Subclavian steal syndrome
Reading File
Finding Sources
Searching PubMed
"subclavian steal syndrome"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compose the full answer.
Subclavian Steal Syndrome
Definition
Subclavian steal syndrome (also called Millikan-Siekert syndrome) occurs when significant stenosis or occlusion of the subclavian artery proximal to the origin of the vertebral artery causes reversal of blood flow in the ipsilateral vertebral artery, siphoning blood away ("stealing") from the vertebrobasilar circulation into the hypoperfused arm.
- Bradley and Daroff's Neurology in Clinical Practice
- Gray's Anatomy for Students
Anatomy and Pathophysiology
The "Steal" Mechanism
The left and right vertebral arteries arise from their respective subclavian arteries, ascend through the transverse foramina of the cervical vertebrae, and unite to form the basilar artery. This confluence is the anatomical key to the steal:
When the proximal subclavian artery is severely stenotic or occluded, vascular resistance in the ipsilateral arm falls dramatically during upper limb exercise. The normal pressure gradient reverses - blood is siphoned from the basilar artery back down the ipsilateral vertebral artery and into the distal subclavian artery (past the obstruction), bypassing the stenosis. The result is hypoperfusion of the posterior fossa (brainstem, cerebellum, occipital cortex).
- Grainger & Allison's Diagnostic Radiology
Collateral Channels
Because stenosis develops gradually, several collateral pathways enlarge over time and can maintain upper limb perfusion at rest. During exercise, these dilate further, accentuating the steal:
- Vertebral artery muscular branches - anastomose with the ascending and deep cervical arteries, draining into the thyrocervical and costocervical trunks and thence into the subclavian artery distal to the obstruction.
- Thyroid anastomoses - the right and left thyroid arteries anastomose within the gland; blood is shunted via the inferior thyroid artery retrograde to the thyrocervical trunk.
- Occipital artery - branches join the deep cervical artery and the superior thyroid artery, providing additional indirect routes to the distal subclavian.
- Gray's Anatomy for Students
Why the Left Side Predominates
The left subclavian artery is more frequently involved because it arises directly from the aortic arch (a common site of atherosclerosis), whereas the right subclavian arises from the brachiocephalic trunk.
Etiology
| Cause | Notes |
|---|---|
| Atherosclerosis | Most common; typically in older adults with dyslipidaemia |
| Takayasu arteritis | Should be suspected in young women with brachiocephalic disease |
| Thoracic outlet / external compression | Rare (e.g., cervical rib, schwannoma) |
| Radiation arteritis | Prior mediastinal irradiation |
| Congenital anomalies | Aberrant subclavian artery |
Clinical Features
The syndrome is asymptomatic at rest in many patients; symptoms are provoked by vigorous ipsilateral arm exercise.
Vertebrobasilar (neurological) symptoms:
- Vertigo and dizziness
- Syncope or "drop attacks" (sudden fall without loss of consciousness)
- Diplopia, binocular visual loss, transitory visual disturbances
- Facial paraesthesiae
- Headache
- Dysarthria, ataxia
Upper limb symptoms:
- Arm fatigue and muscle cramping with exertion
- (Limb ischaemia is uncommon because collaterals are usually adequate)
- Unilateral digital ischaemia from microembolisation is a warning sign requiring urgent investigation
Physical examination signs:
- Blood pressure discrepancy ≥20 mmHg between arms (affected side lower)
- Diminished or absent radial/brachial pulse on the affected side
- Subclavian/supraclavicular bruit
- Reproduction of symptoms with arm exercise (reactive hyperaemia test)
A BP difference of ≥40 mmHg between arms is particularly concerning.
- Rosen's Emergency Medicine; Current Surgical Therapy 14e
Diagnosis
Duplex Ultrasound (first-line)
The vertebral artery is interrogated in the mid-neck. Key findings:
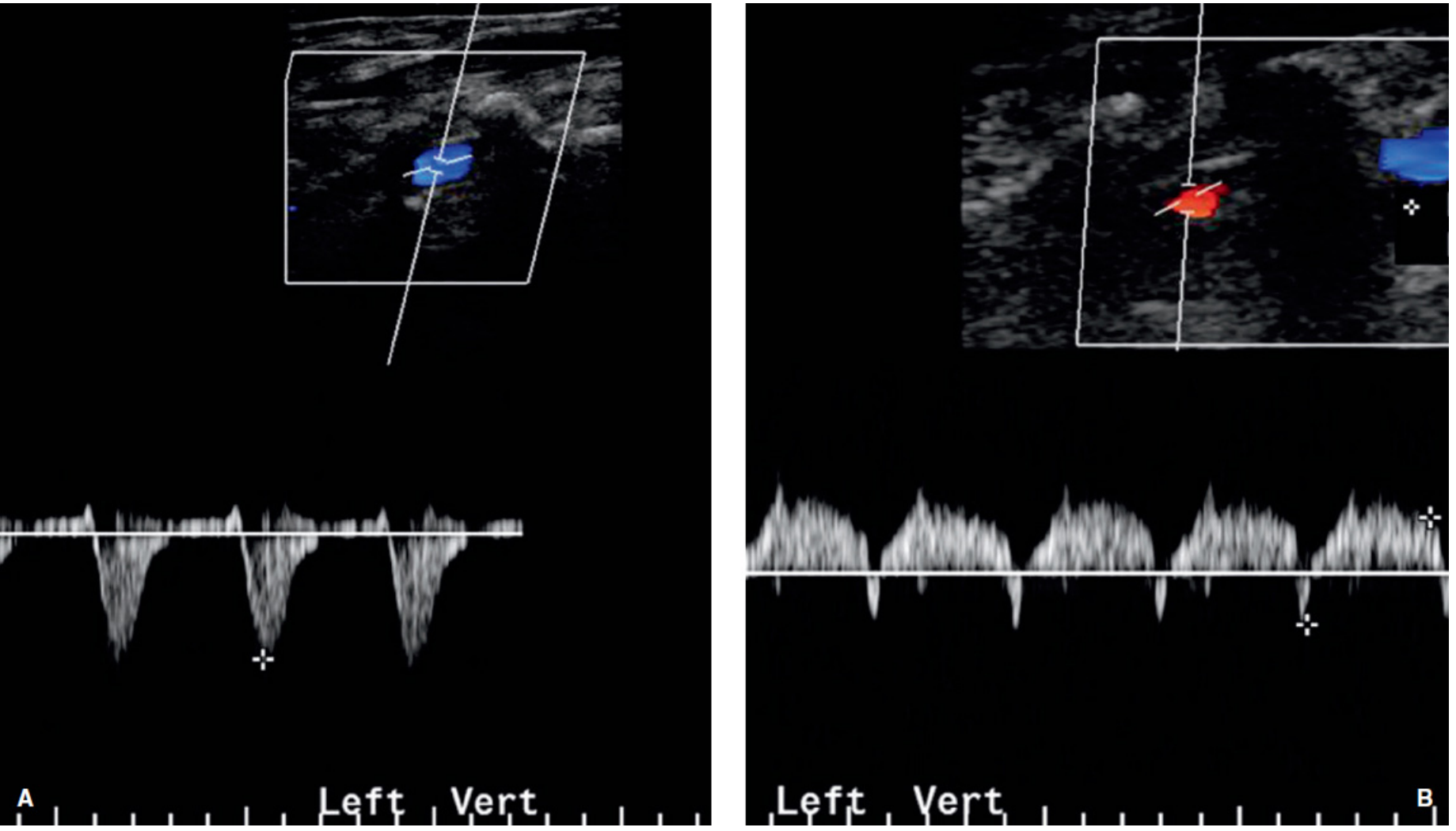
- Retrograde (reversed) flow in the vertebral artery - displayed as flow below baseline on spectral Doppler and the same colour as the adjacent vein on colour Doppler
- Biphasic ("to and fro") flow - seen with subtotal subclavian stenosis rather than complete occlusion; flow alternates above and below baseline with each heartbeat
- High-resistance vertebral waveform pattern
The Doppler appearance of reverse vs. biphasic vertebral flow is shown below:
CTA and MRA
Both require IV contrast and allow visualisation of the aortic arch and brachiocephalic vessels. CTA is generally preferred over MRA because it is faster, better tolerated (less claustrophobia, less cardiac motion artifact), and MRA tends to overestimate stenosis severity.
Digital subtraction angiography (DSA)
Remains the gold standard and is particularly appropriate when endovascular treatment is being planned.
- Current Surgical Therapy 14e; Grainger & Allison's Diagnostic Radiology
Treatment
Who needs treatment?
- Symptomatic steal (vertebrobasilar symptoms with arm exercise): treatment indicated
- Asymptomatic steal: generally observed; exceptions include:
- Patients who require ipsilateral internal mammary artery as a coronary bypass conduit (LIMA steal could cause myocardial ischaemia)
- Difficult haemodialysis access cases
- Preocclusive proximal common carotid disease
- Isolated proximal subclavian occlusive disease causing only arm fatigue rarely requires intervention given the rich collateral network
Endovascular (preferred for isolated subclavian disease)
- Percutaneous transluminal angioplasty and stenting of the stenotic subclavian artery
- Preferred over open surgery for isolated left subclavian disease because of lower morbidity, comparable patency, and avoidance of thoracotomy/sternotomy
Open Surgical - Extraanatomic (indirect) revascularisation
For isolated unilateral proximal subclavian lesions, extraanatomic procedures through supraclavicular incisions are well tolerated with low morbidity and excellent patency:
- Carotid-subclavian bypass (prosthetic 7-8 mm Dacron or PTFE graft) - most common
- Subclavian-carotid transposition - the subclavian artery is transected and reimplanted end-to-side into the common carotid artery; avoids prosthetic material
- Axilloaxillary bypass - an option when ipsilateral carotid disease precludes using it as inflow
Open Surgical - Anatomic (direct) revascularisation
Reserved for multivessel brachiocephalic disease requiring median sternotomy:
- Aorto-brachiocephalic bypass with ascending aorta as inflow
- Innominate endarterectomy for focal non-ostial atherosclerosis (not suitable for ostial lesions or bovine arch anatomy)
Reported outcomes for brachiocephalic reconstruction: 30-day mortality 4-7%, perioperative stroke 2-5%, 5-year and 10-year patency >90%.
- Current Surgical Therapy 14e (Mulholland & Greenfield's Surgery)
Key Points Summary
| Feature | Detail |
|---|---|
| Mechanism | Retrograde vertebral artery flow due to proximal subclavian stenosis/occlusion |
| Most affected side | Left (>right) |
| Trigger | Ipsilateral arm exercise |
| Core symptom triad | Arm fatigue + vertebrobasilar symptoms + BP discrepancy |
| Best initial test | Duplex Doppler ultrasound (retrograde or biphasic vertebral flow) |
| Gold standard imaging | Digital subtraction angiography |
| First-line treatment | Endovascular angioplasty/stenting |
| Surgical fallback | Carotid-subclavian bypass or transposition |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Gray's Anatomy for Students; Grainger & Allison's Diagnostic Radiology; Current Surgical Therapy 14e; Mulholland & Greenfield's Surgery 7e; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.