Technique of fascial closure in midline laparotomy.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"midline laparotomy" AND "fascial closure" AND "incisional hernia"
Finding Sources
Finding Sources
Reading File
Reading Article
PMID: 40354104
Reading Article
PMID: 41761330
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have all the information needed for a thorough answer. Let me compile it.
Fascial Closure in Midline Laparotomy
Fischer's Mastery of Surgery, 8th ed.
Anatomical Considerations
The midline incision divides the linea alba - the avascular fibrous fusion of the bilateral anterior and posterior rectus sheaths. When closing, the primary goal is to approximate only the linea alba (fascia/aponeurosis) without incorporating fat or muscle in each stitch.
The oblique abdominal muscles generate forces perpendicular to the healing linea alba, making it biomechanically vulnerable. Long-term incisional hernia rates exceed 20% after midline laparotomy.
Key principle: Fatty and muscular tissues incorporated in a stitch become ischemic under suture tension, undergo necrosis, create suture slack, and allow fascial edge separation - the primary mechanism of hernia formation.
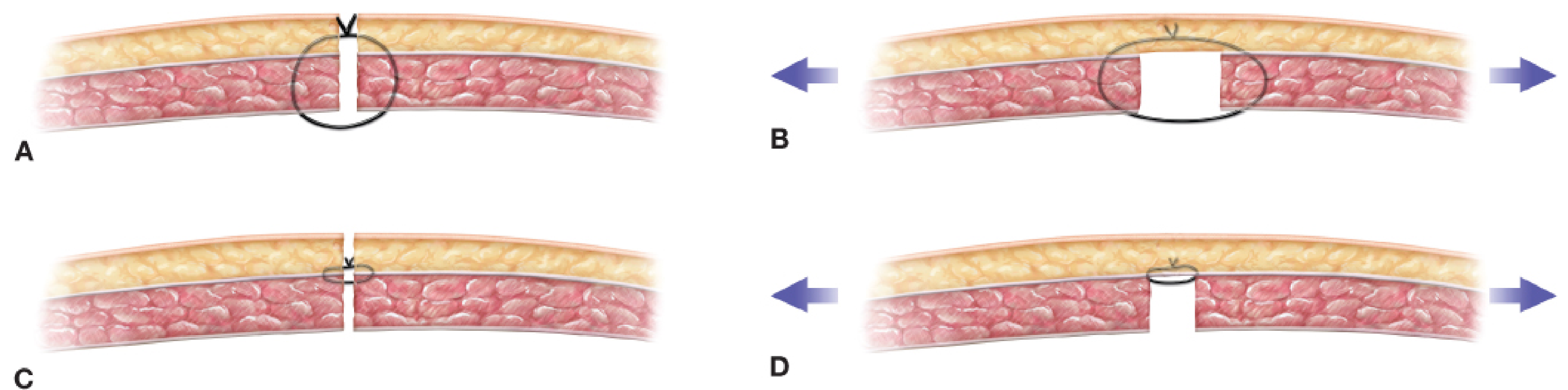
Large tissue bites incorporating fat and muscle (A) lead to suture slack and fascial gaps (B) as tissues necrose. Small bites of only fascia (C) result in minimal necrosis and maintained apposition (D).
Layers Closed (and Not Closed)
| Layer | Action | Rationale |
|---|---|---|
| Peritoneum | Not closed separately | Adds no strength; unnecessary |
| Linea alba (fascia) | Closed - primary layer | Only layer that matters for strength |
| Subcutaneous fat / Scarpa fascia | Closed with antimicrobial suture in obese patients | Reduces SSI in high-BMI patients; does not affect hernia rate |
| Skin | Closed as appropriate; NPWT or delayed closure in septic/contaminated wounds | Wound infection increases hernia risk |
Drains and ostomies should never exit through the midline incision, as they predispose to infection and weaken the closure.
Suture Material
Type
A synthetic monofilament slowly absorbable suture is the evidence-based choice:
- Monofilament sutures are acapillary - they do not wick bacteria, unlike braided multifilament sutures.
- Slow absorption (e.g., polydioxanone/PDS, Maxon, Monoplus) is essential because fascial healing takes over a year; these sutures retain >50% tensile strength at 6 weeks and absorb after 6-8 months.
- Fast absorbable sutures (e.g., Vicryl) retain only 25% strength at 4 weeks - the fascia has not healed sufficiently, risking dehiscence, evisceration, and hernia.
- Nonabsorbable sutures (polypropylene, polyester) remain an option but carry risk of long-term suture sinuses and infection.
Gauge
USP 2-0 on a small (20-mm) taper-tip needle (SH needle) for small-bite technique. The small needle arc helps restrict each bite to fascia only.
Suturing Technique
Continuous vs. Interrupted
- Continuous suture is the standard for elective midline closure - faster, fewer knots, less foreign material.
- Interrupted suture may be preferred in: thin/frail fascia, closure under tension, or emergency laparotomy settings - failure of one suture does not cause failure of the entire line. A 2026 meta-analysis (25 RCTs, n=3,548) found interrupted closure significantly reduced wound dehiscence (RR 0.47) and shortened hospital stay in emergency laparotomy. [PMID 41761330]
- Retention sutures have largely been abandoned - little evidence supports their use.
The Small Bite Technique (Evidence-Based Gold Standard)
The cornerstone of modern fascial closure is the small bite technique achieving a Suture Length : Wound Length (SL:WL) ratio >4.
The SL:WL Ratio
Each stitch should be placed:
- 5-8 mm back from the fascial edge
- 5 mm apart (advancement between bites)
This produces a ratio of suture used vs. wound length of at least 4:1, distributing force across many stitches and reducing pull-out risk.
A 2025 meta-analysis (7 RCTs, n=2,299) confirmed small bites vs. large bites:
- Reduced ventral incisional hernia by 54% (RR 0.46)
- Reduced SSI (RR 0.73)
- Shortened length of stay [PMID 40354104]
Step-by-Step Technique
- Measure the wound length and multiply by 4 to calculate the minimum suture length required.
- Select a 2-0 slowly absorbable monofilament (PDS) on an SH needle of sufficient length. Record initial suture length.
- Pass the suture through tissue just above the apex of the fascial defect and secure with a half-blood knot (tail kept short to minimize suture loss). Measure and subtract the discarded tail.
- Run the closure with 5 mm bites back from the fascial edge, 5 mm apart, incorporating only the linea alba - no fat, no muscle.
- Approximate the fascial edges without tension. Applying tension risks suture pull-out with small bites.
- At the end, secure with an Aberdeen knot (same type used to finish subcuticular closures). Measure and subtract the remaining tail.
- Calculate achieved SL:WL ratio: (original length - tail 1 - tail 2) / wound length. If <4, remove the suture and repeat.
- If the wound is too long for one suture, use two sutures (one from each end), each secured with Aberdeen knots adjacent to each other - do not tie the sutures together (this would reduce burst strength).
- Document the wound length, total suture used, and achieved SL:WL ratio in the operative note.
Knot Details
- Half-blood knot (starting knot): Three loops of the short tail around the long end, tail passed up through all three loops, then the long end pulled to cinch. Minimizes wasted suture.
- Aberdeen knot (finishing knot): The free end is passed through the loop three times creating successive new loops; on the fourth pass the free end is pulled all the way through, tightening the knot.
Prophylactic Mesh Augmentation (PMA)
In high-risk patients (e.g., open AAA repair, morbid obesity, active smokers, collagen disorders), PMA may be considered after primary fascial closure.
- Mesh can be placed in intraperitoneal, preperitoneal, retrorectus, or onlay planes.
- Onlay and preperitoneal positions carry higher seroma risk.
- PMA is contraindicated in: patients requiring future laparotomy (e.g., stoma reversal), pregnancy, mesh allergy, and is relatively contraindicated in contaminated/infected wounds.
- PMA is not used for incisional hernia repair - it is a prophylactic adjunct to primary closure only.
Summary of Evidence-Based Principles
| Parameter | Recommendation |
|---|---|
| Suture type | Monofilament slowly absorbable (PDS) |
| Suture gauge | USP 2-0 |
| Needle | 20 mm taper tip (SH) |
| Technique | Continuous running (elective); interrupted considered in emergency/high tension |
| Bite depth | 5-8 mm from fascial edge, fascia only |
| Bite spacing | 5 mm between stitches |
| SL:WL ratio | Must achieve >4:1 |
| Peritoneum | Do not close separately |
| Subcutaneous | Close with antimicrobial suture in obese patients |
| Drains/ostomies | Never through midline incision |
Sources:
- Fischer's Mastery of Surgery, 8th ed. - Chapter on Fascial Closure in Midline Laparotomy
- Alrashidi et al. (2025) - Small vs. large bites meta-analysis, 7 RCTs, n=2,299 [PMID 40354104]
- Alharran et al. (2026) - Interrupted vs. continuous in emergency laparotomy, 25 RCTs, n=3,548 [PMID 41761330]
This is a shared conversation. Sign in to Orris to start your own chat.