in Clinical Practice - Vagus Nerve Anatomy and VNS, pp. 2283
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Vagus Nerve, p. 602
- Gray's Anatomy for Students - Right and Left Vagus Nerves, pp. 260-262
- Fischer's Mastery of Surgery, 8e - Surgical Anatomy of Vagus Nerve
- Yamada's Textbook of Gastroenterology, 7e - Vagal afferents and energy regulation, p. 563
This is a shared conversation. Sign in to Orris to start your own chat.