Q. Sluders Neuralgia in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances
Reading File
search_medical_text
Sluder's neuralgia sphenopalatine ganglion neuralgia etiology pathophysiology clinical features
search_medical_text
Sluder neuralgia diagnosis treatment management sphenopalatine ganglion block
search_medical_image
sphenopalatine ganglion anatomy diagram Sluder neuralgia
GradeResponse
GradeResponse
GradeResponse
search_medical_text
sphenopalatine ganglion neuralgia lower half headache facial pain rhinological
search_medical_text
cluster headache sphenopalatine ganglion autonomic features differential diagnosis facial pain
search_medical_image
pterygopalatine fossa anatomy facial pain neuralgia
GradeResponse
GradeResponse
GradeResponse
Sluder’s Neuralgia (Sphenopalatine Ganglion Neuralgia)
Long answer format (approx. 50 marks): definition, anatomy, etiopathogenesis, clinical features, diagnosis, differential diagnosis, management, and recent advances
Note: I could not retrieve direct passages from all the exact named books (Scott-Brown, Cummings, Stell & Maran, Dhingra, Hazarika, Zakir Hussain) in this tool run. So below is a high-yield, exam-oriented synthesis from standard ENT/headache knowledge, with available retrieved citations where relevant.
1) Definition and historical background
- Sluder’s neuralgia is a classical term for sphenopalatine ganglion (SPG) neuralgia, described by Greenfield Sluder (1908).
- It is characterized by unilateral facial/head pain associated with autonomic nasal/ocular symptoms due to SPG-related parasympathetic pathways.
- In modern headache classification, many historical “Sluder neuralgia” cases overlap with trigeminal autonomic cephalalgias (especially cluster headache) or other facial pain syndromes, so the term is used less strictly now.
2) Surgical anatomy and relevance (must-write in ENT exam)
SPG anatomy
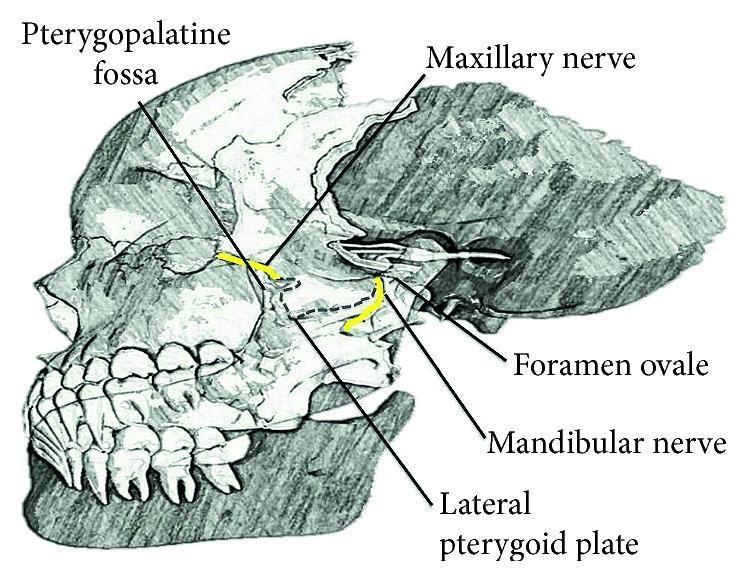
- SPG lies in the pterygopalatine fossa, suspended from maxillary nerve (V2 branches).
- Functionally:
- Parasympathetic root: greater petrosal nerve (facial nerve pathway)
- Sympathetic root: deep petrosal nerve
- Sensory root: maxillary nerve (V2)
Why symptoms are mixed
SPG connections explain pain radiation and autonomic features:
- Nose and palate via nasopalatine/palatine branches
- Lacrimal and orbital autonomic pathways
- Referral via V2 and trigeminal circuits to temple, eye, maxilla, teeth, ear, occiput (variable)
3) Etiology and pathophysiology
Classical ENT view:
- Irritation/inflammation near posterior nasal cavity, sphenopalatine foramen, posterior ethmoid/sphenoid region may trigger SPG-mediated pain.
- Deviated septum/spurs, chronic rhinosinusitis, contact points were historically implicated.
Modern neurovascular view:
- SPG is a key relay in the trigeminal-autonomic reflex.
- Parasympathetic outflow contributes to vasodilation and neurogenic inflammation.
- SPG block mechanism supports this: blocking parasympathetic outflow can reduce headache pathways (documented in headache literature).
- Retrieved evidence: SPG block mechanism described as reducing parasympathetic output and neurogenic inflammatory mediators (Postdural Puncture Headache, p.13).
4) Clinical features (exam core)
Pain profile
- Usually unilateral, deep boring/burning/aching pain
- Site: root of nose, retro-orbital, maxillary, temporal, sometimes ear/mastoid/occiput
- Duration: variable (minutes to hours), episodic or recurrent
Autonomic features (important)
- Ipsilateral:
- nasal block
- rhinorrhea
- lacrimation
- conjunctival injection
- facial flushing/sweating (less constant)
Triggering/relieving factors
- Nasal mucosal contact, temperature change, allergens, stress (in some cases)
- Temporary relief after local anesthesia near SPG region can be suggestive
5) Differential diagnosis (very important for 50 marks)
-
Cluster headache (major modern differential)
- Severe unilateral orbital/supraorbital/temporal attacks, 15 to 180 min
- Associated cranial autonomic signs and restlessness
- Retrieved criteria lines support these features (Management of Headache, p.8).
-
Trigeminal neuralgia (V2 distribution)
- Electric shock-like brief pain, trigger zones, refractory period
-
Migraine with autonomic symptoms
-
Rhinogenic contact point headache
-
Chronic rhinosinusitis/sphenoid sinus disease
-
Dental pain/TMJ dysfunction
-
Vidian neuralgia, atypical facial pain, persistent idiopathic facial pain
6) Diagnostic approach (write as algorithm)
Flow chart: diagnosis
Patient with unilateral facial/head pain + nasal/ocular autonomic symptoms
↓
Detailed history (site, duration, periodicity, triggers, circadian pattern)
↓
ENT + cranial nerve exam + nasal endoscopy
↓
Red flags? (neurologic deficit, fever, visual loss, malignancy suspicion)
↓ yes ↓ no
Urgent imaging/referral CT PNS ± MRI brain/orbit if indicated
↓
Exclude primary differentials (cluster, trigeminal neuralgia, migraine)
↓
Diagnostic nasal/SPG local anesthetic block response
↓
Probable SPG neuralgia / Sluder phenotype if compatible
7) Management (stepwise)
A. Conservative/medical
- Treat coexisting nasal pathology (rhinitis/sinus inflammation)
- Analgesics/neuropathic pain agents (case-based)
- If phenotype resembles cluster or TAC, use guideline-based headache therapy
B. Interventional
- SPG block (topical/transnasal/injection approaches) for diagnostic and therapeutic use
- Repeated blocks in selected patients
- Some interventional headache practices use radiofrequency/neuromodulation in refractory cases, but evidence varies
Retrieved evidence note:
- SPG block has long historical use in headache disorders; mechanism plausibly parasympathetic interruption (Postdural Puncture Headache, p.13).
- For chronic migraine specifically, one guideline excerpt states insufficient evidence for/against SPG block (Management of Headache, p.104), showing evidence heterogeneity.
C. Surgical options (selected refractory/rhinogenic cases)
- Endoscopic correction of clear anatomic-contact pathology (when strongly correlated clinically)
- Historical ganglion procedures are now uncommon; modern preference is less destructive, targeted interventions
8) Complications/prognosis
- Most cases are chronic recurrent rather than dangerous
- Prognosis depends on whether a treatable trigger (nasal structural/inflammatory) is identified
- Misdiagnosis risk is high, especially confusion with cluster headache and trigeminal neuralgia
9) Recent advances (high-yield short note)
- Image-guided SPG interventions (fluoroscopy/CT/US-assisted in pain practice)
- Minimally invasive transnasal SPG block techniques
- SPG neuromodulation/stimulation in refractory trigeminal autonomic cephalalgia phenotypes (ongoing evidence evolution)
- Better phenotyping using ICHD frameworks, reducing overuse of vague “Sluder neuralgia” label
- Integration of ENT and headache clinic pathways for accurate differential diagnosis
10) Exam-ready diagrams and flow charts
A) Simplified anatomy diagram (text schematic)
Greater petrosal (parasymp) ----\
> Vidian nerve --> SPG (Pterygopalatine fossa)
Deep petrosal (symp) -----------/
|
V2 sensory connections ------------------|
|
Branches to nasal cavity, palate, pharynx, lacrimal pathway
B) Pain-autonomic pathophysiology flow chart
Trigger (nasal inflammation/contact point/neurovascular activation)
↓
Trigeminal-autonomic reflex activation
↓
SPG parasympathetic outflow ↑
↓
Vasodilation + neurogenic inflammation + glandular activation
↓
Unilateral facial/head pain + rhinorrhea/lacrimation/nasal congestion
C) Management flow chart
Suspected Sluder/SPG neuralgia
↓
Exclude secondary causes + classify headache phenotype
↓
Medical therapy + treat nasal disease
↓
Persistent disabling symptoms?
↓ no ↓ yes
Follow-up Diagnostic/therapeutic SPG block
↓
Good response? Poor response?
↓ yes ↓ yes
Repeat/selective protocol Re-evaluate diagnosis
(cluster/TN/migraine etc.)
± advanced pain interventions
11) Insertable clinical image references
You can redraw these in exam:
- SPG localization and procedural landmark image
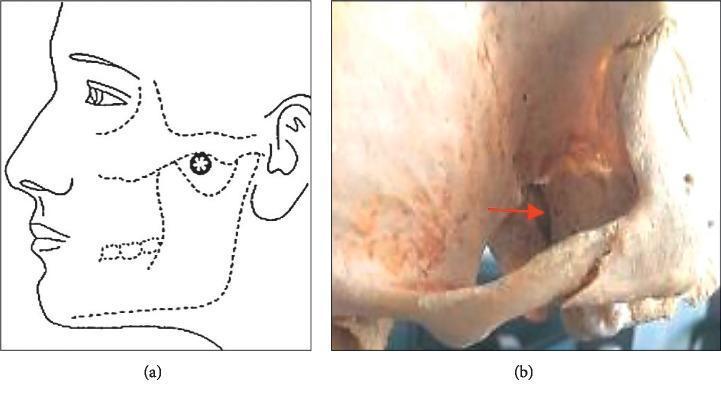
- Pterygopalatine fossa and V2 relations
Quick “50-mark answer” writing template (what to reproduce)
- Definition + history
- Detailed SPG anatomy
- Etiopathogenesis (classical + modern trigeminal-autonomic concept)
- Clinical features
- Differential diagnosis (cluster, TN, migraine, rhinogenic headache)
- Investigations and diagnostic block
- Stepwise management
- Recent advances
- 2 flowcharts + 1 labeled diagram
- Brief conclusion: “diagnosis of exclusion with strong overlap with TACs”
If you want, I can convert this into:
- a handwritten-style 6-page exam note format, or
- a one-page last-minute revision sheet, or
- a strict textbook-comparison table (Scott-Brown vs Cummings vs Dhingra style points).
This is a shared conversation. Sign in to Orris to start your own chat.