Urinary bladder
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of Urinary Bladder Pathology drawn from Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease.
Urinary Bladder: Pathology & Diseases
1. Congenital Anomalies
| Anomaly | Key Features |
|---|---|
| Vesicoureteral reflux | Most common and serious congenital anomaly; predisposes to ascending pyelonephritis and loss of renal function |
| Diverticula | Pouch-like invaginations (congenital or acquired); congenital ones result from focal muscular failure; acquired ones most often follow BPH/outflow obstruction. Rare carcinomas arise within diverticula - typically at higher stage because the muscularis propria layer is thin or absent |
| Exstrophy | Developmental failure of the anterior abdominal/bladder wall; bladder mucosa communicates with the skin surface. Leads to chronic infection, intestinal metaplasia, and markedly increased risk of adenocarcinoma |
| Urachal anomalies | Persistence of the urachal canal creates fistula to umbilicus or urachal cysts. Cysts are prone to neoplastic transformation (mostly adenocarcinoma). Urachal cancers are only 0.1-0.3% of all bladder cancers but constitute 20-40% of bladder adenocarcinomas |
2. Inflammation (Cystitis)
Etiology
- Bacterial cystitis - most common; females more susceptible due to shorter urethra. Organisms: E. coli (most common) > Proteus > Klebsiella > Enterobacter
- Hemorrhagic cystitis - caused by cyclophosphamide or adenovirus/BK virus infection
- Tuberculous cystitis - almost always secondary to renal TB
- Fungal cystitis - Candida albicans or cryptococcal agents; mainly in immunosuppressed patients or those on long-term antibiotics
- Schistosomal cystitis (S. haematobium) - major cause in Africa and Middle East; leads to squamous metaplasia and increased squamous cell carcinoma risk
- Emphysematous cystitis - gas-forming bacteria (e.g., Clostridium perfringens) create gas-filled vesicles in the bladder wall
Clinical triad of cystitis
- Frequency (in acute cases, every 15-20 minutes)
- Lower abdominal/suprapubic pain
- Dysuria
Malakoplakia
A distinctive chronic inflammatory reaction arising in the setting of chronic bacterial infection (mainly E. coli or Proteus). Stems from acquired defects in phagocyte function, so undigested bacterial products accumulate and form Michaelis-Gutmann bodies - laminated mineralized concretions due to calcium salt deposition.
Interstitial Cystitis (Bladder Pain Syndrome)
- Occurs mostly in females; etiology unknown
- Defined by the AUA as "an unpleasant sensation perceived to be related to the urinary bladder, with urinary symptoms >6 weeks duration, in the absence of infection or other identifiable causes"
- Cystoscopy shows: mucosal fissures and punctate hemorrhages (glomerulations)
- Histology: nonspecific; increased mast cells in submucosa; some cases have chronic mucosal Hunner ulcers
- Biopsy's main role is to rule out carcinoma in situ (CIS), which clinically mimics interstitial cystitis
3. Neoplasms
Bladder cancer is the 9th most common cancer worldwide. ~80% of patients are between 50-80 years old. Men are more commonly affected.
Histologic Types (USA)
| Type | Frequency |
|---|---|
| Urothelial (transitional cell) carcinoma | ~90% |
| Squamous cell carcinoma | 2-5% (much higher in schistosomiasis-endemic areas) |
| Adenocarcinoma | Rare |
Risk Factors
- Cigarette smoking (most important environmental factor)
- Occupational carcinogens (aniline dyes, aromatic amines)
- Radiation therapy
- Cyclophosphamide (hemorrhagic cystitis -> carcinoma)
- Schistosomiasis (-> squamous cell carcinoma)
- Family history
Pathogenesis: Two Major Molecular Pathways
| Pathway | Lesion | Mutations | Behavior |
|---|---|---|---|
| Papillary (low-grade) | Superficial papillary tumors | FGFR3 amplification, activating RAS and PI3-kinase mutations | Frequently recur; muscle invasion in only ~20%, usually when TP53 mutation also present |
| CIS pathway (high-grade) | Flat (non-papillary) CIS | p53 and RB disruption, additional epigenetic changes | Progresses to muscle-invasive cancer |
WHO 2022 Classification of Non-Invasive Urothelial Tumors
Flat lesions:
- Urothelial dysplasia
- Urothelial carcinoma in situ (CIS)
Papillary lesions (from lowest to highest grade):
- Urothelial papilloma
- Papillary urothelial neoplasm of low malignant potential (PUNLMP)
- Low-grade papillary urothelial carcinoma
- High-grade papillary urothelial carcinoma
Staging (AJCC 8th Edition / pTNM)
| Stage | Description |
|---|---|
| Ta | Noninvasive papillary carcinoma |
| Tis | Flat CIS |
| T1 | Invades lamina propria |
| T2a | Invades superficial muscularis propria (inner half) |
| T2b | Invades deep muscularis propria (outer half) |
| T3a | Invades perivesical soft tissue microscopically |
| T3b | Invades perivesical soft tissue macroscopically |
| T4a | Invades prostate stroma, seminal vesicles, uterus, or vagina |
| T4b | Invades pelvic or abdominal wall |
Non-muscle-invasive (Ta, Tis, T1) = 70-80% of all urothelial neoplasms
Muscle-invasive (T2+) = 20-30%
Histologic Images
Bladder CIS:
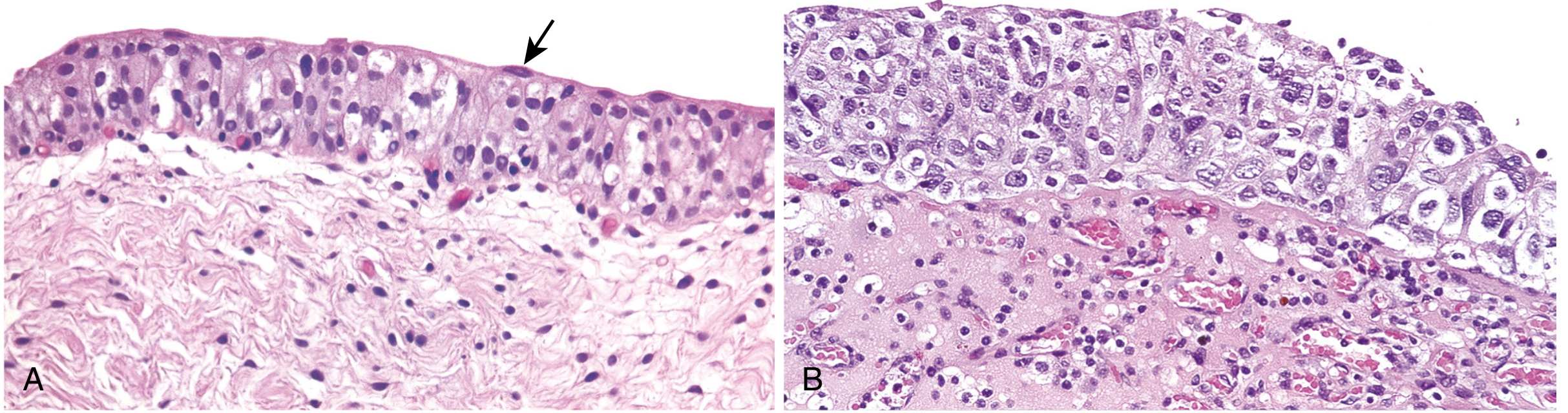
(A) Normal urothelium with uniform nuclei and a well-developed umbrella cell layer (arrow). (B) CIS showing a disorganized urothelium with markedly enlarged and pleomorphic nuclei.
Advanced invasive urothelial carcinoma (gross):
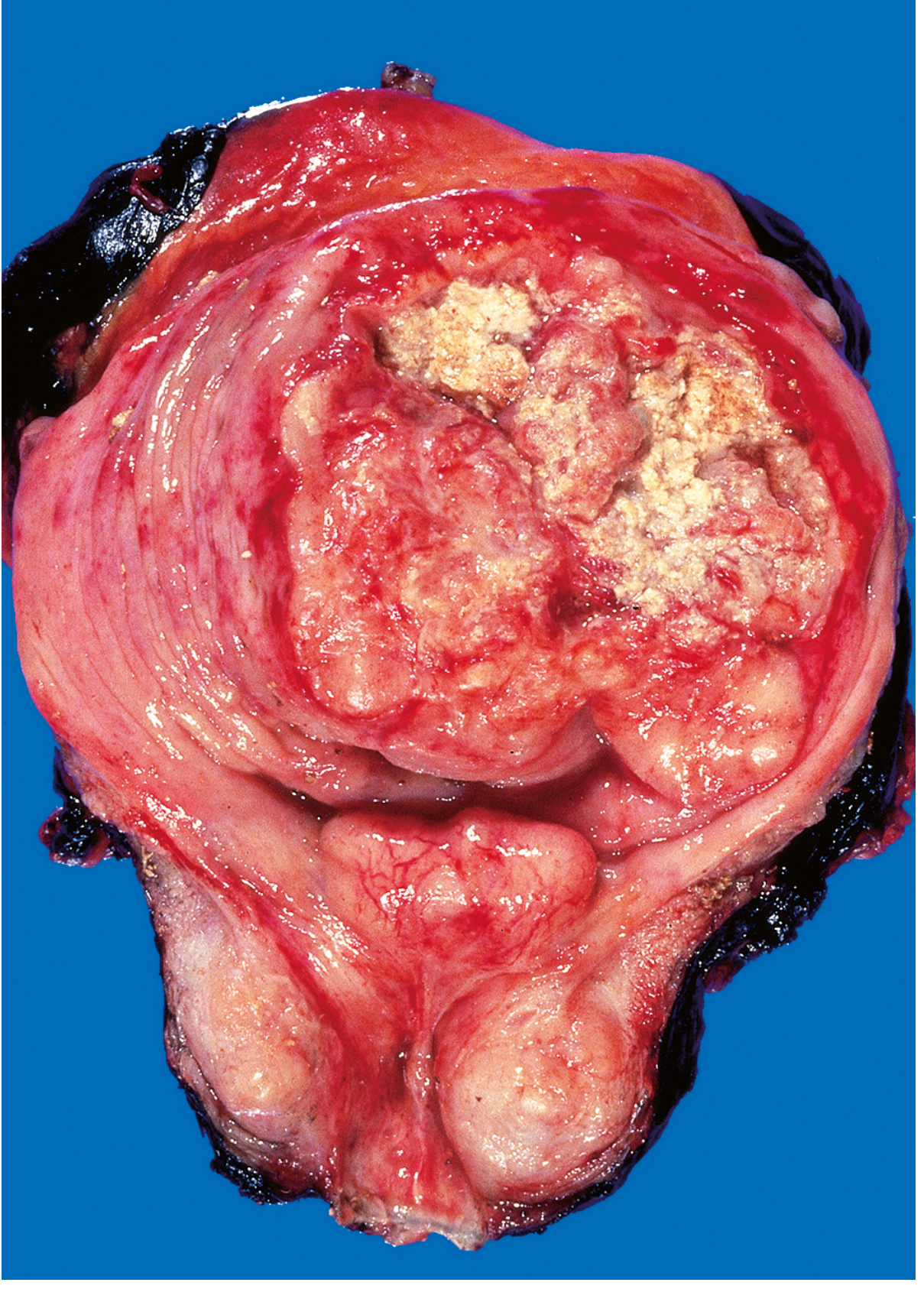
Opened bladder showing a high-grade invasive urothelial carcinoma. The multinodular neoplasm has fungated into the bladder lumen. Yellow areas represent ulceration and necrosis.
Clinical Presentation
- Painless hematuria - most common symptom
- Frequency, urgency, dysuria may accompany hematuria
- Ureteral obstruction can lead to pyelonephritis or hydronephrosis
Treatment Summary
| Disease extent | Treatment |
|---|---|
| Small, localized, low-grade papillary | Transurethral resection (TURBT) alone |
| CIS, high-grade, large, multifocal, or lamina propria invasion | Intravesical BCG (M. bovis attenuated strain) |
| Muscle-invasive (T2+) | Radical cystectomy ± neoadjuvant/adjuvant chemotherapy, or radiation |
| BCG-refractory CIS or high-grade disease | Radical cystectomy |
| Metastatic disease | Chemotherapy (5-year survival ~15%); ~30% respond to immune checkpoint inhibitors; novel antibody-drug conjugates targeting Nectin-4 and FGFR3 |
Prognosis
| Tumor Type | Prognosis |
|---|---|
| Papilloma, PUNLMP, low-grade papillary carcinoma | 98% 10-year survival; <10% progress to higher grade |
| High-grade papillary carcinoma | ~25% invade and cause death |
| CIS alone (no invasive component) | 28% progress to muscle-invasive; 7% die of disease |
| CIS with associated invasive carcinoma | 59% progress to muscle-invasive; 45% die of disease |
Non-muscle-invasive bladder cancers recur in up to 70% of cases. Because of this, lifelong cystoscopic surveillance is mandatory.
Other Epithelial Bladder Tumors
- Squamous cell carcinoma - 3-7% in USA; much more common in schistosomiasis-endemic countries; arises from squamous metaplasia driven by chronic inflammation
- Adenocarcinoma - rare; arises from urachal remnants, intestinal metaplasia in exstrophy, or cystitis glandularis
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (9780443264528); Robbins & Kumar Basic Pathology (9780323790185)
This is a shared conversation. Sign in to Orris to start your own chat.