Give Me DNB style Distinction answer for Cricothyrotomy and percutaneous tracheostomy including relevant diagrams, flowchart, keywords, bullet point
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
cricothyrotomy cricothyroid membrane anatomy surgical procedure
Reading File
Searching Images
percutaneous dilatational tracheostomy Seldinger technique guidewire ICU
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the material needed. Let me compose the comprehensive DNB-style distinction answer.
✦ DNB DISTINCTION ANSWER
Cricothyrotomy and Percutaneous Tracheostomy
🔑 KEY WORDS / HIGH-YIELD TAGS
CICO · Cannot Intubate Cannot Oxygenate · Cricothyroid Membrane (CTM) · Seldinger Technique · Ciaglia Blue Rhino · Percutaneous Dilatational Tracheostomy (PDT) · PEAA · Failed Airway · Jet Ventilation · Tracheoinnominate Fistula · Subglottic Stenosis · Bronchoscopic GuidancePART 1 — CRICOTHYROTOMY
1.1 Definition & Synonyms
Cricothyrotomy (= cricothyroidotomy = coniotomy = minitracheostomy) is the establishment of an emergency airway through the cricothyroid membrane (CTM) — a fibroelastic membrane between the inferior border of the thyroid cartilage and the superior edge of the cricoid cartilage.
Two forms:
- Surgical/Open cricothyrotomy — incision + tube insertion
- Needle cricothyrotomy → Percutaneous Translaryngeal Ventilation (PTLV) / Transtracheal Jet Ventilation
1.2 Relevant Anatomy
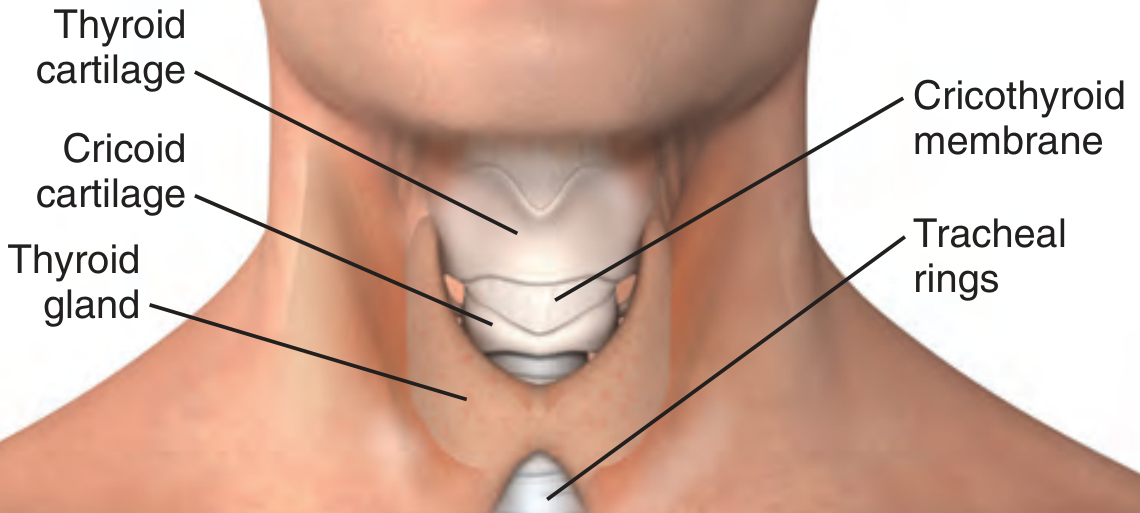
Fig. 1 — Normal adult larynx showing position of the cricothyroid membrane
| Structure | Detail |
|---|---|
| CTM dimensions | ~9 mm longitudinally × 30 mm transversely |
| Location | 2–3 cm inferior to laryngeal prominence (Adam's apple) / 4 fingerbreadths above sternal notch |
| Borders | Superior: thyroid cartilage; Inferior: cricoid cartilage |
| Vascularity | Relatively avascular; cricothyroid arteries arch only at the SUPERIOR aspect → incise in the LOWER 1/3 |
| Landmark | Cricoid = ONLY completely circumferential cartilaginous ring of larynx |
Pitfall: Cricothyroid arteries branch from the superior thyroid artery and traverse the superior CTM — always incise in the caudad (lower) third of the membrane.
1.3 Indications
- Primary: Cannot Intubate, Cannot Oxygenate (CICO) = Failed Airway
- Inability to maintain SpO₂ >90% between intubation attempts
- Failure after ≥3 attempts at endotracheal intubation
- Inability to bag-mask-valve ventilate
- Failure of rescue maneuvers (GEB, iLMA, video laryngoscopy)
1.4 Contraindications
| Absolute | Relative |
|---|---|
| Age <5–12 years (larynx too small; narrow-bore needle only) | Distorted/inaccessible neck anatomy |
| Laryngeal fracture | Overlying infection or hematoma |
| Tracheal transection below CTM | Operator inexperience |
| Obstruction below CTM |
1.5 Techniques
A. Surgical (Open) Cricothyrotomy — Steps
1. Position: supine, neck extended (shoulder roll)
2. Identify CTM: "Laryngeal Handshake"
- Dominant hand cephalad; thumb & middle finger stabilize
thyroid cartilage; index finger palpates CTM
3. Stabilise larynx; vertical stab incision (1.5 cm) through skin
4. Horizontal incision through lower 1/3 of CTM
5. Hook caudal edge of CTM; dilate with tracheal hook or
curved haemostat
6. Insert tracheostomy tube (Shiley 6.0) or ETT (6.0 cuffed)
→ direct caudally
7. Inflate cuff, confirm with ETCO₂ + bilateral auscultation
8. Secure tube; convert to formal tracheostomy within 72 hrs
Scalpel-Bougie technique (DAS/UK guideline preferred):
- Single vertical incision → horizontal CTM stab → bougie inserted caudally → 6.0 ETT railroaded over bougie
B. Needle Cricothyrotomy / PEAA (Percutaneous Emergency Airway Access)
1. 14-gauge over-needle catheter attached to syringe
2. Advance at 45° caudally through caudad 1/3 of CTM
3. Continuous negative aspiration → free air confirms placement
4. Advance catheter; remove needle
5. Attach to jet ventilator (15 psi) or BVM via adapter
6. I:E ratio 1:4 to allow CO₂ exhalation
(ventilation is achieved but CO₂ clearance LIMITED)
Key limitation: Needle cricothyrotomy = oxygenation only (30–45 min maximum). CO₂ rises → MUST convert to definitive airway.
Devices: Cook Transtracheal Airway Catheter, Ravussin Catheter (pre-curved, kink-resistant)
1.6 Step-by-Step Flowchart
DIFFICULT AIRWAY
│
┌─────────▼─────────┐
│ Attempt ETI (x3) │
│ ± Video laryngoscopy │
│ ± GEB / LMA │
└─────────┬─────────┘
│ FAIL
▼
┌────────────────────┐
│ SpO₂ >90%? │
│ BVM maintainable? │
└──────┬─────┬───────┘
YES NO
│ │
One more ┌─▼──────────────────────┐
attempt │ FAILED AIRWAY = CICO │
│ CRICOTHYROTOMY NOW │
└─┬──────────────────────┘
│
┌───────▼────────────────┐
│ Surgical Cricothyrotomy│◄── Preferred
│ (Scalpel-Bougie or │
│ Standard Open) │
└───────┬────────────────┘
│ If surgical not possible
▼
┌──────────────────────────┐
│ Needle Cricothyrotomy │
│ + Jet Ventilation/BVM │
│ (Bridge, max 30–45 min) │
└──────────────────────────┘
│
▼
Convert to formal tracheostomy
within 24–72 hours
1.7 Complications
| Timing | Complication |
|---|---|
| Acute | Bleeding / haematoma |
| Tube malposition / false passage | |
| Bronchial intubation (right main) | |
| Laryngotracheal injury | |
| Tension pneumothorax | |
| Subcutaneous emphysema | |
| Late | Subglottic stenosis (feared; historically overestimated — Brantigan & Grow 1976 refuted Jackson's 1921 concerns) |
| Subjective voice changes | |
| Difficulty swallowing | |
| Persistent stoma | |
| Infection |
Historical pearl: Chevalier Jackson (1921) reported subglottic stenosis as a major complication of cricothyrotomy; this led to its abandonment. Brantigan and Grow (1976) conclusively refuted this — complication rates were comparable to tracheostomy if proper technique was used.
PART 2 — PERCUTANEOUS TRACHEOSTOMY (PDT)
2.1 Definition & History
Percutaneous Dilatational Tracheostomy (PDT) is a bedside ICU procedure using the Seldinger (guidewire) technique to establish a definitive tracheal airway through serial dilation, without open surgical dissection.
Timeline:
- 1626 — Sanctorius: first percutaneous tracheal cannulation ("ripping needle")
- 1869 — Trendelenburg: first cuffed tracheostomy tube
- Late 1960s — Toye & Weinstein: Seldinger guidewire for tracheal access
- 1985 — Pasquale Ciaglia: described modern PDT → "Ciaglia technique" → now the gold standard
2.2 Anatomy for PDT
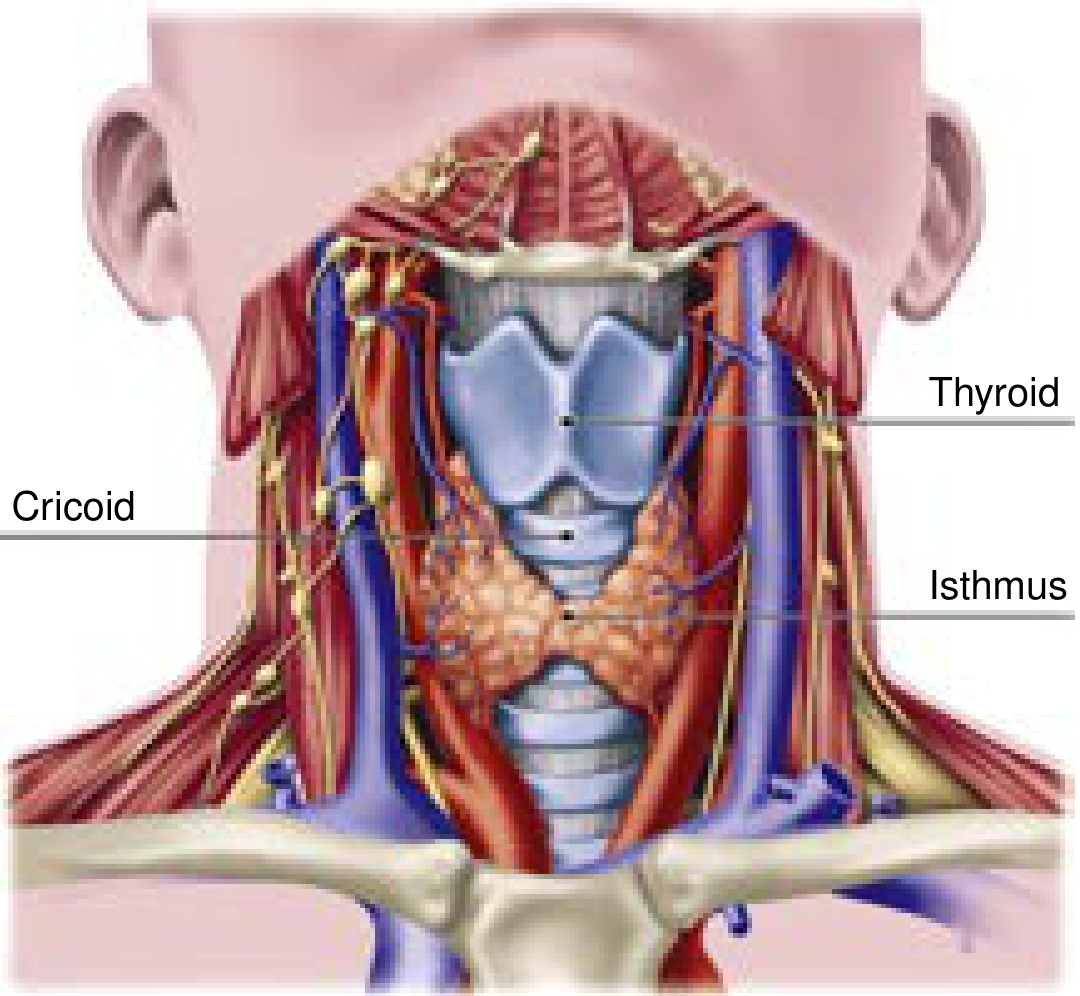
Fig. 2 — Tracheal anatomy showing thyroid gland, cricoid, thyroid cartilage and isthmus
| Feature | Detail |
|---|---|
| Trachea length | 11 ± 1 cm (♂); 10 ± 1 cm (♀) |
| Tracheal diameter | 2.5–2.7 cm (♂); 2.1–2.3 cm (♀) |
| Tracheal rings | 18–22 incomplete semicircular cartilaginous rings |
| Ideal entry site | Between 1st–2nd or 2nd–3rd tracheal rings |
| Danger above | Cricoid cartilage — avoid → subglottic stenosis risk |
| Danger below | Innominate artery (especially if high-riding) → tracheoinnominate fistula |
| Thyroid isthmus | Overlies rings 2–4; assess with USS |
2.3 Indications
- Prolonged mechanical ventilation (most common; controversial timing)
- Upper airway obstruction (head/neck malignancy, angioedema, burns, trauma)
- Airway protection after neurological events (CVA, TBI, ICH)
- Chronic neuromuscular disease (MND, GBS, high cervical SCI)
- Obstructive sleep apnea (selected cases)
- Central airway obstruction (neoplasm, subglottic stenosis, radiation stricture)
- Emergency adjunct when ETI has failed
2.4 Timing
| Classification | Definition |
|---|---|
| Early tracheostomy | ≤4–7 days of intubation |
| Late tracheostomy | >10 days |
Current evidence: Multiple RCTs and meta-analyses (including the TracMan trial: 1,032 patients, 57 sites) show no mortality benefit of early vs. late tracheostomy. However, early tracheostomy may reduce ventilator-associated pneumonia (VAP). Decision must be individualised.
2.5 Contraindications
| Absolute | Relative |
|---|---|
| Cellulitis/deep infection at site | Coagulopathy (PT/PTT >1.5× control; platelets <50,000) |
| Operator inexperience | Thrombocytopenia |
| Emergent airway (use surgical cricothyrotomy) | |
| Inability to palpate tracheal anatomy | |
| Overlying vessels | |
| High PEEP requirement (>12 cmH₂O) — derecruitment risk | |
| Morbid obesity (relative; USS guidance helps) |
Uremia: PDT safe but pretreat with DDAVP (desmopressin) to improve platelet function.
2.6 Ciaglia Blue Rhino PDT — Step-by-Step Procedure
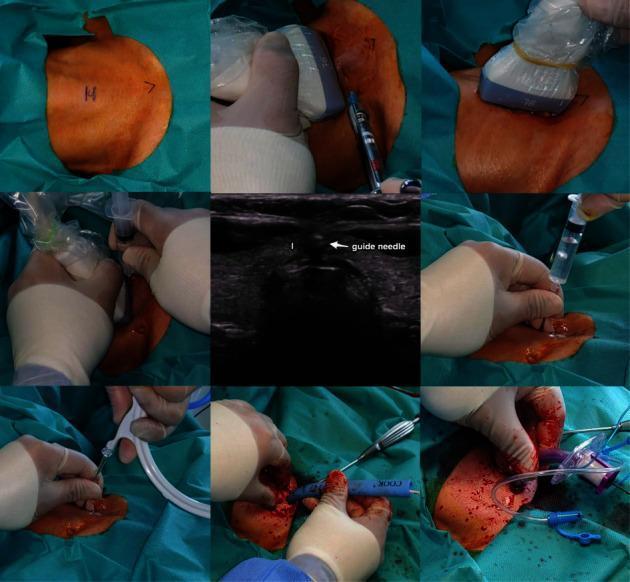
Fig. 3 — Step-by-step USS-guided percutaneous dilatational tracheostomy using the Ciaglia Blue Rhino technique
PRE-PROCEDURE
─────────────
✓ Review CT neck (high-riding innominate artery, aberrant vessels)
✓ USS neck: identify vessels, thyroid isthmus, tracheal rings
✓ Labs: PT, PTT, platelets, BUN
✓ Increase FiO₂ to 1.0
✓ Shoulder roll → neck extended
✓ Sedation + analgesia + short-acting paralysis
✓ Sterile prep and drape
PROCEDURE (Ciaglia Blue Rhino)
──────────────────────────────
Step 1: Identify entry site — between rings 1–2 or 2–3
Step 2: Infiltrate 10 mL of 1% lidocaine + epinephrine
Step 3: 1.0–1.5 cm horizontal (or vertical) skin incision
→ blunt dissect to tracheal rings
Step 4: Bronchoscope positioned at distal ETT tip;
Transillumination through anterior neck confirms level
Step 5: ETT cuff deflated; ETT pulled back to subglottis
(bronchoscopist confirms position)
Step 6: 14-gauge introducer needle inserted MIDLINE
under direct bronchoscopic vision
Step 7: Aspiration of air + direct bronchoscopic view =
confirmation of intratracheal position
Step 8: J-tipped guidewire advanced toward carina
Step 9: Short 14-Fr dilating catheter used for initial dilation
Step 10: Single tapered Blue Rhino dilator over guidewire
(AVOID posterior tracheal membrane)
Step 11: Tracheostomy tube (loaded on obturator) passed
over guidewire → cuff inflated
Step 12: Confirm position — bronchoscopy through ETT
then through tracheostomy; tidal volume return
POST-PROCEDURE
──────────────
✓ Secure tube; CXR to exclude pneumothorax
✓ Tracheostomy collar/ties
✓ Suction setup
2.7 PDT Flowchart
PATIENT REQUIRING TRACHEOSTOMY
│
┌────────────▼────────────────┐
│ Assess anatomy (USS ± CT) │
│ Labs: PT, PTT, Plt, BUN │
└────────────┬────────────────┘
│
┌────────────▼──────────────────────────┐
│ Is anatomy favourable? │
│ - Palpable cartilages? │
│ - No overlying vessels? │
│ - Coagulation acceptable? │
│ - PEEP <12 cmH₂O? │
└────┬──────────────────────┬───────────┘
YES NO
│ │
▼ ▼
PDT (Bedside ICU) Surgical Tracheostomy
Bronchoscopy-guided (OR, open dissection)
│
▼
Seldinger technique:
Needle → Guidewire → Dilator → Tube
│
▼
Confirm: Bronchoscopy + ETCO₂ + CXR
│
▼
Ongoing tracheostomy care &
early decannulation assessment
2.8 PDT vs. Surgical Tracheostomy — Comparison
| Feature | PDT | Surgical Tracheostomy |
|---|---|---|
| Setting | ICU bedside | Operating room (or bedside) |
| Anaesthesia | Sedation + paralysis | General / conscious sedation |
| Incision | Small (1–1.5 cm) | Larger dissection |
| Bleeding control | Limited (no electrocautery) | Electrocautery available |
| Visualisation | Indirect (bronchoscope) | Direct |
| Cost | Lower | Higher |
| Time | Shorter | Longer |
| Infection | Lower wound infection rate | Slightly higher |
| Emergency use | NOT ideal | Preferred for emergency |
| Difficult anatomy | Relative contraindication | Preferred |
| Tracheal stenosis | Similar (0.16% meta-analysis) | Similar |
2.9 Complications
Acute
| Complication | Notes |
|---|---|
| Bleeding | Most common; avoid overlying vessels (USS guidance) |
| Posterior tracheal wall injury | Perforation → mediastinitis |
| Paratracheal placement / false tract | Life-threatening |
| Hypoxia during procedure | Minimize by increasing FiO₂ |
| Subcutaneous emphysema | |
| Pneumothorax / Pneumomediastinum | Manage conservatively unless expanding |
Late
| Complication | Notes |
|---|---|
| Tracheoinnominate Artery Fistula (TIF) | <1% incidence; 85% mortality; occurs 7–14 days post-op. Signs: sentinel bleed. DO NOT deflate cuff. Pack + OR for repair |
| Laryngotracheal stenosis | Clinically significant when >75% luminal reduction; stridor when diameter <5 mm |
| Tracheomalacia | From cuff pressure |
| Stomal infection / abscess | Antibiotics; surgical drainage if abscess |
| Accidental decannulation | Before tract matures (~7–10 days): oral intubation → redilate under control |
| Airway fire | Keep FiO₂ <0.4 during electrocautery |
TIF Management Mnemonic: "DCOR" Do NOT deflate cuff → Call surgeon immediately → OR for immediate repair → Resuscitate
PART 3 — SIDE-BY-SIDE QUICK COMPARISON TABLE
| Feature | Cricothyrotomy | Percutaneous Tracheostomy |
|---|---|---|
| Access site | CTM (larynx) | Trachea (rings 1–2 or 2–3) |
| Urgency | Emergency (CICO) | Semi-elective (ICU) |
| Tube size | 6.0 cuffed ETT or Shiley | Shiley 8.0 (standard) |
| Duration of use | Temporary (convert within 72 h) | Long-term |
| Ventilation quality | Full (surgical) / Oxygenation only (needle) | Full |
| Subglottic stenosis | Higher risk if prolonged | Lower risk (below glottis) |
| Main risk | Voice change, stenosis | TIF, posterior wall injury |
| Key anatomical hazard | Cricothyroid arteries (superior CTM) | Innominate artery (inferior/deep) |
| Success rate | 90–100% (surgeon); ~50% (needle by anaesthetist) | >95% (bronchoscopy-guided) |
PART 4 — CLINICAL SCENARIOS (DNB APPLICATION)
Scenario 1: CICO in a trauma patient with massive orofacial injuries
- Action: Immediate surgical cricothyrotomy (scalpel-bougie technique)
- Do NOT attempt repeated laryngoscopy or needle cricothyrotomy (inadequate CO₂ clearance)
- Convert to formal tracheostomy within 24–72 hours
Scenario 2: ICU patient, intubated 14 days, failed multiple weaning trials, TBI
- Action: PDT — USS-guided, bronchoscopy-assisted, Ciaglia Blue Rhino
- Check coagulation, palpate anatomy, PEEP assessment
Scenario 3: Post-PDT patient, day 9 — massive haemorrhage from tracheostomy
- Think TIF immediately
- DO NOT deflate cuff; apply digital pressure; call vascular/cardiothoracic surgery; OR for innominate artery ligation
PART 5 — DNB EXAM BULLET SUMMARY
Cricothyrotomy — High-Yield Points
- CTM = emergency airway of choice in CICO
- Dimensions: 9 mm × 30 mm; access in LOWER 1/3
- Relatively avascular — cricothyroid arteries at superior margin
- Contraindicated in age <5–12 years (use needle only)
- Success: 90–100% surgical; ~50% needle (by non-surgeon)
- Needle cricothyrotomy = temporising measure only — max 30–45 min
- Convert surgical cricothyrotomy to tracheostomy within 72 h
- Subglottic stenosis risk: historical overconcern; equivalent to tracheostomy with good technique
- Jackson (1921) overestimated risk → refuted by Brantigan & Grow (1976)
Percutaneous Tracheostomy — High-Yield Points
- PDT first described by Ciaglia (1985) — Ciaglia Blue Rhino = gold standard
- Ideal site: between rings 1–2 or 2–3
- Requires bronchoscopic guidance (reduces complications)
- USS neck pre-procedure to identify overlying vessels
- Timing: no proven mortality benefit early vs. late (TracMan trial)
- Most feared late complication: TIF (<1%; mortality ~86%)
- Tracheal stenosis: clinically significant only when >75% luminal reduction; stridor when <5 mm
- DDAVP pre-procedure in uraemic patients
- NOT for emergency airway access
- PDT complication rates equivalent to surgical tracheostomy when bronchoscope-guided
REFERENCES
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapters on Cricothyrotomy & Percutaneous Translaryngeal Ventilation
- Current Surgical Therapy, 14e — Thiboutot & Feller-Kopman, Percutaneous Dilatational Tracheostomy
- Miller's Anesthesia, 10e — Cricothyrotomy and PEAA
- Barash's Clinical Anesthesia, 9e — Emergency Airway Management
- Current Surgical Therapy 14e — Comparison: PDT vs. Surgical Tracheostomy
This is a shared conversation. Sign in to Orris to start your own chat.