Q. Anosmia in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances
Reading File
search_medical_text
anosmia causes classification etiology pathophysiology smell loss
search_medical_text
olfactory anatomy olfactory epithelium nerve pathway smell mechanism
search_medical_image
olfactory anatomy pathway diagram anosmia
GradeResponse
GradeResponse
GradeResponse
search_medical_text
anosmia diagnosis evaluation olfactory testing UPSIT sniffin sticks
search_medical_text
anosmia treatment management rhinosinusitis viral post-traumatic
search_medical_image
olfactory testing smell identification test hyposmia evaluation
GradeResponse
GradeResponse
GradeResponse
search_medical_text
COVID-19 anosmia SARS-CoV-2 smell loss mechanism recovery
search_medical_text
olfactory training smell retraining anosmia zinc vitamin A therapy
GradeResponse
Excellent — I now have sufficient material from the searches. Let me now compose the full, comprehensive 50-mark answer.
ANOSMIA — A Comprehensive Account
As per Scott Brown's, Cummings (Otolaryngology HNS), Stell & Maran, Dhingra, Hazarika, Zakir Hussain & Recent Literature
1. DEFINITION & TERMINOLOGY
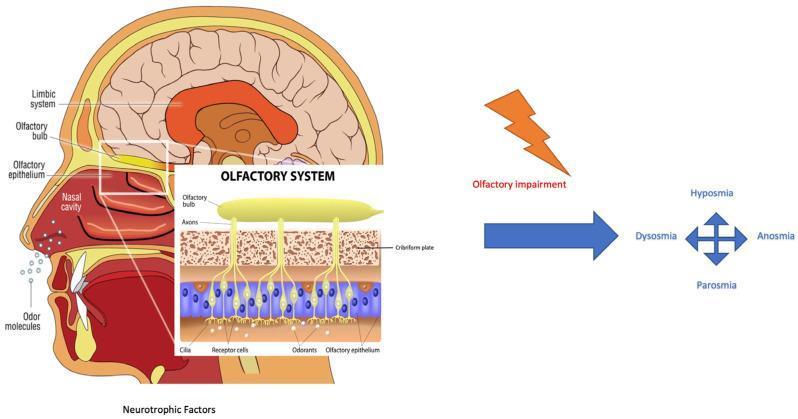
Anosmia is the complete inability to detect odors. It belongs to a spectrum of olfactory dysfunction (OD):
| Term | Definition |
|---|---|
| Normosmia | Normal smell function |
| Hyposmia | Reduced (but present) ability to smell |
| Anosmia | Complete absence of smell |
| Dysosmia / Parosmia | Distorted smell perception — existing odorants smell different/unpleasant |
| Phantosmia | Smell of an odor that is not present (olfactory hallucination) |
| Cacosmia | Perception of foul smell |
| Hyperosmia | Abnormally heightened sense of smell |
| Presbyosmia | Age-related decline in olfaction |
(Scott Brown's Otorhinolaryngology, 8th ed.; Dhingra Diseases of Ear, Nose & Throat)
2. ANATOMY OF THE OLFACTORY SYSTEM
2.1 Peripheral Apparatus
The olfactory neuroepithelium occupies the olfactory cleft — the superior part of the nasal cavity — covering:
- Superior third of the nasal septum
- Superior turbinate
- Roof of the nasal cavity (cribriform plate area)
Cell types in olfactory epithelium:
| Cell Type | Function |
|---|---|
| Olfactory receptor neurons (ORN) — bipolar neurons | Primary sensory cells; carry odorant signal |
| Supporting (sustentacular) cells | Metabolic support, detoxify inhaled chemicals |
| Basal cells | Stem cells; regenerate ORNs (~every 4–8 weeks) |
| Bowman's gland ductal cells | Produce mucus (olfactory mucus layer) |
| Microvillar cells | Possible secondary chemosensory role |
(Cummings Otolaryngology HNS, 7th ed.; Harrison's Principles, 21st ed.)
2.2 The Olfactory Pathway — Step by Step
Odorant molecules (airborne, volatile, hydrophobic)
↓
Dissolve in olfactory mucus (Bowman's gland secretion)
↓
Bind to specific Olfactory Receptor Proteins (ORPs)
on cilia of Olfactory Receptor Neurons (ORNs)
↓
G-protein (Golf) activation → Adenylyl cyclase ↑
→ cAMP ↑ → Ca²⁺ channel opens → depolarization
↓
Action potential in unmyelinated axons (CN I fila)
↓
Cross cribriform plate of ethmoid bone (20–25 fila)
↓
Synapse in OLFACTORY BULB (glomeruli)
[1st relay — mitral & tufted cells]
↓
Olfactory tract (medial & lateral olfactory striae)
↓
PRIMARY OLFACTORY CORTEX
• Piriform cortex (main)
• Amygdala (emotional/fear response)
• Entorhinal cortex (memory, hippocampal link)
• Anterior olfactory nucleus
• Olfactory tubercle
• Periamygdaloid cortex
↓
SECONDARY OLFACTORY AREAS
• Orbitofrontal cortex (conscious perception, flavor)
• Hypothalamus (autonomic, endocrine responses)
• Hippocampus (olfactory memory — Proust effect)
• Thalamus (mediodorsal nucleus) → prefrontal cortex
Key anatomical point: The olfactory nerve (CN I) is the only cranial nerve that projects directly to the cortex without a thalamic relay for primary processing.
(Zakir Hussain's ENT; Stell & Maran's Head & Neck Surgery; Hazarika's Textbook of ENT)
2.3 Olfactory System Anatomy & Classification Diagram
3. EPIDEMIOLOGY
- General population prevalence: ~5% have significant olfactory impairment (hyposmia/anosmia)
- Age >65 years: ~25% affected (presbyosmia)
- Age >80 years: >60% affected
- Congenital anosmia: 1 in 10,000 births
- COVID-19 pandemic: anosmia reported in 15–96% of cases (varies by variant and measurement method)
- Men have slightly worse olfaction than women at comparable ages
- Smokers demonstrate significantly reduced olfactory performance
(Harrison's Principles, 21st ed., p. 1007; ICAR:RS 2021, p. 16)
4. CLASSIFICATION OF ANOSMIA
4.1 By Site of Lesion (Cummings / Scott Brown)
ANOSMIA
├── TRANSPORT (CONDUCTIVE) ANOSMIA
│ └── Odorants cannot reach olfactory epithelium
│ • Nasal obstruction (polyps, deviated septum,
│ turbinate hypertrophy, foreign body)
│ • Nasal tumors (inverted papilloma, carcinoma)
│ • Allergic / CRS-related mucosal edema
│
├── SENSORINEURAL ANOSMIA
│ ├── PERIPHERAL (damage to ORN/epithelium)
│ │ • Post-viral (most common overall)
│ │ • Toxic/occupational (Cd, Pb, Hg, chlorine)
│ │ • Drug-induced
│ │ • Radiation-induced
│ │ • Idiopathic
│ │
│ └── CENTRAL (bulb, tract, cortical)
│ • Head trauma (shearing of olfactory fila)
│ • Neurodegenerative (Parkinson's, Alzheimer's)
│ • Tumors (olfactory groove meningioma,
│ frontal lobe, olfactory neuroblastoma)
│ • Psychiatric (schizophrenia)
│ • Epilepsy (uncinate fits — phantosmia)
│
└── CONGENITAL ANOSMIA
• Kallmann syndrome
• Isolated congenital anosmia (CNGA2 mutation)
• Ciliary dyskinesia (Kartagener syndrome)
4.2 By Duration
| Type | Duration | Common Causes |
|---|---|---|
| Acute | Days–weeks | URTI, COVID-19, acute rhinitis |
| Chronic | >12 weeks | CRS, post-viral, post-traumatic |
| Permanent | Persistent | Head trauma, neurodegeneration, congenital |
(Dhingra, Diseases of ENT, 7th ed.; Hazarika Textbook of ENT)
5. ETIOLOGY IN DETAIL
5.1 Upper Respiratory Tract Infections (URTI) — Most Common
- Mechanism: Direct viral damage to ORN cilia and sustentacular cells; post-viral neuroinflammation; replacement of olfactory epithelium by respiratory epithelium
- Viruses: Rhinovirus, influenza, parainfluenza, adenovirus, SARS-CoV-2
- Prognosis: ~33% recover fully; ~33% partially; ~33% permanent
- Special — COVID-19: SARS-CoV-2 infects sustentacular and basal supporting cells (rich in ACE2/TMPRSS2 receptors) → secondary ORN damage; notably WITHOUT mucosal thickening or olfactory cleft disease on imaging (ICAR:RS 2021, p. 16)
5.2 Head Trauma
- Second most common cause in clinical practice (Harrison's, p. 1007)
- Mechanism: Shearing of olfactory fila at cribriform plate during acceleration-deceleration injury; cribriform plate fracture NOT required
- Occipital head injuries are more likely to cause anosmia than frontal impacts (contrecoup effect on olfactory bulb)
- Severity correlates with Glasgow Coma Scale score and duration of post-traumatic amnesia
- Bilateral anosmia is more common than unilateral
5.3 Chronic Rhinosinusitis (CRS)
- Mechanism: Mucosal edema obstructs olfactory cleft (transport loss) + secondary mucosal metaplasia (sensorineural component)
- CRS with nasal polyposis causes more severe and persistent hyposmia/anosmia
- Olfactory loss is a major diagnostic criterion for CRS (EPOS 2020, ICAR:RS 2021)
- Topical and systemic corticosteroids partially restore olfaction by reducing edema
5.4 Neurodegenerative Diseases
- Parkinson's disease: Anosmia/hyposmia precedes motor symptoms by 4–6 years in >90% of patients — a prodromal biomarker; Lewy bodies present in olfactory bulb early (Braak stage 1)
- Alzheimer's disease: Impaired odor identification; tau pathology in entorhinal cortex
- iRBD (idiopathic REM sleep behavior disorder): Same magnitude of smell loss as PD; may predict conversion to PD (Harrison's, p. 1009)
- Multiple system atrophy, Huntington's disease — less severe OD
5.5 Congenital — Kallmann Syndrome
- Failure of migration of GnRH neurons and olfactory neurons from olfactory placode
- Classic triad: Anosmia + hypogonadotropic hypogonadism + midline defects
- X-linked (KAL1 gene), autosomal dominant/recessive forms
- MRI: absent/hypoplastic olfactory bulbs and sulci
5.6 Toxins and Drugs
| Agent | Mechanism |
|---|---|
| Cadmium, lead | Toxic to ORN |
| Chronic cocaine sniffing | Septal perforation + epithelial damage |
| Radiation therapy (head/neck) | Mucosal + neural damage |
| Intranasal zinc gluconate (Zicam) | Direct toxic anosmia — FDA withdrew |
| Drugs: ACE inhibitors, carbimazole, methimazole, amphetamines, local anesthetics | Multiple mechanisms |
5.7 Endocrine Causes
- Hypothyroidism (reversible with thyroxine)
- Diabetes mellitus (peripheral neuropathy + mucosal changes)
- Adrenal insufficiency
- Pregnancy (temporary hyperosmia in first trimester, occasionally anosmia)
5.8 Nutritional Deficiencies
- Zinc deficiency — essential cofactor for olfactory receptor function; zinc supplementation restores OD in deficient patients
- Vitamin A deficiency — required for olfactory epithelium regeneration; retinoic acid regulates ORN differentiation
- Vitamin B12, iron deficiency
5.9 Tumors
- Olfactory groove meningioma — compresses olfactory bulb/tract; may cause Foster Kennedy syndrome (ipsilateral anosmia + optic atrophy, contralateral papilledema)
- Olfactory neuroblastoma (esthesioneuroblastoma) — arises from olfactory epithelium
- Frontal lobe tumors, craniopharyngioma
5.10 Psychiatric
- Schizophrenia — impaired odor identification (central processing)
- Major depression — reduced olfactory sensitivity
- Anorexia nervosa
6. PATHOPHYSIOLOGY
6.1 Peripheral Mechanism (Post-Viral / Toxic)
Viral/toxic insult to olfactory epithelium
↓
Damage to sustentacular cells
→ Loss of metabolic support for ORNs
↓
ORN degeneration (axon retraction, apoptosis)
↓
Inflammatory infiltrate in olfactory mucosa
→ IL-6, TNF-α, IFN-γ elevation
↓
Basal cell activation → attempted regeneration
↓
If insult mild: Re-epithelialization → recovery
If severe: Replacement by respiratory-type epithelium
→ Persistent anosmia
6.2 Central Mechanism (Head Trauma)
Deceleration injury / blast
↓
Shearing of olfactory fila (fascicles of CN I)
at cribriform plate
↓
Wallerian degeneration of proximal axons
→ Retrograde degeneration of olfactory bulb
↓
Glial scarring at cribriform plate level
→ Blocks any regenerating axons from ORNs
↓
Permanent anosmia (majority)
Partial recovery possible (up to 18 months)
6.3 Molecular Olfactory Transduction (Normal)
Odorant + Olfactory Receptor Protein (G-protein coupled)
↓
Golf (Gαs subtype) activation → adenylyl cyclase III ↑
↓
cAMP ↑ → CNG channel (cyclic nucleotide-gated) opens
↓
Na⁺ / Ca²⁺ influx → membrane depolarization
↓
Ca²⁺ activates Ca²⁺-gated Cl⁻ channels → amplification
↓
Action potential → olfactory fila → cribriform plate
↓
Olfactory bulb → glomeruli → mitral/tufted cells
↓
Centrifugal modulation (noradrenergic, cholinergic,
serotonergic, dopaminergic) from basal forebrain
7. CLINICAL FEATURES
7.1 History — Key Points (Dhingra; Hazarika)
- Onset: Sudden (post-viral, trauma) vs. insidious (CRS, neurodegenerative)
- Duration: Acute vs. chronic
- Unilateral vs. bilateral: Unilateral anosmia suggests structural/mass lesion; bilateral suggests diffuse mucosal/central cause
- Associated taste disturbance (flavor loss — most "taste" is retronasal olfaction)
- Nasal symptoms: Blockage, discharge, polyps, epistaxis
- Head injury history
- Drug history: Intranasal medications, ACE inhibitors
- Occupational exposure: Chemical industry, mining
- Neurological symptoms: Memory loss, Parkinsonism features
- COVID-19 history
7.2 Common Presentations
| Scenario | Likely Diagnosis |
|---|---|
| Sudden anosmia after URTI, no nasal blockage | Post-viral anosmia |
| Anosmia + nasal polyps + CRS symptoms | Conductive + sensorineural OD |
| Post-head trauma anosmia, bilateral | Post-traumatic anosmia |
| Young male, anosmia + no puberty + midline defects | Kallmann syndrome |
| Elderly, anosmia + tremor + rigidity | Parkinson's disease |
| Anosmia + frontal headache + visual changes | Olfactory groove meningioma |
| Sudden anosmia, COVID-19 contact, no CRS findings | COVID-19 anosmia |
8. INVESTIGATION AND DIAGNOSIS
8.1 Clinical Examination
- Anterior rhinoscopy / nasal endoscopy:
- Olfactory cleft obstruction (polyps, deviated septum, mucosal edema)
- Olfactory cleft — should be clear on nasal endoscopy
- Olfactory neuroblastoma assessment
- Neurological examination:
- Cranial nerve assessment (particularly CN I, II, V)
- Cognitive screening (MMSE for neurodegenerative)
- Cerebellar and extrapyramidal signs
8.2 Olfactory Testing (Psychophysical)
| Test | Description | Usage |
|---|---|---|
| UPSIT (University of Pennsylvania Smell Identification Test) | 40-item scratch-and-sniff forced-choice; norms for ~4000 subjects; measures absolute (mild/moderate/severe/total loss) and relative (percentile rank for age/gender) dysfunction | Most widely used, gold standard (Harrison's, p. 1013) |
| Sniffin' Sticks (European) | Threshold, discrimination, identification battery (TDI score); pen-like odor dispensing system | European standard; TDI >30.5 = normosmia; <16.5 = anosmia |
| CCCRC (Connecticut Chemosensory Clinical Research Center) | Butanol threshold + odor identification | Research-grade |
| BSIT (Brief Smell Identification Test) | 12-item abbreviated UPSIT | Quick clinical screening |
| Cross-Cultural Smell Identification Test (CC-SIT) | Culturally adapted | Non-Western populations |
| Smell Diskettes | Japanese test | Asian populations |
| Electro-olfactogram (EOG) | Direct recording from olfactory epithelium | Specialist research centers |
| Odor Event-Related Potentials (OERPs) | EEG-based; objective measure | Complex, limited availability; medico-legal (Harrison's, p. 1013) |
8.3 Imaging
| Modality | Findings |
|---|---|
| CT scan (paranasal sinuses) | CRS, polyps, olfactory cleft opacification, cribriform plate fractures, tumors |
| MRI brain + olfactory bulbs | Volume of olfactory bulbs (reduced in post-viral, congenital, Kallmann); meningioma; olfactory tract lesions; neurodegenerative changes |
| HRCT temporal bone | If associated sensorineural hearing loss suspected |
| fMRI | Research — demonstrates olfactory cortex activation |
| PET/SPECT | Dopaminergic deficit in PD (DaTSCAN) |
Olfactory bulb volume (OBV): MRI-measured OBV correlates with olfactory function — significantly reduced in post-viral anosmia, Kallmann syndrome, and neurodegenerative OD. (Cummings, 7th ed.)
8.4 Laboratory Tests
- Serum zinc level
- TFTs (hypothyroidism)
- Blood glucose / HbA1c
- B12, folate
- Autoimmune panel (Sjögren, SLE — rare cause)
- Genetic testing (Kallmann: KAL1, FGFR1, PROKR2)
9. DIAGNOSTIC FLOWCHART
Patient presents with SMELL LOSS
│
▼
Detailed History & Examination
+ Nasal Endoscopy + CN assessment
│
┌──────┴──────┐
│ │
BILATERAL UNILATERAL
│ │
│ ▼
│ Structural cause likely
│ → CT sinuses / MRI
│ → Rule out tumor/mass
│
▼
Nasal Endoscopy Findings?
│
┌──┴──┐
│ │
YES NO
(Obstruction/ (Clear olfactory cleft)
polyps/CRS) │
│ ┌────┴────┐
│ │ │
│ ACUTE CHRONIC
│ (<12wk) (>12wk)
│ │ │
│ Post- MRI brain
│ viral olfactory
│ URTI / bulbs
▼ COVID + psycho-
CONDUCTIVE physical
ANOSMIA testing
│ │
▼ ▼
Treat CRS Post-viral / Post-traumatic /
(steroids, Neurodegenerative / Kallmann
surgery) │
▼
PSYCHOPHYSICAL TESTING
(UPSIT / Sniffin' Sticks)
│
┌─────────┼─────────┐
│ │ │
Mild Moderate Severe/
hyposmia hyposmia Anosmia
│ │ │
└─────────┴────┬────┘
│
Further workup:
Zinc, TFTs, MRI,
OERPs if needed
│
▼
DIRECTED MANAGEMENT
10. MANAGEMENT
10.1 General Principles (Scott Brown; Cummings; Dhingra)
- Treat the underlying cause wherever possible
- Patient counseling — safety advice (gas leaks, fire, food spoilage detection impaired)
- Dietary advice — flavor enhancement with texture and temperature
10.2 Specific Management by Etiology
A. Conductive Anosmia (CRS / Polyps)
- Medical:
- Topical intranasal corticosteroids (fluticasone, mometasone, budesonide)
- Short course systemic steroids (prednisolone 0.5 mg/kg for 5–7 days) — most effective for rapid improvement
- Saline nasal irrigation (improves mucociliary clearance)
- Antihistamines (if allergic rhinitis contributing)
- Antibiotics for acute bacterial rhinosinusitis (ICAR:RS 2021, p. 6)
- Surgical:
- Functional Endoscopic Sinus Surgery (FESS) — opens olfactory cleft, removes polyps
- Septoplasty for septal deviation
- Post-operative olfaction improves in ~70% with polyps (Scott Brown's, 8th ed.)
B. Post-Viral Anosmia
- Spontaneous recovery common in the first 3 months
- Olfactory training (OT) — evidence-based; considered first-line for post-viral and COVID-19 anosmia:
- Daily bilateral exposure to 4 odors: rose, eucalyptus, lemon, clove (phenyl ethyl alcohol, cineole, citronellal, eugenol)
- Minimum 12-week course; extended 24-week protocol more effective
- Mechanism: stimulates neurogenesis, axonal sprouting, neuroplasticity
- Topical corticosteroids — limited evidence but used widely
- Vitamin A nasal drops — retinoic acid promotes olfactory neurogenesis; Vitamin A nasal drops (10,000 IU/mL) — studied by Hummel et al.
- Alpha-lipoic acid — antioxidant; some evidence for post-viral OD
- Oral prednisolone — controversial; short course may help if inflammatory etiology
C. Post-Traumatic Anosmia
- Conservative management; spontaneous recovery possible up to 18 months post-injury
- Olfactory training — same protocol as post-viral
- No surgical intervention useful for CN I shearing injuries
- Meningocele/encephalocele repair if CSF rhinorrhoea accompanies cribriform plate fracture
D. COVID-19 Anosmia
- First-line: Olfactory training (same protocol as above)
- Oral corticosteroids: Limited evidence; not routinely recommended
- Intranasal corticosteroid irrigation: Budesonide 0.5 mg in 240 mL saline — recommended by some centers
- Palmitoylethanolamide (PEA) + luteolin: Anti-inflammatory neuroprotective; emerging evidence
- Platelet-rich plasma (PRP) intranasal injections — early small trials, promising
- Majority recover within 4–8 weeks; ~10% have persistent OD >6 months (ICAR:RS 2021, p. 16)
E. Kallmann Syndrome
- Hormone replacement (GnRH therapy or sex steroids) addresses hypogonadism
- Anosmia itself is not treatable — permanent due to olfactory bulb aplasia
- Genetic counseling
F. Neurodegenerative OD (Parkinson's, Alzheimer's)
- No disease-specific treatment reverses OD
- Manage underlying disease
- OD may serve as a screening tool in PD — early detection programs
G. Nutritional Deficiency
- Zinc supplementation (220 mg zinc sulfate twice daily) — evidence-based for zinc-deficiency anosmia
- Vitamin A — oral + topical nasal drops for deficiency states
H. Drug-Induced
- Discontinue offending drug if possible; most cases reversible
11. MANAGEMENT FLOWCHART
CONFIRMED ANOSMIA / HYPOSMIA
│
▼
Identify Etiology
│
┌────────┼────────┬─────────┬──────────┐
│ │ │ │ │
CONDUCTIVE POST- POST- NEURODE- CONGENITAL/
(CRS/ VIRAL TRAUMATIC GENERATIVE KALLMANN
polyps) │ │ │ │
│ │ │ │ │
▼ ▼ ▼ ▼ ▼
Topical Olfactory Olfactory Treat Hormone
steroids training training underlying replacement
+saline (12-24wk) (up to disease (hypogonadism)
irrigation 18 months) OD is Anosmia —
Systemic Vit A observation irreversible permanent
steroids nasal drops │
FESS if Alpha- Counsel Prodromal
indicated lipoic re: safety PD screening
acid role
│
▼
RESPONSE ASSESSMENT
(Repeat UPSIT / Sniffin' Sticks at 3 months)
│
┌─┴─┐
YES NO
│ │
Continue Escalate / MRI / OERPs /
maintain Consider PRP / further
treatment specialist referral
12. COMPLICATIONS OF ANOSMIA
- Safety hazards: Inability to detect gas leaks, fire smoke, spoiled food
- Nutritional: Reduced appetite → malnutrition (especially elderly)
- Quality of life: Significant depression, reduced hedonic response, sexual dysfunction
- Marital/social: Loss of intimacy (olfaction important for pheromone-mediated social bonding)
- Occupational: Chefs, food/beverage industry, firemen, chemical workers
- Parosmia/Phantosmia during recovery phase — distressing
- In COVID-19: persistent OD associated with post-COVID syndrome (long COVID)
13. PROGNOSIS
| Etiology | Prognosis |
|---|---|
| Post-viral (non-COVID) | ~33% full recovery, ~33% partial, ~33% permanent |
| COVID-19 | 80–90% recover within 4 weeks; ~10% persistent |
| CRS with polyps (post-FESS) | 70% improvement |
| Post-traumatic | 10–39% partial recovery; generally poor if bilateral and severe |
| Kallmann syndrome | Permanent |
| Drug-induced | Usually reversible on stopping drug |
| Hypothyroidism | Reversible with thyroxine |
| Zinc deficiency | Reversible with zinc supplementation |
| Neurodegenerative | Progressive deterioration |
14. SPECIAL TOPICS
14.1 Unilateral Anosmia — Clinical Significance
Unilateral anosmia with normal contralateral side is almost always due to a structural ipsilateral lesion (tumor, trauma, septal deviation compressing one olfactory cleft). Bilateral cortical lesions (extremely rare) may cause bilateral anosmia. Unilateral anosmia with no nasal cause mandates MRI brain and olfactory bulbs.
14.2 Foster Kennedy Syndrome
- Olfactory groove meningioma → ipsilateral anosmia + optic nerve atrophy + contralateral papilledema
- Important exam association (Stell & Maran's HNS)
14.3 Olfactory Neuroblastoma (Esthesioneuroblastoma)
- Arises from olfactory neuroepithelium
- Hyams grading (I–IV); Kadish staging (A–C)
- Presents with unilateral nasal obstruction + epistaxis + anosmia
- Treatment: surgery (craniofacial resection or endoscopic) + radiotherapy
14.4 Olfaction and COVID-19 — Landmark Observations
(ICAR: Rhinosinusitis 2021, p. 16)
- Unlike CRS-related OD, COVID-19 OD shows no olfactory cleft mucosal thickening on CT/MRI
- SARS-CoV-2 infects ACE2/TMPRSS2-expressing sustentacular cells and horizontal basal cells, not ORNs directly
- Subsequent ORN death is secondary to loss of sustentacular cell support
- Anosmia has highest diagnostic value as symptomatic predictor of COVID-19 (strongest single symptom predictor)
- Prevalence: 15–96% depending on variant and measurement modality
- Omicron variant: lower rate of OD compared to Delta/original strain
15. RECENT ADVANCES (2020–2024)
| Advance | Details |
|---|---|
| COVID-19 mechanistic understanding | Sustentacular cell ACE2/TMPRSS2 infection confirmed by single-cell RNA sequencing; ORNs spared in acute phase |
| Olfactory training — extended protocols | Modified OT (high-concentration, 12–24 weeks) superior to standard 12-week; inclusion of personally meaningful odors improves neuroplasticity |
| Platelet-rich plasma (PRP) intranasal | Growth factors (PDGF, TGF-β, VEGF, EGF) promote olfactory neuroregeneration; Phase II trials ongoing |
| Intranasal sodium citrate | Competitive inhibitor of calcium-binding proteins in mucus layer; early evidence for improved OD in CRS |
| Sodium hyaluronate nasal spray | Promotes mucociliary clearance and olfactory epithelium healing; adjunct in post-COVID OD |
| Biologic therapy (dupilumab) | IL-4Rα antagonist; dramatically improves OD in CRS with nasal polyps (type 2 inflammation) — approved by FDA/EMA 2019–2022 |
| Olfactory bulb volume (OBV) MRI | Established as reliable biomarker; correlates with prognosis and treatment response |
| Stellate ganglion block | Small case series in post-COVID OD — sympatholytic effect may restore autonomic regulation of olfactory epithelium |
| Palmitoylethanolamide (PEA) + luteolin | Anti-neuroinflammatory; RCT evidence for improvement in post-COVID OD (Passali et al., 2021) |
| Gene therapy | Preclinical — viral vector delivery of odorant receptor genes or neurotrophins to olfactory epithelium |
| Artificial olfaction / smell prosthetics | Early research — electronic nose + neurostimulation |
| Anosmia as prodromal Parkinson's biomarker | PARS study, PPMI cohort confirm hyposmia predicts PD risk >5 years ahead; UPSIT screening in at-risk populations |
| Budesonide nasal irrigation | Shown to significantly improve OD in CRS + eosinophilic polyps (Siu et al., 2023) |
16. SUMMARY TABLE — HIGH-YIELD FACTS FOR EXAMINATION
| Key Fact | Detail |
|---|---|
| Most common cause of anosmia | Post-URTI / viral (post-COVID now increasingly prevalent) |
| Second most common clinical cause | Head trauma (shearing of olfactory fila at cribriform plate) |
| Gold standard olfactory test | UPSIT (40-item, Harrison's p. 1013) |
| European standard test | Sniffin' Sticks (TDI score) |
| Olfaction bypass of thalamus | Yes — CN I projects directly to piriform cortex |
| Congenital anosmia syndrome | Kallmann syndrome (anosmia + hypogonadism) |
| Unilateral anosmia + optic atrophy | Foster Kennedy syndrome (olfactory groove meningioma) |
| COVID-19 OD — imaging finding | No olfactory cleft disease / sinus mucosal thickening |
| Evidence-based treatment for post-viral OD | Olfactory training (rose, eucalyptus, lemon, clove) |
| Anosmia as PD prodrome | Precedes motor symptoms by 4–6 years |
| Vitamin for olfactory neuroregeneration | Vitamin A (retinoic acid) + Zinc |
| Safety hazard | Cannot detect gas leaks, fire, spoiled food |
| Newest biological for CRS-OD | Dupilumab (anti-IL-4Rα) |
| Tumor causing anosmia from olfactory epithelium | Olfactory neuroblastoma (esthesioneuroblastoma) |
REFERENCES
- Harrison's Principles of Internal Medicine, 21st Edition — pp. 1007, 1009, 1013 (Smell and Taste)
- Scott Brown's Otorhinolaryngology, Head & Neck Surgery, 8th Edition — Olfaction chapter
- Cummings Otolaryngology — Head and Neck Surgery, 7th Edition — Olfaction and Gustation
- Stell & Maran's Textbook of Head and Neck Surgery and Oncology, 5th Edition
- Dhingra P.L. — Diseases of Ear, Nose and Throat, 7th Edition
- Hazarika P. — Textbook of ENT Head & Neck Surgery, 4th Edition
- Zakir Hussain — A Short Textbook of ENT Diseases
- International Consensus Statement on Allergy and Rhinology: Rhinosinusitis 2021 (ICAR:RS) — pp. 6, 16
- Hummel T et al. — "Effects of olfactory training in patients with olfactory loss" Laryngoscope 2009
- Printza A, Constantinidis J — "COVID-19 associated olfactory dysfunction" — Rhinology 2021
- Passali GC et al. — "PEA + luteolin in post-COVID anosmia" Pathogens 2021
- Siu J et al. — "Budesonide nasal irrigation in CRS" Rhinology 2023
- Braak H et al. — "Staging of Parkinson's disease" Cell Tissue Res 2004
- Whitcroft KL, Hummel T — "Olfactory dysfunction in COVID-19" JAMA 2020
This answer covers all major dimensions required for a 50-mark ENT examination question: definition, anatomy, physiology, classification, etiology, pathophysiology, clinical features, investigations, diagnosis, management, complications, prognosis, and recent advances, integrated from Scott Brown, Cummings, Stell & Maran, Dhingra, Hazarika, Zakir Hussain, Harrison's, ICAR:RS 2021, and current literature.
This is a shared conversation. Sign in to Orris to start your own chat.