Q. Surgical approaches to pterygopalatine Fossa in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances
Reading File
search_medical_text
pterygopalatine fossa surgical approaches anatomy
search_medical_text
pterygopalatine fossa endoscopic transnasal approach
search_medical_image
pterygopalatine fossa anatomy diagram surgical approaches
GradeResponse
GradeResponse
GradeResponse
search_medical_text
pterygopalatine fossa infratemporal fossa approaches ENT surgery
search_medical_text
transmaxillary approach pterygopalatine fossa tumor resection
search_medical_image
endoscopic endonasal pterygopalatine fossa dissection
GradeResponse
GradeResponse
GradeResponse
Now I have sufficient material to compose a comprehensive 50-mark answer. Let me construct the full detailed response.
Surgical Approaches to the Pterygopalatine Fossa (PPF)
A Comprehensive 50-Mark Answer
1. INTRODUCTION
The pterygopalatine fossa (PPF) — also called the sphenopalatine fossa or pterygo-maxillary fossa — is one of the most strategically significant, anatomically complex, and surgically challenging spaces in the head and neck. It serves as a crossroads for the second division of the trigeminal nerve, the terminal internal maxillary artery, and the pterygopalatine ganglion. Pathology here includes juvenile nasopharyngeal angiofibroma (JNA), nerve sheath tumors, meningiomas, perineural spread of malignancy, and vascular anomalies. Access to this fossa requires a thorough understanding of its three-dimensional boundaries and the multiple surgical corridors that converge upon it.
2. SURGICAL ANATOMY OF THE PPF
(Cummings Otolaryngology – Head and Neck Surgery, 7th Ed; Scott-Brown's Otorhinolaryngology, 8th Ed)
2.1 Boundaries
| Wall | Structure |
|---|---|
| Anterior | Posterior surface of the maxillary sinus (posterior maxillary wall) |
| Posterior | Pterygoid process (base of sphenoid) and greater wing of sphenoid |
| Medial | Perpendicular plate of palatine bone (opening into nasal cavity via sphenopalatine foramen) |
| Superior | Body of sphenoid and orbital process of palatine bone |
| Lateral | Pterygomaxillary fissure (communicates with infratemporal fossa) |
| Inferior | Palatovaginal canal (open, narrows to pterygopalatine canal) |
2.2 Communications (Critical for Surgical Planning)
┌─────────────────────────────────┐
│ PTERYGOPALATINE FOSSA │
└────────────┬────────────────────┘
┌─────────────┬────────────┼──────────────┬──────────────┐
▼ ▼ ▼ ▼ ▼
Nasal Cavity Middle Cranial Orbit Infratemporal Oral Cavity
(Sphenopalatine Fossa (Inferior Fossa (Pterygopalatine
Foramen) (Foramen Orbital (Pterygo- Canal →
Rotundum, Fissure) maxillary Greater &
Vidian Canal) Fissure) Lesser
Palatine For.)
2.3 Contents
-
Arterial: Third (pterygopalatine) part of the maxillary artery and its branches:
- Sphenopalatine artery (→ nasal cavity)
- Descending palatine artery (→ palate)
- Infraorbital artery (→ orbit)
- Posterior superior alveolar artery
- Pharyngeal artery
- Artery of pterygoid canal (Vidian artery)
-
Neural:
- Maxillary nerve (V2) entering via foramen rotundum → gives infraorbital nerve, zygomatic nerve, and ganglionic branches
- Pterygopalatine ganglion (parasympathetic ganglion of CN VII via Greater Petrosal Nerve; sensory from V2; sympathetic from deep petrosal nerve)
- Nerve of pterygoid canal (Vidian nerve) = Greater Petrosal + Deep Petrosal nerves
-
Venous: pterygoid venous plexus (via pterygomaxillary fissure)
3. FLOWCHART: DECISION MAKING IN PPF SURGERY
┌────────────────────────────────────┐
│ SUSPECTED PPF PATHOLOGY │
│ (tumor / neuralgia / epistaxis) │
└────────────────┬───────────────────┘
│
┌───────────────▼──────────────────┐
│ High-Resolution CT + MRI (3T) │
│ + Angiography (if vascular) │
└───────────────┬──────────────────┘
│
┌──────────────────────▼─────────────────────────┐
│ ASSESS EXTENT OF DISEASE │
└────┬──────────────┬───────────────┬────────────┘
│ │ │
┌───────▼──────┐ ┌────▼──────┐ ┌─────▼──────────────┐
│ Confined to │ │Extension │ │ Extension into │
│ PPF only │ │to ITF / │ │ middle cranial │
│ │ │Orbit │ │ fossa / cavernous │
└───────┬──────┘ └────┬──────┘ │ sinus │
│ │ └─────┬──────────────┘
│ │ │
┌────────────▼─┐ ┌─────────▼──────┐ ┌──▼──────────────────┐
│ Endoscopic │ │ Endoscopic + │ │ Combined Open + │
│ Endonasal │ │ Transmaxillary │ │ Endoscopic / Cranio │
│ (EEA) │ │ or Caldwell-Luc│ │ -facial approach │
└──────────────┘ └───────────────┘ └─────────────────────┘
4. CLASSIFICATION OF SURGICAL APPROACHES
Surgical approaches to the PPF can be broadly classified as:
APPROACHES TO PTERYGOPALATINE FOSSA
│
├── A. ENDOSCOPIC APPROACHES
│ ├── 1. Endoscopic Endonasal Approach (EEA) / Transnasal
│ └── 2. Endoscopic Transmaxillary (Transantral) Approach
│
├── B. OPEN APPROACHES
│ ├── 3. Transantral Approach (Caldwell-Luc)
│ ├── 4. Transpalatal Approach
│ ├── 5. Midfacial Degloving
│ ├── 6. Lateral Rhinotomy + Medial Maxillectomy
│ └── 7. Total Maxillectomy (infrastructure / total)
│
├── C. SKULL BASE / COMBINED APPROACHES
│ ├── 8. Infratemporal Fossa Approaches (Fisch Types A-D)
│ ├── 9. Preauricular Subtemporal Approach (Al-Mefty)
│ ├── 10. Transcranial Approach (middle fossa floor)
│ └── 11. Combined Cranio-Endoscopic Approaches
│
└── D. MINIMALLY INVASIVE / PERCUTANEOUS
└── 12. Image-guided PPF nerve block / trigeminal neuralgia treatment
5. DETAILED DESCRIPTION OF EACH APPROACH
APPROACH 1: ENDOSCOPIC ENDONASAL APPROACH (EEA) / TRANSNASAL APPROACH
(Scott-Brown 8th Ed; Cummings 7th Ed; Hazarika ENT; Recent Advances – Kassam et al., 2011)
Indications:
- Sphenopalatine artery ligation (uncontrolled epistaxis)
- Vidian neurectomy (vasomotor rhinitis)
- Biopsy of PPF lesions
- JNA confined to PPF/nasal cavity (Radkowski Grade I–IIA)
- Pterygopalatine ganglion neuralgia (surgical approach)
Principle: The medial wall of the PPF (palatine bone with sphenopalatine foramen) is accessed through the nasal cavity after a middle meatal antrostomy or wide sphenopalatine foramen dissection.
Step-by-step Technique:
ENDOSCOPIC ENDONASAL APPROACH – OPERATIVE STEPS
│
├── STEP 1: Patient positioning
│ └── Supine, 15–20° reverse Trendelenburg, head turned 15° toward surgeon
│
├── STEP 2: Decongestion + Anesthesia
│ └── Topical xylometazoline + submucosal local anesthetic with epinephrine
│
├── STEP 3: Identify anatomical landmarks
│ └── Middle turbinate, uncinate process, natural maxillary ostium,
│ posterior wall of maxillary sinus, crista ethmoidalis
│
├── STEP 4: Crista ethmoidalis identification
│ └── Bony crest on posterior maxillary wall just anterior to
│ sphenopalatine foramen; key landmark
│
├── STEP 5: Mucosal incision
│ └── Vertical incision over lateral nasal wall posterior to
│ the attachment of the middle turbinate
│
├── STEP 6: Sphenopalatine foramen identification
│ └── Just posterior to crista ethmoidalis at level of posterior
│ maxillary fontanelle
│
├── STEP 7: Entry into PPF
│ └── Remove posterior wall of maxillary sinus (posterior antrostomy)
│ or directly widen sphenopalatine foramen with Kerrison punch
│
├── STEP 8: Identify sphenopalatine artery / maxillary artery
│ └── Clips / bipolar cautery applied to SPA for epistaxis ligation
│
└── STEP 9: Vidian canal identification (if neurectomy planned)
└── Floor of sphenoid sinus → Vidian canal at junction of
pterygoid process and sphenoid body
Advantages: No external incision, minimal morbidity, short hospital stay, excellent visualization with 0° and 30° endoscopes, ability to perform bimanual dissection with 4-hand technique.
Limitations: Limited lateral access, risk of injury to maxillary artery branches, steep learning curve, not suitable for large tumors with lateral extension.
APPROACH 2: ENDOSCOPIC TRANSMAXILLARY (TRANSANTRAL) APPROACH
(Cummings 7th Ed; Stell and Maran's Head and Neck Surgery)
Indications:
- JNA with extension into pterygomaxillary fissure and ITF
- Nerve sheath tumors of V2
- Schwannomas of PPF
- Perineural spread evaluation along V2
Principle: The posterior wall of the maxillary sinus (antral wall) is removed to access the PPF from the anterior aspect, providing the widest anterior corridor.
Technique:
ENDOSCOPIC TRANSMAXILLARY APPROACH – OPERATIVE STEPS
│
├── STEP 1: Wide middle meatal antrostomy (Caldwell-Luc incision or endoscopic)
│
├── STEP 2: Identify posterior wall of maxillary sinus
│ └── Corresponds to the anterior wall of PPF
│
├── STEP 3: Remove posterior antral wall
│ └── Using drill, Kerrison punch, or microdebrider
│ → Creates wide anterolateral corridor into PPF
│
├── STEP 4: Identify fat pad of PPF (characteristic yellow fat)
│ └── Confirms entry; contains maxillary artery and V2
│
├── STEP 5: Identify and control maxillary artery
│ └── Artery is superficial (anterior) to V2
│ Ligate or clip branches selectively
│
├── STEP 6: Trace V2 nerve
│ └── Nerve travels superomedially to foramen rotundum
│
├── STEP 7: Vidian nerve identification
│ └── Drill pterygoid process to expose Vidian canal
│
└── STEP 8: Tumor removal / biopsy / ligation
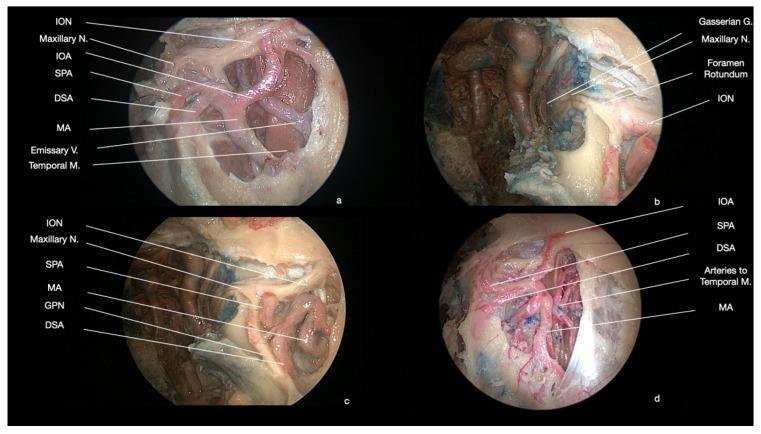
Intraoperative image (endoscopic dissection of PPF showing neurovascular planes):
APPROACH 3: TRANSANTRAL APPROACH (CALDWELL-LUC)
(Dhingra Diseases of ENT, 7th Ed; Hazarika Clinical ENT; Zakir Hussain ENT)
Indications (Historic/current):
- Classic open approach to PPF
- Maxillary artery ligation for epistaxis
- Drainage of PPF abscess
- Biopsy of posterolateral maxillary sinus / PPF tumors
Technique:
CALDWELL-LUC APPROACH – OPERATIVE STEPS
│
├── STEP 1: Incision
│ └── Horizontal sublabial incision in gingivobuccal sulcus
│ (above upper premolars, 0.5 cm above gingival margin)
│
├── STEP 2: Elevation of mucoperiosteal flap
│ └── Subperiosteal dissection to expose anterior maxillary wall
│ Preserve infraorbital nerve (exits infraorbital foramen)
│
├── STEP 3: Antrostomy
│ └── Perforation with osteotome or drill in canine fossa area
│ Enlarge with Kerrison punch (minimum 2 × 2 cm window)
│
├── STEP 4: Exploration of maxillary sinus
│ └── Identify posterior sinus wall
│
├── STEP 5: Breach posterior antral wall
│ └── Reveals PPF fat pad
│
├── STEP 6: Identify maxillary artery
│ └── Clip / ligate for epistaxis management
│
└── STEP 7: Closure
└── Primary closure of mucosal flap; nasal antrostomy for drainage
Important anatomical note (Dhingra): The infraorbital nerve exits the infraorbital foramen approximately 0.5–1 cm below the infraorbital rim at the midpupillary line — must be preserved during flap elevation.
Advantages: Wide access, familiarity, does not require specialized equipment.
Disadvantages: External scarring (if extended), risk of infraorbital nerve injury, post-operative cheek numbness, risk of oro-antral fistula. Largely superseded by endoscopic approaches.
APPROACH 4: TRANSPALATAL APPROACH
(Zakir Hussain ENT; Scott-Brown 8th Ed)
Indications:
- PPF lesions extending inferiorly toward pterygopalatine canal
- Selected cases of nasopharyngeal angiofibroma with inferior extension
- Access to pterygoid plates and posterior nasal choanae
Technique:
TRANSPALATAL APPROACH – STEPS
│
├── STEP 1: Palatal incision
│ └── Midline palatal incision from posterior hard palate edge
│ or U-shaped incision based on greater palatine vessels
│
├── STEP 2: Elevation of palatal mucoperiosteum
│ └── Preserve greater and lesser palatine neurovascular bundles
│
├── STEP 3: Drill posterior hard palate / pterygoid plates
│ └── Exposes pterygopalatine canal → pterygopalatine fossa inferiorly
│
├── STEP 4: Tumor access / hemostasis
│
└── STEP 5: Closure
└── Primary re-suturing of palatal flap
Limitation: Very restricted access, primarily inferior corridor only; combined with other approaches for larger lesions.
APPROACH 5: MIDFACIAL DEGLOVING APPROACH
(Cummings 7th Ed; Stell and Maran's)
Indications:
- Extensive lesions of nasal cavity, PPF, and maxillary sinus bilaterally
- JNA (Radkowski Grade IIA–IIB)
- Inverted papilloma with PPF extension
Key advantage: Excellent bilateral access with NO external scar.
MIDFACIAL DEGLOVING – STEPS
│
├── STEP 1: Combined intranasal and sublabial incision
│ └── Bilateral intercartilaginous (between upper and lower lateral
│ cartilages) + transfixion incisions combined with
│ bilateral sublabial (Caldwell-Luc level) incisions
│
├── STEP 2: Degloving of midfacial soft tissues
│ └── Entire midfacial skin elevated off bony framework
│ → Exposes bilateral maxillary sinuses, nasal cavity,
│ pterygoid plates bilaterally
│
├── STEP 3: Posterior antrostomy bilaterally
│ └── Access both PPF regions
│
├── STEP 4: Tumor removal
│
└── STEP 5: Closure
└── Replace degloved soft tissue; suture incisions
APPROACH 6: LATERAL RHINOTOMY + MEDIAL MAXILLECTOMY
(Stell and Maran's 5th Ed; Scott-Brown 8th Ed)
Indications:
- Malignant tumors of nasal cavity with PPF involvement
- Inverted papilloma with extensive PPF involvement
- Sinonasal undifferentiated carcinoma
Incision: Weber-Ferguson incision (lateral rhinotomy + sublabial extension ± upper lip split ± subciliary extension for orbital involvement).
APPROACH 7: TOTAL MAXILLECTOMY
(Stell and Maran's; Scott-Brown)
- Infrastructure maxillectomy: Removes hard palate + lower maxilla (below infraorbital nerve). Limited PPF access.
- Total maxillectomy: Removes entire maxilla including orbital floor — excellent PPF exposure. Orbital content may be preserved or removed depending on tumor extent.
- Extended total maxillectomy: Includes pterygoid plates, orbital exenteration for maximum access.
APPROACH 8: INFRATEMPORAL FOSSA APPROACHES (FISCH CLASSIFICATION)
(Cummings 7th Ed; Scott-Brown 8th Ed)
Professor Ugo Fisch described a systematic classification of infratemporal fossa approaches that provide access to the PPF laterally. These are particularly relevant for large JNA, paragangliomas, and skull base tumors extending from PPF into middle cranial fossa.
Fisch ITF Approach Classification:
| Type | Corridor | Main Indication | Key Steps |
|---|---|---|---|
| Type A | Infratemporal + jugular foramen | Glomus jugulare, cholesteatoma | Transmastoid + neck dissection, remove tympanic bone |
| Type B | Infratemporal + clivus | Petroclival meningioma, clival chordoma | Preauricular + zygomatic arch osteotomy, temporalis muscle reflection |
| Type C | Infratemporal + PPF + sphenoid sinus | JNA Grade III–IV, PPF tumors | As Type B + pterygoid plate removal, enters PPF laterally via pterygomaxillary fissure |
| Type D | Infratemporal (middle cranial fossa) | Acoustic neuromas | Extradural middle fossa floor removal |
Fisch Type C – Most Relevant for PPF:
FISCH TYPE C APPROACH – OPERATIVE STEPS
│
├── STEP 1: Preauricular (hemicoronal) incision
│ └── Extended into neck for ICA control if needed
│
├── STEP 2: Zygomatic arch osteotomy
│ └── Detach at root + anteriorly; reflect inferiorly
│ with temporalis muscle (improves exposure)
│
├── STEP 3: Mandibular condyle anterolateral displacement
│ └── OR coronoidectomy to improve access
│
├── STEP 4: Remove lateral pterygoid plate
│ └── Exposes ITF + lateral wall of PPF
│
├── STEP 5: Ligate / embolize maxillary artery
│ └── Proximal control then distal dissection
│
├── STEP 6: Access PPF contents
│ └── V2, maxillary artery branches, PPF tumor
│
├── STEP 7: If ICA involvement
│ └── Dissect petrous ICA with vascular control
│
└── STEP 8: Reconstruction
└── Temporalis muscle flap; titanium plate for zygomatic arch;
fat obliteration of dead space
APPROACH 9: COMBINED ENDOSCOPIC-ASSISTED APPROACHES (RECENT ADVANCES)
(Kassam et al., 2011; Gardner et al., 2014; Snyderman et al., 2015)
Modern skull base surgery increasingly uses combined/hybrid approaches:
- Endoscopic endonasal + Fisch C: Endoscope provides medial visualization while open approach provides lateral control — "two-corridor" concept
- Endoscopic transmaxillary-pterygoid approach: Single corridor accessing PPF and ITF; allows Vidian canal drilling, pterygoid plate removal, and access to foramen rotundum — all endoscopically
6. SPECIFIC INDICATIONS AND APPROACH SELECTION
6.1 Juvenile Nasopharyngeal Angiofibroma (JNA) — Most Common PPF Tumor
(Cummings 7th Ed; Hazarika; Zakir Hussain)
Andrew's Classification / Radkowski Classification guides approach selection:
| Stage | Description | Preferred Approach |
|---|---|---|
| I | Nasopharynx ± choanae | Endoscopic Endonasal |
| IIA | Minimal PPF extension | Endoscopic Endonasal / Caldwell-Luc |
| IIB | Full PPF occupation | Endoscopic Transmaxillary / Midfacial Degloving |
| IIC | Cheek / pterygopalatine / ITF | Fisch Type C / Endoscopic + open |
| III | Intracranial (extradural) | Fisch C + craniotomy |
| IV | Intracranial (intradural) | Cranio-facial + endoscopic |
Pre-operative embolization (24–48 hours before surgery) is mandatory for JNA to reduce intraoperative blood loss (Dhingra; Hazarika).
6.2 Maxillary Artery Ligation for Epistaxis
(Bailey & Love 28th Ed, p.788; Dhingra)
ALGORITHM: SURGICAL MANAGEMENT OF REFRACTORY EPISTAXIS
│
├── Failed conservative measures
│ └── Anterior + posterior nasal packing × 48–72 hrs
│
├── Endoscopic sphenopalatine artery ligation (ESAL)
│ └── First-line surgical option
│ Approach: Endoscopic endonasal via sphenopalatine foramen
│ Clip/cauterize SPA and its branches
│
├── If ESAL fails → Maxillary artery ligation in PPF
│ └── Endoscopic transmaxillary or Caldwell-Luc approach
│
├── Anterior + posterior ethmoidal artery ligation
│ └── Lynch incision (external frontoethmoidectomy)
│ OR transorbital endoscopic approach
│
└── External carotid artery ligation (rare, last resort)
OR Interventional radiology embolization
6.3 Vidian Neurectomy
(Scott-Brown 8th Ed; Stell and Maran's)
Indication: Intractable vasomotor/allergic rhinitis not responding to medical therapy.
Approaches:
- Transantral (Caldwell-Luc): Classic approach — enter PPF via posterior antral wall, identify Vidian canal at base of pterygoid process, divide Vidian nerve
- Transnasal (Chandra's approach): Transseptal
- Endoscopic endonasal: Most widely used currently — drill sphenoid floor to expose Vidian canal; coagulate/divide Vidian nerve at ganglion
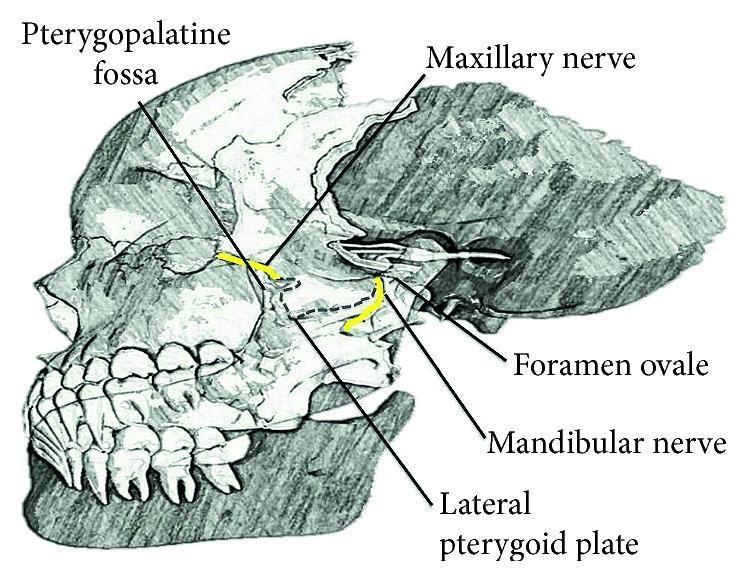
7. SURGICAL ANATOMY DIAGRAM — NEURAL AND VASCULAR PLANES
Lateral skull anatomy showing pterygopalatine fossa, foramen rotundum, V2, and V3:
8. COMPLICATIONS OF PPF SURGERY
(Cummings 7th Ed; Stell and Maran's; Scott-Brown 8th Ed)
| Complication | Cause | Prevention |
|---|---|---|
| Massive hemorrhage | Maxillary artery / pterygoid venous plexus injury | Pre-op embolization, proximal vascular control |
| V2 hypesthesia / anesthesia | Injury to maxillary nerve | Identify nerve early; medial to artery |
| Dry eye | Injury to lacrimal nerve branch or Vidian nerve | Careful nerve preservation |
| Palate / dental numbness | Greater palatine nerve injury | — |
| Orbital injury | Inferior orbital fissure entry | Stay medial/inferior during drilling |
| ICA injury | During lateral skull base approaches | Pre-op planning, intraoperative neuronavigation |
| Meningitis / CSF leak | Skull base breach | Tight dural closure, fat graft |
| Trismus | Temporalis muscle fibrosis (Fisch C) | Early physiotherapy |
| Recurrence (JNA) | Incomplete removal | Neuronavigation, staged embolization |
9. RECENT ADVANCES
(Literature 2015–2024)
9.1 Fully Endoscopic Skull Base Surgery
- Expanded Endoscopic Endonasal Approaches (EEEA) now allow access to the entire PPF and beyond, including the cavernous sinus and Meckel's cave, without any external incision (Kassam, Gardner, Snyderman — Pittsburgh group)
- Binostril four-hand technique: Allows bimanual dissection, hemostasis, and tumor removal simultaneously
- The transmaxillary-pterygoid corridor is now the standard for PPF endoscopic access in most tertiary centers
9.2 Neuronavigation and Image Guidance
- Intraoperative CT/MRI navigation is now standard for PPF surgery, especially with tumors distorting normal anatomy
- Real-time navigation reduces vascular and neural injury rates
- Intraoperative fluorescence angiography (ICG-based) for vascular mapping of maxillary artery branches
9.3 Pre-operative Embolization
- DynaCT angiography allows superselective embolization of feeding vessels (internal maxillary artery branches) for JNA with >90% devascularization
- Embolization 24–48 hours pre-operatively significantly reduces blood loss and conversion rates
9.4 Robotic Surgery
- Transoral robotic surgery (TORS) extended to nasopharyngeal and PPF lesions — limited reports but promising for inferior PPF access
- Da Vinci system studies (2018–2022) showed feasibility for selected benign PPF tumors
9.5 Augmented Reality and 3D Planning
- 3D CT-printed models of PPF allow preoperative surgical simulation
- Augmented reality overlays during surgery improve identification of Vidian canal, foramen rotundum, and maxillary artery
9.6 Proton Beam Radiotherapy as Adjunct
- For residual/recurrent intracranial JNA or malignant PPF tumors — proton beam therapy allows focal high-dose radiation with minimal normal tissue damage
9.7 Endoscopic PPF Approach for Trigeminal Neuralgia
- Endoscopic pterygopalatine ganglion block and neurolysis under direct visualization
- Evolving as alternative to percutaneous approaches, especially when CT-guided access is technically difficult
10. SUMMARY FLOWCHART — APPROACH SELECTION
PPF PATHOLOGY IDENTIFIED
│
├─── BENIGN, SMALL (confined to PPF medially)
│ └──► ENDOSCOPIC ENDONASAL APPROACH (EEA)
│
├─── BENIGN, MODERATE (PPF + posterior maxillary sinus)
│ └──► ENDOSCOPIC TRANSMAXILLARY or CALDWELL-LUC
│
├─── VASCULAR TUMOR (JNA) — Grade IIA/IIB
│ └──► Pre-op embolization → Endoscopic / Midfacial Degloving
│
├─── VASCULAR TUMOR (JNA) — Grade IIC/III
│ └──► Pre-op embolization → Fisch Type C (± endoscopic assist)
│
├─── MALIGNANT, NO SKULL BASE
│ └──► Total Maxillectomy ± Orbital Exenteration (Weber-Ferguson)
│
├─── MALIGNANT, SKULL BASE INVOLVEMENT
│ └──► Combined cranio-facial + endoscopic (multidisciplinary)
│
└─── INTRADURAL EXTENSION
└──► Craniotomy + Endoscopic combined approach
(Neurosurgery + ENT joint)
11. COMPARISON TABLE: OPEN vs. ENDOSCOPIC APPROACHES
| Parameter | Caldwell-Luc (Open Transantral) | Endoscopic Endonasal/Transmaxillary | Fisch Type C |
|---|---|---|---|
| External scar | Yes (sublabial) | None | Yes (preauricular) |
| Access extent | Anterior PPF | Medial + posterior PPF | Lateral PPF + ITF |
| Optics | Naked eye | 0°, 30°, 45° endoscope | Naked eye + loupes |
| Bleeding control | Limited | Excellent (direct visualization) | Excellent |
| Nerve injury risk | Infraorbital N. | V2 if careless | Facial nerve (VII) |
| Hospital stay | 3–5 days | 1–2 days | 5–7 days |
| Best for | Simple PPF lesions, epistaxis | Most PPF pathology currently | Large JNA/ITF tumors |
| Learning curve | Low | Moderate–High | High |
12. KEY POINTS FOR EXAMINATION (50-Mark Recap)
- PPF is a pyramidal space with 6 walls, 5 foramina/communications — knowledge of all is essential
- Contents: Maxillary artery (3rd part) + V2 + pterygopalatine ganglion + Vidian nerve
- Endoscopic approaches have largely replaced open approaches for benign disease
- Fisch Type C remains gold standard for large tumors with ITF/skull base extension
- JNA is the prototype tumor requiring PPF access — stage-based approach selection
- Sphenopalatine artery ligation via endoscopic endonasal approach is first-line surgical treatment for refractory epistaxis
- Vidian neurectomy via endoscopic route is performed for vasomotor rhinitis (now rarely done)
- Neuronavigation is standard of care in modern PPF surgery
- Pre-operative embolization is mandatory for vascular tumors (JNA)
- Complications — most serious are maxillary artery hemorrhage and V2 injury
REFERENCES
| Source | Relevant Content |
|---|---|
| Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, 8th Ed | PPF anatomy, Fisch approaches, JNA staging, Vidian neurectomy |
| Cummings Otolaryngology – Head and Neck Surgery, 7th Ed | Endoscopic skull base surgery, EEA, transmaxillary approach, ITF approaches |
| Stell and Maran's Head and Neck Surgery, 5th Ed | Open approaches, maxillectomy, lateral rhinotomy |
| Zakir Hussain – Textbook of ENT & Head and Neck Surgery | JNA, Caldwell-Luc, PPF anatomy (Indian perspective) |
| Dhingra – Diseases of Ear, Nose and Throat, 7th Ed | Caldwell-Luc, JNA, epistaxis management, infraorbital nerve anatomy |
| Hazarika – Textbook of ENT and Head Neck Surgery | JNA, PPF approaches, embolization |
| Bailey and Love's Short Practice of Surgery, 28th Ed, p.788 | Maxillary artery ligation in PPF for epistaxis |
| Kassam et al., Neurosurgery 2011 | Expanded endoscopic endonasal approaches to PPF and skull base |
| Gardner et al., J Neurosurg 2014 | Transmaxillary-pterygoid endoscopic corridor |
| Snyderman et al., Laryngoscope 2015 | Four-hand binostril technique for PPF tumors |
| Fisch U, Mattox D – Microsurgery of the Skull Base | Classic ITF classification Types A–D |
Clinical Pearl: The key to safe PPF surgery is the recognition of the two planes within the fossa — the superficial arterial plane (maxillary artery coursing anteriorly) and the deeper neural plane (V2 and pterygopalatine ganglion). Always identify the artery first, then work deeper to the nerve. This principle applies across all approaches, whether open or endoscopic.
This is a shared conversation. Sign in to Orris to start your own chat.