Etiopathogenesis
Asking for Preferences
Etiopathogenesis ,diagnosis and management of hiv
Reading File
Finding Sources
Finding Sources
Searching PubMed
"HIV" AND "antiretroviral therapy" AND "guidelines"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive, well-illustrated answer. Here is the full response:
HIV - Etiopathogenesis, Diagnosis, and Management
1. ETIOLOGY
The Virus
HIV (Human Immunodeficiency Virus) belongs to the family Retroviridae, genus Lentivirus. It is a single-stranded, enveloped RNA virus with a genome size of ~9.75 kb. Two species exist:
- HIV-1 - responsible for the global pandemic; further divided into groups M (major, >90% of cases), O (outlying), N (new), and P.
- HIV-2 - less virulent; prevalent mainly in West Africa; naturally resistant to NNRTIs and enfuvirtide.
Among HIV-1 Group M subtypes, Clade C accounts for ~47% of global infections (predominant in India and South Africa), Clade B ~12% (Americas, Europe, Australia), and Clade E predominates in Southeast Asia. - Sherris & Ryan's Medical Microbiology
Structure
The HIV virion has two key surface glycoproteins critical to infection:
- gp120 - binds CD4 receptor on host cells
- gp41 - mediates membrane fusion after coreceptor binding
Transmission Routes
- Sexual contact (anal > vaginal > oral) - most common globally
- Parenteral - sharing needles/syringes, blood transfusions, needle-stick injuries
- Vertical (mother-to-child) - transplacental, intrapartum, breastfeeding. Maternal viral load is a major determinant of perinatal transmission (Lancet 2025 systematic review, PMID 40652949).
2. PATHOGENESIS
Step-by-Step Life Cycle
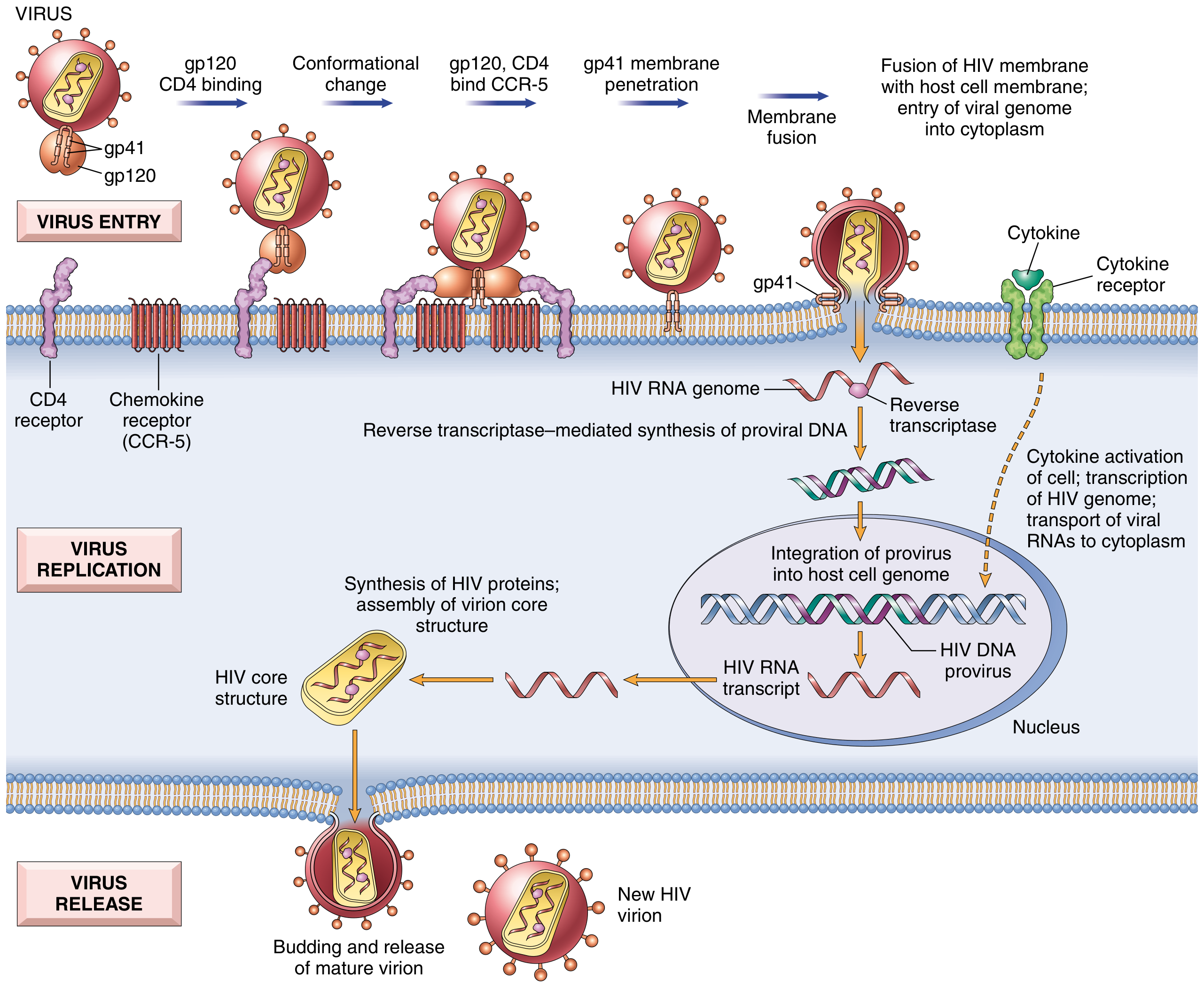
Life cycle of HIV (from Robbins, Cotran & Kumar Pathologic Basis of Disease)
Entry:
- HIV gp120 binds to CD4 receptor on T-helper cells, macrophages, and dendritic cells.
- A conformational change exposes the coreceptor binding site.
- gp120 then binds the CCR5 coreceptor (M-tropic strains, important in early infection) or CXCR4 (T-tropic strains, later disease).
- gp41 mediates membrane fusion, releasing the viral core into the cytoplasm.
Replication:
5. Viral RNA is reverse-transcribed into double-stranded DNA by reverse transcriptase (error-prone, driving antigenic variation).
6. Viral DNA (provirus) is integrated into the host genome via integrase.
7. The provirus may remain latent until host T-cell activation.
8. On T-cell activation, NF-kB (stimulated by antigens, cytokines like TNF) drives transcription of both host immune genes and HIV long-terminal-repeat sequences simultaneously - described as "subversion from within." - Robbins, Cotran & Kumar
9. Viral RNA is translated, polyproteins are cleaved by protease, and new virions bud from the cell surface.
Key Defense Evasion:
- The viral protein Vif binds and degrades host APOBEC3G (a cytidine deaminase that would otherwise introduce lethal mutations into viral DNA).
Natural History and Stages
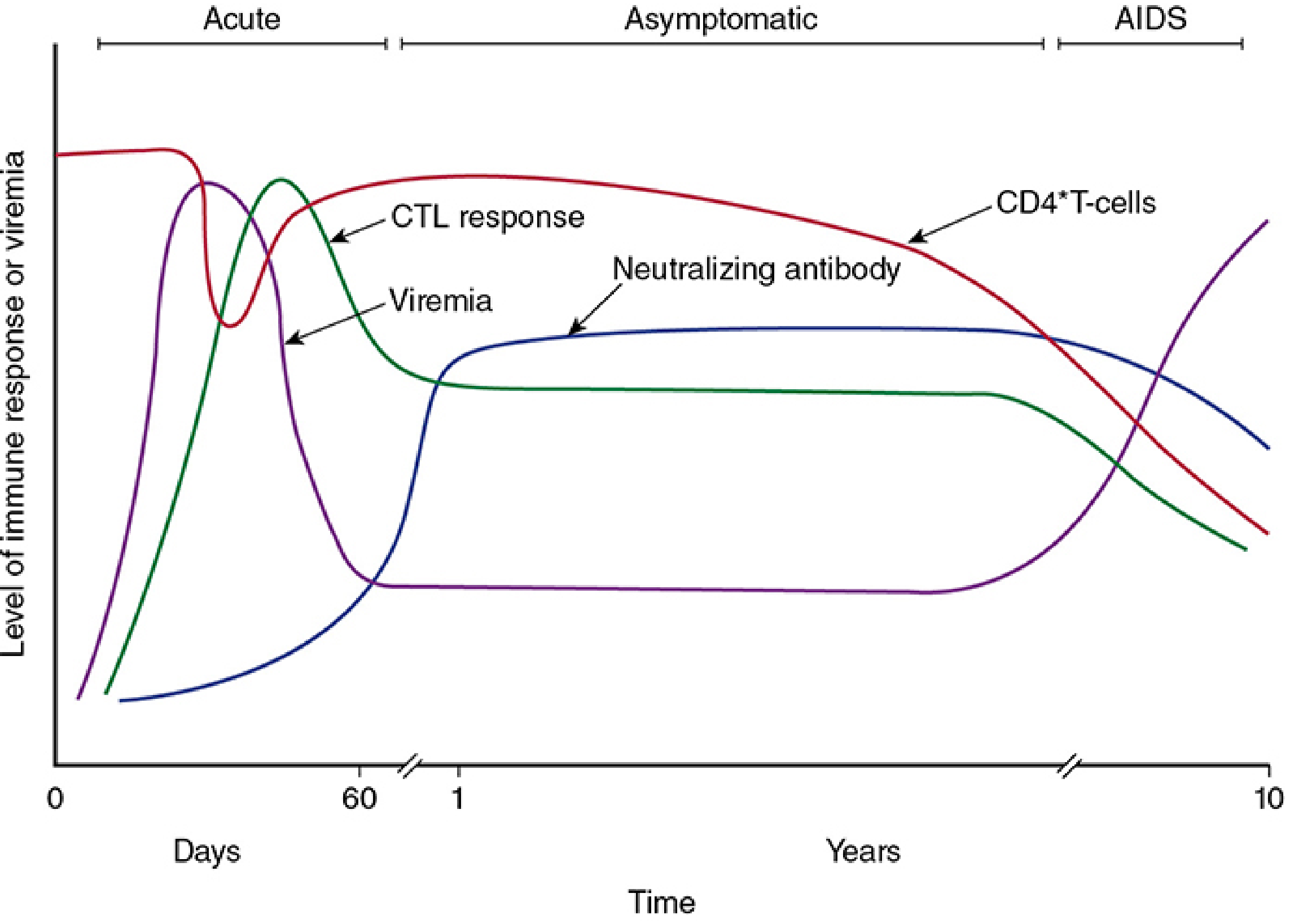
Temporal changes in viremia, CD4 T-cells, CTL response, and neutralizing antibody during HIV-1 infection (Sherris & Ryan's Medical Microbiology)
HIV infection follows five characteristic phases:
| Phase | Timing | Features |
|---|---|---|
| Acute retroviral syndrome | 2-6 weeks post-exposure | Flu/mononucleosis-like: fever, rash, lymphadenopathy, pharyngitis, malaise. Neurologic symptoms (meningitis, encephalitis) in |
| Seroconversion / immune response | ~60 days | CTL response peaks, then neutralizing antibodies develop; viremia drops to a "set point" |
| Clinical latency (chronic phase) | Years (~10 years untreated) | Asymptomatic or persistent generalized lymphadenopathy; continued low-level viral replication; CD4 slowly declines (~50-100 cells/µL per year) |
| Symptomatic HIV | CD4 200-500 | Constitutional symptoms, opportunistic infections (TB, fungal pneumonia) begin |
| AIDS | CD4 <200/µL or AIDS-defining illness | Severe opportunistic infections (CMV, MAC, PCP), HIV encephalopathy, AIDS-defining malignancies (Kaposi's sarcoma, NHL, invasive cervical cancer) |
Mechanisms of CD4+ T-Cell Depletion
Approximately 100 billion new viral particles are produced every day, and 1-2 billion CD4+ T cells die daily in untreated infection. - Robbins, Cotran & Kumar
Mechanisms of T-cell loss include:
- Direct cytopathic effect - viral replication leads to cell lysis (primary mechanism in circulating T cells)
- Syncytium formation - gp120 on infected cells binds CD4 on neighboring uninfected cells, forming giant multinucleated cells
- Apoptosis - both infected and uninfected bystander T cells undergo programmed death
- ADCC (Antibody-dependent cell cytotoxicity) - anti-gp120 antibodies on infected CD4+ cell surfaces trigger NK cell-mediated killing
- Interference with T-cell maturation in the thymus
- CTL killing of infected cells
Infection of Non-T Cells
- Macrophages - express CCR5 and low-level CD4; >90% of acute infections are by M-tropic (CCR5-using) strains. Macrophages are resistant to HIV cytopathic effects and act as a long-term viral reservoir, especially in the lungs and brain. Infected monocytes carry HIV to the CNS (explaining HIV encephalopathy).
- Dendritic cells - mucosal DCs capture virus and transport it to lymph nodes, facilitating T-cell infection. DC-SIGN (a lectin receptor) binds HIV and presents it to T cells in intact, infectious form.
- Follicular dendritic cells (FDCs) - trap antibody-coated virions on their surface; these retain infectivity for CD4+ follicular helper T cells.
B-Cell Dysfunction
Although HIV does not infect B cells directly, paradoxical polyclonal B-cell activation occurs early (due to EBV reactivation, viral gp41, IL-6 from infected macrophages), leading to:
- Hypergammaglobulinemia
- Germinal center hyperplasia
- Autoimmune phenomena (e.g., immune thrombocytopenia)
- Impaired specific antibody responses to new antigens (due to overwhelmed B-cell capacity)
Why HIV Persists Despite Immune Response
The immune system cannot eliminate HIV because of:
- High mutation rate - generates CTL and antibody escape variants
- Latent proviral reservoir - integrated DNA in resting CD4+ memory T cells is invisible to immune surveillance
- Cell-to-cell spread - bypasses neutralizing antibodies
- MHC I and II suppression - impairs antigen presentation
- Antigenic variation - especially in the envelope gene (20-30% inter-clade variation)
3. DIAGNOSIS
HIV Testing Algorithm (2014 CDC Recommended)
Step 1 - 4th Generation Ag/Ab Combination Immunoassay (screening)
- Detects both p24 antigen AND HIV-1/HIV-2 antibodies simultaneously
- HIV can be detected as early as 18 days post-infection
- Sensitivity: 99-100% | Specificity: 98-100%
- Positive result → proceed to Step 2
Step 2 - HIV-1/HIV-2 Antibody Differentiation Assay (confirmatory)
- Distinguishes HIV-1 from HIV-2 antibodies
- Replaces the old Western blot as the confirmatory test
Step 3 - HIV-1 RNA NAT (Nucleic Acid Test / Viral Load)
- If Step 1 reactive but Step 2 negative/indeterminate
- HIV RNA detectable from ~11 days post-infection (earliest detection)
- In acute retroviral syndrome: viral load typically >100,000 copies/mL
- A viral load <10,000 copies/mL on an initial test should raise suspicion for a false positive
Key point: Because the 4th-generation Ag/Ab assay may be negative at the time of acute seroconversion, an HIV viral load assay should always be sent when acute HIV is being considered. - Symptom to Diagnosis, 4th Ed.
Additional Baseline Testing After HIV Diagnosis
| Test | Purpose |
|---|---|
| CD4+ T-cell count | Stage disease; guide OI prophylaxis |
| HIV RNA viral load | Baseline; monitor ART response |
| Genotype resistance testing | Recommended in ALL newly diagnosed patients (transmission of drug-resistant strains is documented) |
| HLA-B*5701 testing | Before abacavir use (hypersensitivity) |
| Hepatitis B/C serology | Coinfection screening; affects ART choice |
| TB screening | TB/HIV coinfection common |
| CMV, Toxoplasma serology | Baseline for OI risk stratification |
CDC Staging (2014 revised)
| Stage | CD4 count (adults ≥6 years) |
|---|---|
| Stage 0 | HIV+ but test negative within prior 6 months (early/acute infection) |
| Stage 1 | ≥500 cells/µL |
| Stage 2 | 200-499 cells/µL |
| Stage 3 (AIDS) | <200 cells/µL OR AIDS-defining illness |
4. MANAGEMENT
Principle: Treat Everyone
Combination antiretroviral therapy (ART) - also called HAART - is indicated for all HIV-positive individuals regardless of CD4 count, initiated as soon as possible after diagnosis (same-day or "rapid start" initiation is now preferred). - Harrison's Principles of Internal Medicine 22e (2025); EACS Guidelines 2025, PMID 41088922
The goal of ART is: viral load suppressed to <50 copies/mL within 6 months.
Drug Classes
| Class | Mechanism | Examples |
|---|---|---|
| NRTIs (Nucleoside/Nucleotide Reverse Transcriptase Inhibitors) | Block HIV RNA→DNA reverse transcription (chain termination) | Tenofovir (TDF/TAF), Emtricitabine (FTC), Lamivudine (3TC), Abacavir (ABC), Zidovudine (AZT) |
| NNRTIs (Non-Nucleoside RTIs) | Non-competitive RT inhibitors; HIV-1 specific | Efavirenz, Rilpivirine, Doravirine, Etravirine |
| PIs (Protease Inhibitors) | Block viral polyprotein cleavage | Darunavir, Atazanavir (boosted with ritonavir or cobicistat) |
| INSTIs (Integrase Strand Transfer Inhibitors) | Block integration of proviral DNA | Dolutegravir (DTG), Bictegravir (BIC), Raltegravir, Cabotegravir |
| CCR5 Antagonists | Block viral entry via CCR5 | Maraviroc |
| Fusion Inhibitors | Block gp41-mediated membrane fusion | Enfuvirtide (T-20) |
| CD4 Attachment Inhibitors | Block gp120 binding to CD4 | Fostemsavir |
| Capsid Inhibitors | Disrupt viral capsid assembly/uncoating | Lenacapavir |
Note: NNRTIs, enfuvirtide, and fostemsavir are NOT active against HIV-2 and should not be used in HIV-2-infected patients. - Harrison's 22e
Preferred First-Line Regimens (Treatment-Naive Adults)
Standard preferred regimens use 2 NRTIs + 1 INSTI:
- Bictegravir/Tenofovir AF/Emtricitabine (Biktarvy) - single-pill, once daily ✓
- Dolutegravir + Tenofovir/Emtricitabine - highly effective, high barrier to resistance ✓
- Dolutegravir + Lamivudine (2-drug regimen) - for HBV-negative patients with baseline HIV RNA <500,000 copies/mL ✓
A typical regimen includes a pharmacokinetic enhancer (ritonavir or cobicistat) when PI-based regimens are used.
Long-acting injectables (Cabotegravir + Rilpivirine IM monthly or every 2 months) are now available for patients who prefer avoiding daily oral therapy.
Monitoring on ART
| Parameter | Frequency |
|---|---|
| HIV RNA (viral load) | At 4-8 weeks after ART start, then every 3-6 months until suppressed, then every 6-12 months |
| CD4 count | Every 3-6 months initially; annually once stable |
| Drug resistance testing | Before starting ART; if virologic failure |
| Adherence assessment | Every visit |
Opportunistic Infection (OI) Prophylaxis
| CD4 count | OI risk | Prophylaxis |
|---|---|---|
| <200/µL | Pneumocystis jirovecii pneumonia (PCP) | Trimethoprim-sulfamethoxazole (TMP-SMX) |
| <100/µL | Toxoplasma encephalitis | TMP-SMX (same drug covers both) |
| <50/µL | Mycobacterium avium complex (MAC) | Azithromycin weekly |
| All stages | TB (if LTBI+) | Isoniazid preventive therapy |
Post-Exposure Prophylaxis (PEP)
- Indicated within 72 hours of exposure to HIV-infected blood or body fluids (sexual, needlestick, or non-occupational).
- Regimen: Tenofovir-Emtricitabine 300/200 mg once daily + Dolutegravir 50 mg once daily for 28 days.
- Follow-up HIV testing at 6 weeks. - Washington Manual of Medical Therapeutics
Pre-Exposure Prophylaxis (PrEP)
- Oral PrEP: Tenofovir AF/Emtricitabine (Descovy) or Tenofovir DF/Emtricitabine (Truvada)
- Injectable PrEP: Cabotegravir IM every 2 months (highly effective, superior to oral in some trials)
- Indicated for HIV-negative individuals at substantial risk.
Special Populations
- Pregnancy: Continue ART throughout. Prefer dolutegravir-based regimens. Viral load suppression reduces MTCT to <1%. IV Zidovudine during labor if viral load >1000 copies/mL. - Lancet 2025 meta-analysis PMID 40652949
- TB coinfection: Start TB treatment first; introduce ART within 2-8 weeks (within 2 weeks if CD4 <50).
- HIV-2: Avoid NNRTIs, enfuvirtide, fostemsavir; use INSTI-based regimens.
Targets: UNAIDS 95-95-95
The global target is that by 2025: 95% of HIV-positive people know their status → 95% of diagnosed are on ART → 95% of those on ART are virally suppressed.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Sherris & Ryan's Medical Microbiology 8e; Harrison's Principles of Internal Medicine 22e (2025); Symptom to Diagnosis 4e; Park's Textbook of Preventive and Social Medicine; Washington Manual of Medical Therapeutics. Recent guideline: EACS Guidelines v13.0 (2026), PMID 41088922.
In short
HIV - Quick Summary
Etiopathogenesis
The Virus: HIV (Retroviridae, Lentivirus) - single-stranded RNA virus. Two types: HIV-1 (global) and HIV-2 (West Africa, milder).
Transmission: Sexual contact > parenteral (needles, blood) > vertical (mother to child)
How it causes disease:
- gp120 binds CD4 receptor → then binds coreceptor (CCR5 or CXCR4) → gp41 mediates membrane fusion → viral RNA enters cell
- Reverse transcriptase converts RNA → DNA → integrates into host genome (provirus)
- Slowly destroys CD4+ T cells (~100 billion virions/day; 1-2 billion CD4 cells die daily)
- When CD4 <200/µL → AIDS → opportunistic infections
Three clinical stages:
- Acute (weeks 2-6): fever, rash, lymphadenopathy, high viremia
- Latency (years): asymptomatic, CD4 slowly falls
- AIDS (CD4 <200): OIs, malignancies, death
Diagnosis
| Test | Use |
|---|---|
| 4th Gen Ag/Ab assay | Screening - detects p24 Ag + antibodies; positive from day 18 |
| HIV-1/2 Ab differentiation | Confirms & distinguishes HIV-1 vs HIV-2 |
| HIV RNA (viral load) | Earliest detection (day 11); confirms acute infection |
| CD4 count | Stages disease |
| Genotype resistance test | All newly diagnosed patients |
Acute HIV → always send viral load (Ag/Ab test can still be negative)
Management
Treat everyone - ART started immediately regardless of CD4 count.
Goal: Viral load <50 copies/mL
Drug classes:
| Class | Key Drugs |
|---|---|
| NRTI | Tenofovir, Emtricitabine, Lamivudine |
| NNRTI | Efavirenz, Rilpivirine |
| PI | Darunavir + ritonavir/cobicistat |
| INSTI (preferred) | Dolutegravir, Bictegravir |
| Entry inhibitors | Maraviroc (CCR5), Enfuvirtide |
Preferred 1st-line regimen:
- Bictegravir/TAF/FTC (Biktarvy) - single pill once daily
- Dolutegravir + TDF/FTC - widely used globally
OI Prophylaxis:
- CD4 <200 → TMP-SMX (PCP)
- CD4 <50 → Azithromycin (MAC)
PEP: Tenofovir/FTC + Dolutegravir × 28 days (within 72 hrs of exposure)
PrEP: Tenofovir/FTC daily OR Cabotegravir IM every 2 months (for high-risk HIV-negative individuals)
This is a shared conversation. Sign in to Orris to start your own chat.