Tell me about IBD in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"inflammatory bowel disease"[MeSH Terms] AND "therapy"[MeSH Terms]
Reading File
Finding Sources
Searching PubMed
"inflammatory bowel disease" AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive response. Let me compile the full detailed answer.
Inflammatory Bowel Disease (IBD) - A Comprehensive Overview
IBD refers to two chronic idiopathic inflammatory disorders: Ulcerative Colitis (UC) and Crohn Disease (CD). Approximately 10% of IBD cases cannot be cleanly distinguished and are labeled "IBD-undetermined." Both conditions are lifelong, relapsing-remitting illnesses driven by a dysregulated immune response in a genetically predisposed host exposed to environmental triggers.
1. Epidemiology
IBD occurs worldwide, but incidence is highest in North America, the UK, and northern Europe, with rates rising globally.
| Metric | Ulcerative Colitis | Crohn Disease |
|---|---|---|
| Incidence (North America) | ~19/100,000 person-years | ~20/100,000 person-years |
| Prevalence (North America) | ~280/100,000 | ~320/100,000 |
| Peak age of onset | 20-40 (2nd peak >70) | 15-30 (2nd peak in 7th decade) |
| Sex distribution | 1:1 (F:M) | 1.2:1 (F:M) |
Both diseases peak in the second to fourth decade with a smaller second peak in the elderly. IBD is more prevalent in White and Ashkenazi Jewish populations, though the incidence in African Americans is approaching that of Whites. Cigarette smoking paradoxically worsens Crohn disease but has an ameliorating effect on UC. NSAIDs can trigger flares in both. Appendectomy (for inflammatory indications) is protective against UC.
- Goldman-Cecil Medicine, p. 1479-1480
2. Pathobiology
Three major pathways converge to trigger IBD: genetic predisposition, immune dysregulation, and an environmental trigger.
Genetics
- 5-20% of IBD patients have a first-degree relative with IBD; first-degree relatives carry a 10-15x increased risk.
- Identical twin concordance for CD is ~50%; for UC it is somewhat lower.
- Over 200 gene susceptibility loci have been linked to IBD; at least 30 are specific to CD, 20+ to UC.
- NOD2/CARD15 (chromosome 16q12): expressed in Paneth cells, macrophages, and dendritic cells. Senses muramyl dipeptide (a component of gram-positive bacterial cell walls). A mutation in the leucine-rich domain fails to activate NF-kB and is strongly associated with CD.
- ATG16L1 and IRGM genes (involved in autophagy) are linked to CD susceptibility - they impair the cell's ability to process intracellular pathogens.
- IL-23 receptor polymorphisms confer varied risk for both UC and CD.
- HLA-DR class II polymorphisms increase risk for UC.
- ADCY7 missense mutations cause excessive inflammatory responses predisposing to UC.
- IBD is also associated with Turner syndrome, Hermansky-Pudlak syndrome, ankylosing spondylitis, psoriasis, primary sclerosing cholangitis, and multiple sclerosis.
Microbiome and Immune Dysregulation
The gut microbiome plays an important role. Patients with IBD show reduced microbial diversity with decreased Firmicutes (especially Faecalibacterium prausnitzii) and increased Proteobacteria. The intestinal epithelial barrier becomes "leaky," allowing microbial antigens to penetrate, which the innate immune system fails to clear adequately, leading to an overactive adaptive immune response. In CD, the inflammation is predominantly Th1/Th17-driven (IL-12, IL-23, TNF-alpha); in UC, it is more Th2-mediated.
- Goldman-Cecil Medicine, p. 1480
3. Pathology: Key Differences
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Location | Esophagus to anus ("mouth to anus") | Colon only |
| Pattern | Skip lesions (non-contiguous) | Continuous, starts in rectum, extends proximally |
| Depth | Transmural (full wall) | Mucosal/submucosal only |
| Ulceration | Discrete, aphthous → cobblestone | Continuous |
| Granulomas | Noncaseating (in ~15% biopsies; up to 70% surgical specimens) | Absent |
| Fistula | Present (common) | Absent |
| Stricture | Present | Absent (lead pipe colon from fibrosis) |
| Perianal disease | Present (fissures, skin tags) | Absent |
| Pseudopolyps | Less common | Common (from epithelial regeneration) |
| Rectal involvement | 60% | Always (pathognomonic) |
Histopathology - Crohn Disease
- Early: acute inflammatory infiltrate in the lamina propria, cryptitis, crypt abscesses
- Late: crypt architectural distortion, lymphocytic infiltrate with branching/shortening of crypts
- Noncaseating granulomas confirm the diagnosis when present alongside classic features
- Surgical specimens show transmural inflammation and fat creeping (fat wrapping) on the serosal surface
Histopathology - Ulcerative Colitis
-
Early: epithelial necrosis, acute inflammatory infiltrate, cryptitis, crypt abscesses
-
Chronic: predominantly lymphocytic infiltrate, marked crypt architectural distortion
-
Goldman-Cecil Medicine, p. 1421, 1429-1431
4. Clinical Manifestations
Crohn Disease
The terminal ileum is affected in ~70% of patients. Disease distribution:
- Ileal only (ileitis): 30%
- Ileocolonic: 40%
- Colonic only: 25-30%
- Upper GI (gastric, duodenal, jejunal): uncommon
Symptoms: abdominal pain (typically right lower quadrant), diarrhea, hematochezia, fatigue, weight loss, fever (with severe disease). Patients may present with obstructive symptoms from strictures. Perianal disease (fistulas, abscesses, fissures) is highly characteristic.
Ulcerative Colitis
- Proctitis (rectum only): ~40-50%
- Left-sided colitis (distal to splenic flexure): ~30-35%
- Pancolitis (extensive colitis): ~20%
Symptoms: bloody diarrhea with mucus, urgency, tenesmus (rectal pain/cramping), and abdominal pain. Systemic symptoms (fever, tachycardia, weight loss) indicate severe disease.
Acute severe UC (fulfilling Truelove-Witts criteria): ≥6 bloody stools/day + any one of: fever >37.8°C, HR >90 bpm, Hb <10.5 g/dL, ESR >30 mm/hr.
- Goldman-Cecil Medicine, p. 1481-1482
5. Endoscopic Appearances
Crohn Disease - Cobblestoning
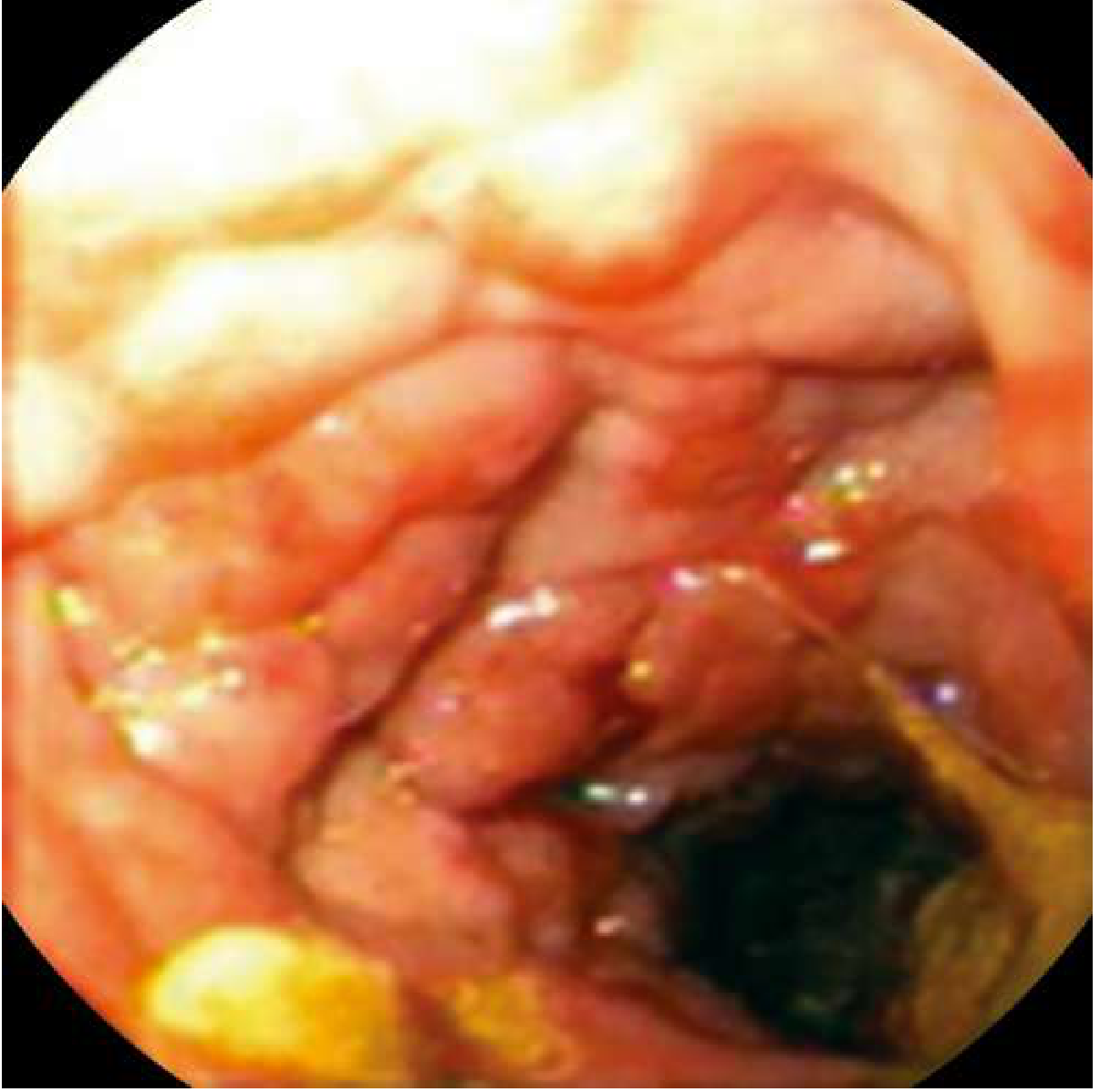
Endoscopic appearance of Crohn disease showing cobblestoning - deep intersecting ulcers with islands of relatively normal mucosa.
- Early: superficial aphthous ulcers
- Progressive: deeper round, linear, or serpiginous ulcers
- Advanced: cobblestone appearance from intersecting longitudinal and transverse ulcers; "skip areas" of normal mucosa between diseased segments
Ulcerative Colitis
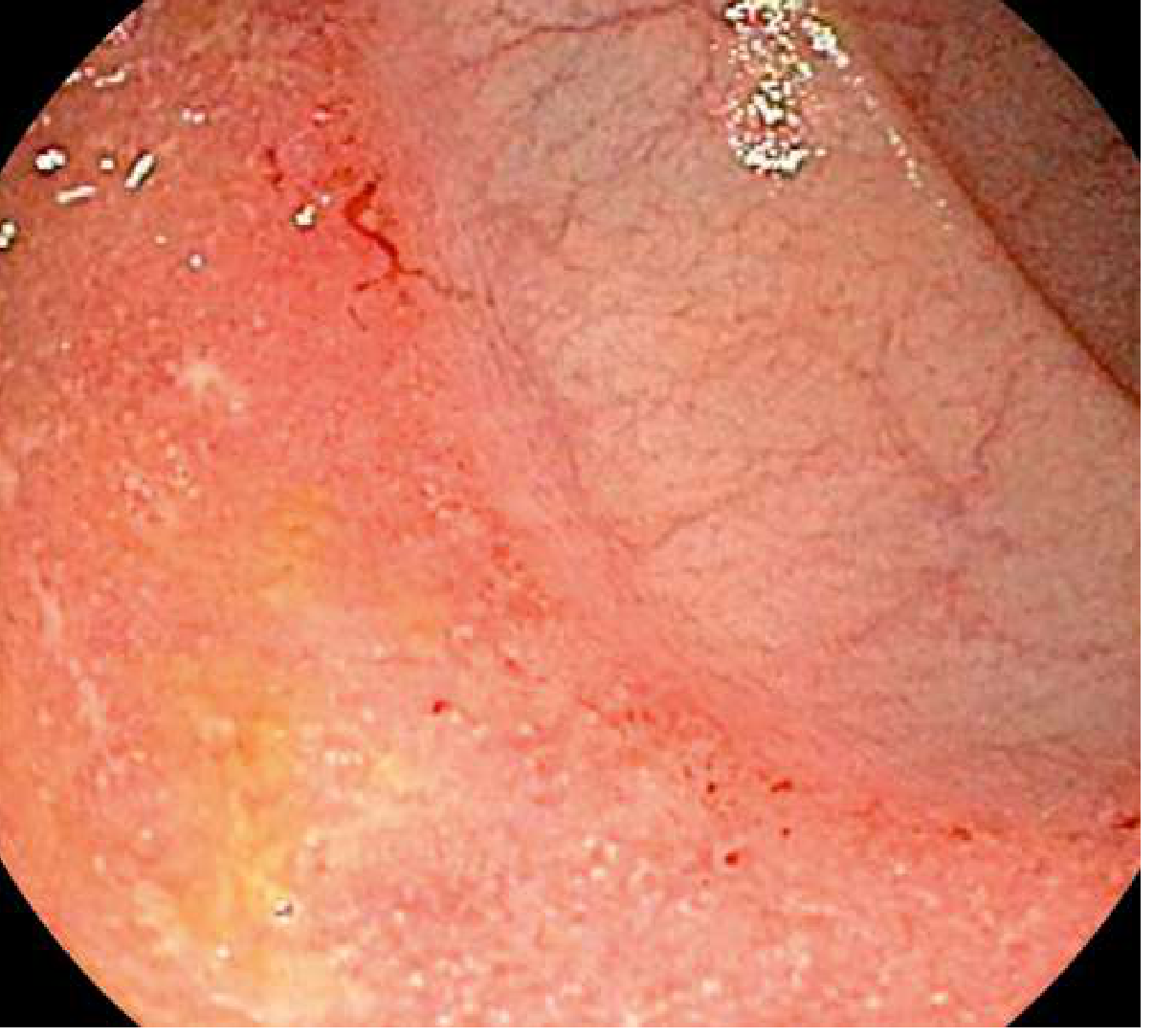
Endoscopic appearance of ulcerative colitis - diffuse mucosal erythema, granularity, and loss of normal vascular pattern starting from the rectum.
-
Mild: granular, edematous, erythematous mucosa with loss of vascular pattern
-
Moderate-severe: friable mucosa, contact bleeding, ulceration
-
Chronic: pseudopolyps, loss of haustral folds, "lead pipe" colon
-
Goldman-Cecil Medicine, p. 1560, 1576-1585
6. Extraintestinal Manifestations (EIMs)
EIMs occur in 25-40% of IBD patients and may involve virtually any organ system:
| System | Manifestation | Correlation with IBD activity |
|---|---|---|
| Musculoskeletal | Peripheral arthritis (large joint > small), ankylosing spondylitis, sacroiliitis | Peripheral correlates; axial is independent |
| Skin | Erythema nodosum, pyoderma gangrenosum | Erythema nodosum correlates with activity |
| Ocular | Episcleritis, uveitis, iritis | Episcleritis correlates with activity |
| Hepatobiliary | Primary sclerosing cholangitis (PSC - more in UC), fatty liver, cholangiocarcinoma | PSC is independent |
| Hematologic | Anemia (iron, B12, folate deficiency), VTE, autoimmune hemolytic anemia | - |
| Renal | Nephrolithiasis (oxalate stones in CD, urate stones), fistulas to bladder | - |
| Nutrition | Malnutrition, vitamin D deficiency, osteoporosis | - |
Primary sclerosing cholangitis is strongly associated with UC (present in ~5% of UC patients) and is independent of colitis activity.
7. Diagnosis
Diagnosis requires integration of clinical history, endoscopy, histopathology, radiology, and labs. No single finding is absolutely diagnostic.
Laboratory Findings
- Anemia: from chronic disease, blood loss, or deficiencies of iron, folate, or B12 (ileal disease)
- Leukocytosis: mild = active disease; marked = abscess or suppurative complication
- ESR and CRP: nonspecific inflammatory markers used to monitor activity; CRP correlates well with clinical and endoscopic activity in CD
- Fecal calprotectin: pooled sensitivity 88%, specificity 73% vs. endoscopically active IBD; UC specificity (79%) > CD (67%); useful for distinguishing IBD from IBS and monitoring treatment response
- Fecal lactoferrin: also a sensitive marker of intestinal inflammation
- Hypoalbuminemia: marker of malnutrition and active disease
- Vitamin B12: reduced if >100 cm of terminal ileum is diseased or resected
Serologic Markers
- ASCA (Anti-Saccharomyces cerevisiae antibodies): positive in 40-70% of CD, <15% of UC
- pANCA (perinuclear antineutrophil cytoplasmic antibody): positive in 55% of UC, 20% of CD (mainly colonic)
- ASCA+/pANCA- combination: sensitivity 55%, specificity 93% for CD
- Additional antibodies (anti-I2, anti-Cbir1, anti-OmpC) are associated with CD
Radiology
- CT enterography / MR enterography: have replaced barium studies as standard imaging; excellent for extent of disease, strictures, fistulas, abscesses, and perianal disease
- MRI enterography is preferred in younger patients and for monitoring (no radiation)
- The "comb sign" on MRI (engorged peri-enteric vasculature around the inflamed bowel) is characteristic of active CD
Activity Scoring
-
Crohn Disease Activity Index (CDAI): remission = CDAI <150; response = reduction ≥100 points. Components include stool frequency, abdominal pain, well-being, complications, use of antidiarrheal drugs, abdominal mass, hematocrit, and body weight.
-
Symptoms alone do not always correlate with objective mucosal inflammation; mucosal healing (endoscopic + biomarker-based) has emerged as a primary therapeutic target.
-
Goldman-Cecil Medicine, p. 1599-1606; Sleisenger & Fordtran, p. 2318
8. Treatment
Drug Classes
1. Aminosalicylates (5-ASA)
- Sulfasalazine and mesalamine are the backbone of mild-moderate UC treatment
- Oral mesalamine (4 g/day) + topical mesalamine enemas for distal-to-extensive UC
- Response rates ~45-55% for mild-moderate UC
- Not clearly effective for small bowel Crohn disease alone; sulfasalazine helps ileocolonic/colonic CD
2. Corticosteroids
- Oral prednisone (40-60 mg/day) for moderate-severe flares - not for maintenance
- Budesonide (9 mg/day enteric-coated): ~70% response for distal ileal/right colonic CD with fewer systemic effects
- IV corticosteroids (methylprednisolone/hydrocortisone) for hospitalized severe disease
- Patients not responding within 3-5 days of IV steroids should be considered for rescue therapy (infliximab or cyclosporine in UC; infliximab or surgery in CD)
3. Immunomodulators (Antimetabolites)
- Azathioprine (2.5 mg/kg/day) and 6-mercaptopurine: used for maintenance; not for rapid induction (takes 3-6 months to work)
- Methotrexate: effective for maintaining remission in CD; preferred over azathioprine/6-MP in males under 35 due to lymphoma risk with thiopurines
- Risk of lymphoma with thiopurines - especially in young men
4. Anti-TNF-alpha Biologics
- Infliximab (chimeric mouse-human IgG1, IV): approved for moderate-severe CD and UC, fistulizing CD, and CD/UC with high-risk prognostic indicators. Dosing: 5 mg/kg at weeks 0, 2, 6, then every 8 weeks.
- Adalimumab (fully human IgG1, SC): approved for moderate-severe CD and UC
- Golimumab (fully human IgG1, SC): approved for UC
- Certolizumab pegol (pegylated Fab fragment IgG4, SC): approved for CD
- Combination of infliximab + azathioprine is more effective than either alone for CD induction and maintenance
- Early "top-down" anti-TNF therapy based on biomarkers (fecal calprotectin ≥250 μg/g, CRP ≥5 mg/L) yields better clinical and endoscopic outcomes than purely symptom-driven decisions
5. Anti-Integrin Biologics
- Vedolizumab (anti-α4β7 integrin): gut-selective, used for moderate-severe CD and UC refractory to other therapies
- Natalizumab (anti-α4 integrin): reserved for refractory CD due to risk of progressive multifocal leukoencephalopathy (PML) from JC virus; requires strict TOUCH prescribing program
6. Anti-IL-12/23 Biologics
- Ustekinumab (anti-p40 subunit of IL-12 and IL-23, IV induction then SC maintenance): effective for moderate-severe CD and UC
- Risankizumab (anti-IL-23 p19): approved for CD and UC
7. JAK Inhibitors (Small Molecules - Oral)
- Upadacitinib (selective JAK inhibitor): approved for moderate-severe UC; induction 45 mg once daily x 8 weeks, then maintenance 15-30 mg once daily
- Tofacitinib: approved for UC; rapid onset; carries cardiovascular and VTE risk warnings
Treatment Algorithms
Mild-Moderate UC:
- Mesalamine (oral + topical) → corticosteroids for flares → immunomodulators or biologics for steroid-dependent/refractory disease
Mild-Moderate CD (ileocolonic/colonic):
- Sulfasalazine or budesonide → escalate to immunomodulators or anti-TNF
Moderate-Severe CD:
- Anti-TNF ± antimetabolite (combination superior to monotherapy) OR ustekinumab OR vedolizumab
- Meta-analysis: adalimumab, infliximab + azathioprine, or ustekinumab are the three most effective therapies for induction and maintenance of CD remission
Severe CD (hospitalized):
- NPO + IV fluids + parenteral corticosteroids
- If no response in 3-5 days: infliximab or surgery
Acute Severe UC (hospitalized):
-
IV corticosteroids (methylprednisolone 60 mg/day or hydrocortisone 400 mg/day)
-
If no response in 3-5 days: rescue therapy with infliximab or cyclosporine (IV), or colectomy
-
Goldman-Cecil Medicine, p. 1700-1760
9. Surgical Management
Ulcerative Colitis
- Surgery (total proctocolectomy) is curative for UC - unlike CD
- Indications: acute severe UC refractory to medical therapy, toxic megacolon, perforation, dysplasia/cancer, medically refractory disease
- The preferred procedure is total proctocolectomy with ileal pouch-anal anastomosis (IPAA/J-pouch)
- Pouchitis (inflammation of the J-pouch) occurs in ~50% of patients long-term; treated with antibiotics (metronidazole, ciprofloxacin)
Crohn Disease
- Surgery is not curative (disease recurs at the anastomosis in >50% within 10 years)
- Indications: obstruction, abscess, fistula refractory to treatment, medically refractory disease, perforation, cancer
- Conservative resection with strictureplasty preferred over wide resections to preserve bowel length and prevent short bowel syndrome
10. Colorectal Cancer Risk
IBD confers a substantially increased risk of colorectal cancer (CRC):
- UC: risk begins after ~7 years of disease; rises ~10% per decade; up to 34% at 30 years (tertiary center data); recent population studies suggest CRC risk may be declining
- Risk correlates with disease duration and extent (pancolitis > left-sided > proctitis)
- CD ileocolitis: CRC risk 4-20x the general population; mucinous carcinomas are common; often arise in bypassed or strictured segments
Surveillance colonoscopy is recommended starting 8-10 years after diagnosis, with biopsies every 1-2 cm throughout the colon. Dysplasia (low-grade or high-grade) detected on surveillance warrants consideration of colectomy (UC) or resection (CD).
- Sleisenger & Fordtran, p. 2617
11. Recent Evidence (2024-2026)
The 2024 American Gastroenterological Association evidence synthesis (PMID 39425738) performed a network meta-analysis on advanced therapies for moderate-to-severe UC, providing updated comparative efficacy data to guide biologic and small-molecule selection. A 2024 meta-analysis (PMID 39106167) updated the evidence on probiotics in IBD, finding limited efficacy for induction or maintenance of remission in CD, with some benefit in UC adjunctive therapy.
Summary Table: CD vs. UC at a Glance
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Location | Entire GI tract, any site | Colon only, rectum always |
| Pattern | Skip lesions | Continuous from rectum |
| Depth | Transmural | Mucosal |
| Hallmark complication | Fistula, stricture, abscess | Toxic megacolon, CRC |
| Smoking effect | Worsens | Improves |
| Surgery | Not curative | Curative |
| Characteristic histology | Noncaseating granuloma | Crypt distortion, no granulomas |
| Preferred serology | ASCA+ / pANCA- | pANCA+ / ASCA- |
| Key biologic target | TNF-α, IL-12/23, integrins | TNF-α, integrins, JAK |
Sources: Goldman-Cecil Medicine (26th ed.), Chapter 127 - Inflammatory Bowel Disease; Sleisenger and Fordtran's Gastrointestinal and Liver Disease (11th ed.), Chapters 115, 127.
This is a shared conversation. Sign in to Orris to start your own chat.