Please make easy notes of chf
Reading File
Finding Sources
Searching PubMed
"heart failure" management
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have enough information from the textbooks to compile comprehensive, easy-to-read notes on CHF. Let me put it all together.
🫀 Congestive Heart Failure (CHF) - Easy Notes
1. DEFINITION
Heart failure (HF) is a clinical syndrome where the heart cannot meet the metabolic requirements of the body at normal filling pressures.
The term "heart failure" is preferred over "congestive heart failure" because pulmonary congestion may actually be absent in many HF patients.
2. EPIDEMIOLOGY
- More than 650,000 new cases diagnosed annually in the US
- Mortality remains ~50% within 5 years of diagnosis
- 1-month rehospitalization rate: ~25%
- Annual cost exceeds $39 billion
3. TYPES OF HEART FAILURE (Based on EF)
| Type | EF | Mechanism |
|---|---|---|
| HFrEF (reduced) | ≤40% | Systolic dysfunction - LV can't contract properly |
| HFmrEF (mildly reduced) | 41-49% | Intermediate group |
| HFpEF (preserved) | ≥50% | Diastolic dysfunction - LV can't relax/fill properly |
| HFimpEF (improved) | Started ≤40%, now >40% | Recovered with treatment |
- HFrEF and HFpEF each account for approximately 50% of all heart failure cases
- EF (Ejection Fraction) = LV stroke volume / end-diastolic volume
4. ACC/AHA STAGES
| Stage | Description | Examples |
|---|---|---|
| A | At risk, no structural disease | HTN, diabetes, CAD risk factors |
| B | Structural disease, no symptoms | Reduced EF, LVH, prior MI |
| C | Structural disease + symptoms | Dyspnea, fatigue, fluid retention |
| D | Advanced/refractory HF | Symptoms at rest, recurrent hospitalizations |
Stages are progressive - unlike NYHA class, they cannot go backward.
5. NYHA FUNCTIONAL CLASSIFICATION
| Class | Symptoms |
|---|---|
| I | No symptoms with ordinary activity |
| II | Slight limitation - symptoms with moderate exertion |
| III | Marked limitation - symptoms with minimal exertion |
| IV | Symptoms at rest |
6. CAUSES / TRIGGERS
- Most common: CAD, MI, hypertension
- Others: Valvular heart disease, diabetes, congenital heart defects, anemia, alcoholism, hyperthyroidism (high-output failure), Paget disease
7. PATHOPHYSIOLOGY (Simple Version)
Cardiac injury (MI, HTN, etc.)
↓
LV Remodeling (stretching + dilation)
↓
Neurohormonal activation:
• RAAS → Angiotensin II → aldosterone → fibrosis + apoptosis
• SNS → Catecholamines → toxic to myocardium, ↑O₂ demand
• Endothelin-1 → vasoconstriction
↓
Progressive worsening of LV function
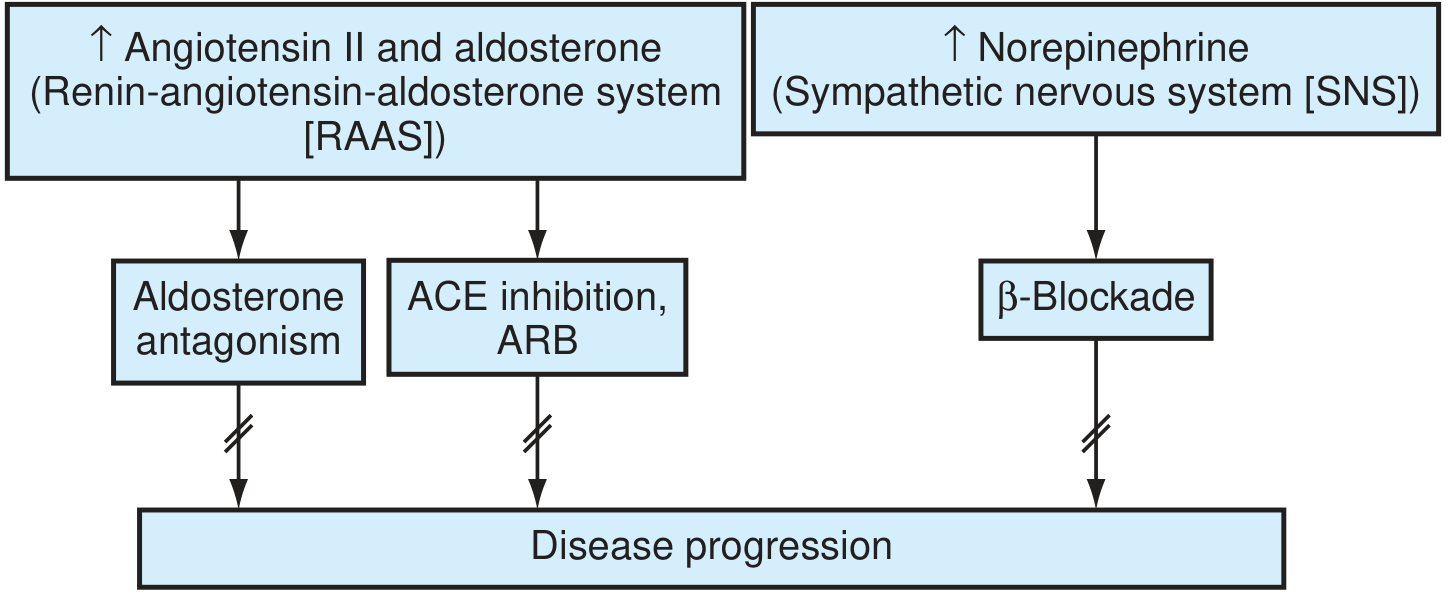
Figure: The RAAS and sympathetic nervous system - key targets in HF treatment. (Textbook of Family Medicine 9e)
8. CLINICAL FEATURES
Left-sided HF (pulmonary congestion):
- Dyspnea on exertion
- Orthopnea (need to sit upright to breathe)
- Paroxysmal nocturnal dyspnea (PND)
- Bilateral rales/crackles
- S3 gallop
Right-sided HF (systemic venous congestion):
- Jugular venous distension (JVD)
- Pitting pedal edema
- Hepatomegaly, ascites
- Hepatojugular reflux
General:
- Fatigue, reduced exercise tolerance
- Cool extremities (poor perfusion)
- Cardiac cachexia (late stage) - nausea, anorexia, muscle wasting
- Cognitive dysfunction (up to 25% have depression)
- Sleep-disordered breathing in ~70% of patients
9. DIAGNOSIS
| Investigation | What it shows |
|---|---|
| Chest X-ray | Cardiomegaly, pulmonary congestion, pleural effusion |
| ECG | LVH, old MI, arrhythmias |
| Echocardiogram | EF, wall motion, valve function - most important |
| BNP / NT-proBNP | Elevated in HF; helps confirm diagnosis and assess severity |
| Labs | CBC, BMP (renal function, K+), LFTs, TFTs, glucose, lipids |
| Hemodynamic monitoring | For severe cases where filling pressures can't be clinically assessed |
10. TREATMENT
Goals:
- Relieve symptoms
- Prevent hospitalizations
- Reduce mortality
🔵 HFrEF (EF ≤40%) - The "Fantastic Four" (Foundational Therapies)
All four should be started as quickly as possible at low doses and uptitrated:
| Drug Class | Examples | Why |
|---|---|---|
| ARNI (preferred) or ACE-i/ARB | Sacubitril-valsartan / Enalapril, Lisinopril | Block RAAS, reduce remodeling |
| Beta-blocker | Carvedilol, Metoprolol succinate, Bisoprolol | Block SNS toxicity, reduce mortality |
| MRA (Mineralocorticoid Receptor Antagonist) | Spironolactone, Eplerenone | Block aldosterone escape, anti-fibrotic |
| SGLT2 inhibitor | Dapagliflozin, Empagliflozin | Improve survival, reduce hospitalizations, improve symptoms |
Diuretics (furosemide) are added for fluid/congestion control but do not reduce mortality on their own.
ACE Inhibitor Dosing Guide
| Drug | Starting Dose | Target Dose |
|---|---|---|
| Captopril | 6.25 mg TID | 50 mg TID |
| Enalapril | 2.5 mg BD | 10-20 mg BD |
| Lisinopril | 2.5-5 mg OD | 20-35 mg OD |
| Ramipril | 2.5 mg OD | 5 mg BD or 10 mg OD |
ARB Dosing Guide
| Drug | Starting Dose | Target Dose |
|---|---|---|
| Candesartan | 4-8 mg OD | 32 mg OD |
| Valsartan | 40 mg BD | 160 mg BD |
| Losartan | 50 mg OD | 150 mg OD |
⚠️ Important drug cautions:
- Avoid NSAIDs (worsen HF, interact with diuretics/ACE-i)
- Avoid non-dihydropyridine calcium channel blockers (verapamil, diltiazem) in HFrEF
- Watch for hyperkalemia with ACE-i + MRA + SGLT2 combination
🔴 Device Therapy (Advanced HFrEF):
- ICD (Implantable Cardioverter Defibrillator) - for EF ≤35%, prevent sudden cardiac death
- CRT (Cardiac Resynchronization Therapy) - for EF ≤35% + LBBB + QRS >150ms
- Heart transplant / LVAD - Stage D refractory HF
11. ACUTE / DECOMPENSATED HF MANAGEMENT
Think "LMNOP":
- L - Lasix (furosemide IV)
- M - Morphine (relieves anxiety, reduces preload)
- N - Nitrates (reduce preload/afterload)
- O - Oxygen
- P - Position upright (legs down)
12. MONITORING
- Weight daily (>2 kg gain in 2 days = alert)
- Blood pressure, heart rate
- Renal function + electrolytes (K+, Na+, creatinine) - especially when starting/titrating drugs
- Check labs 1-2 weeks after starting or dose-titrating ACE-i/ARB
13. PROGNOSIS
- 50% mortality at 5 years overall
- HFrEF has better evidence-based treatment options
- HFpEF prognosis is similar but fewer mortality-reducing treatments are proven
- Cardiac cachexia = poor prognosis sign
Quick Memory Trick
"DABS" = the 4 foundational drugs for HFrEF:
- Diuretic (symptom control)
- ARNI / ACE-i
- Beta-blocker
- SGLT2 inhibitor + Spironolactone (MRA)
Sources: Goldman-Cecil Medicine, Textbook of Family Medicine 9e, Fuster and Hurst's The Heart 15e, Braunwald's Heart Disease
Recent evidence update (2025): A meta-analysis (PMID: 40884036, Circulation Nov 2025) confirmed that dapagliflozin initiated in hospitalized HF patients reduces subsequent cardiovascular death and worsening HF events, further supporting early SGLT2 inhibitor use even during acute admission.
This is a shared conversation. Sign in to Orris to start your own chat.